Pulmonary oedema
Reading File
Finding Sources
Searching PubMed
"pulmonary edema" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content across physiology, pathology, diagnosis, and treatment. I'll compose the full answer.
Pulmonary Oedema
Pulmonary oedema is defined as an excess of extravascular (interstitial and/or alveolar) lung water. It is a life-threatening condition that demands rapid recognition and treatment.
Pathophysiology
Fluid homeostasis in the lung follows Starling forces. Under normal conditions, pulmonary capillary hydrostatic pressure (~7 mmHg) is well below plasma colloid osmotic pressure (~28 mmHg), keeping the lungs dry. Lymphatics continuously drain small amounts of filtered fluid.
Oedema develops when any of the following tips the balance toward net fluid accumulation:
- Increased capillary hydrostatic pressure - exceeds plasma colloid osmotic pressure
- Increased capillary permeability - microvascular/epithelial injury
- Decreased plasma oncotic pressure - hypoalbuminaemia
- Lymphatic obstruction - rare but potent
Safety factor (Guyton): Pulmonary capillary pressure must rise to at least the level of colloid osmotic pressure (~25-28 mmHg) before significant oedema forms - giving an acute safety factor of ~21 mmHg. In chronic conditions (e.g., mitral stenosis), lymphatic expansion over 2 weeks can tolerate pressures up to 40-45 mmHg without lethal oedema. However, when capillary pressure exceeds the safety factor acutely, death may occur within 20-30 minutes if pressure rises 25-30 mmHg above that threshold. - Guyton and Hall Textbook of Medical Physiology
Classification & Causes
1. Cardiogenic (Haemodynamic) - High-pressure oedema
| Mechanism | Examples |
|---|---|
| Increased hydrostatic pressure | Left heart failure (most common), acute MI, hypertensive crisis, mitral stenosis/regurgitation, volume overload |
| Decreased oncotic pressure | Hypoalbuminaemia (nephrotic syndrome, liver disease, protein-losing enteropathy) |
| Lymphatic obstruction | Lymphangitic carcinomatosis |
2. Non-Cardiogenic (Increased Permeability) - Normal-pressure oedema
| Type | Examples |
|---|---|
| Direct lung injury | Bacterial pneumonia, inhaled toxins (chlorine, SO₂, smoke), aspiration of gastric contents, near-drowning, radiation, lung trauma |
| Indirect/systemic injury | Sepsis, burns, pancreatitis, major trauma (SIRS), blood transfusion-related (TRALI) |
| Drugs/toxins | Bleomycin, heroin, cocaine, methadone, amphotericin B, paraquat |
3. Uncertain Origin
- High-altitude pulmonary oedema (HAPE)
- Neurogenic pulmonary oedema (CNS trauma)
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathology
Acute cardiogenic: Alveolar capillaries are engorged; interstitial and alveolar spaces contain pale pink granular transudate on histology. Oedema accumulates first in basal regions of lower lobes (dependent pattern) due to hydrostatic effects.
Chronic cardiogenic: Haemosiderin-laden macrophages ("heart failure cells" - result of microhaemorrhages) are abundant. Over time, alveolar wall thickening and fibrosis produce "brown induration" of the lung - this reduces respiratory function and increases infection susceptibility.
Non-cardiogenic / ARDS: Injury to vascular endothelium or alveolar epithelium produces an inflammatory exudate. The histological pattern is diffuse alveolar damage (DAD). - Robbins
Clinical Features
Acute pulmonary oedema presents with:
- Dyspnoea at rest - rapid onset
- Tachypnoea and tachycardia
- Severe hypoxaemia
- Crackles (alveolar flooding) and wheeze (peribronchial cuffing compressing airways, "cardiac asthma")
- Hypertension from endogenous catecholamine release (common in acute decompensation)
- Frothy, blood-tinged sputum in severe cases
Symptoms of the underlying cause (chest pain in MI, fever in pneumonia, etc.) may accompany the above. - Harrison's Principles of Internal Medicine 22E
Investigations
| Test | Findings |
|---|---|
| CXR | Bilateral airspace opacification, interstitial shadowing, Kerley B lines, upper lobe blood diversion, cardiomegaly (cardiogenic), pleural effusions |
| ECG | ST elevation (acute MI), arrhythmias, LVH |
| BNP/NT-proBNP | Substantially elevated in heart failure; helps distinguish cardiogenic from non-cardiogenic |
| Echocardiography | Systolic/diastolic dysfunction, valvular lesions |
| Pulmonary artery catheter (PAC) | PCWP >18 mmHg = cardiogenic; normal PCWP = non-cardiogenic; indicated when aetiology uncertain or oedema refractory to treatment |
| ABG | Hypoxaemia, hypocapnia early; hypercapnia signals respiratory failure |
Chest X-ray Appearances
Serial CXRs show rapid fluctuation in airspace opacification over 48 hours, reflecting fluid shifts between intravascular compartment and air spaces:
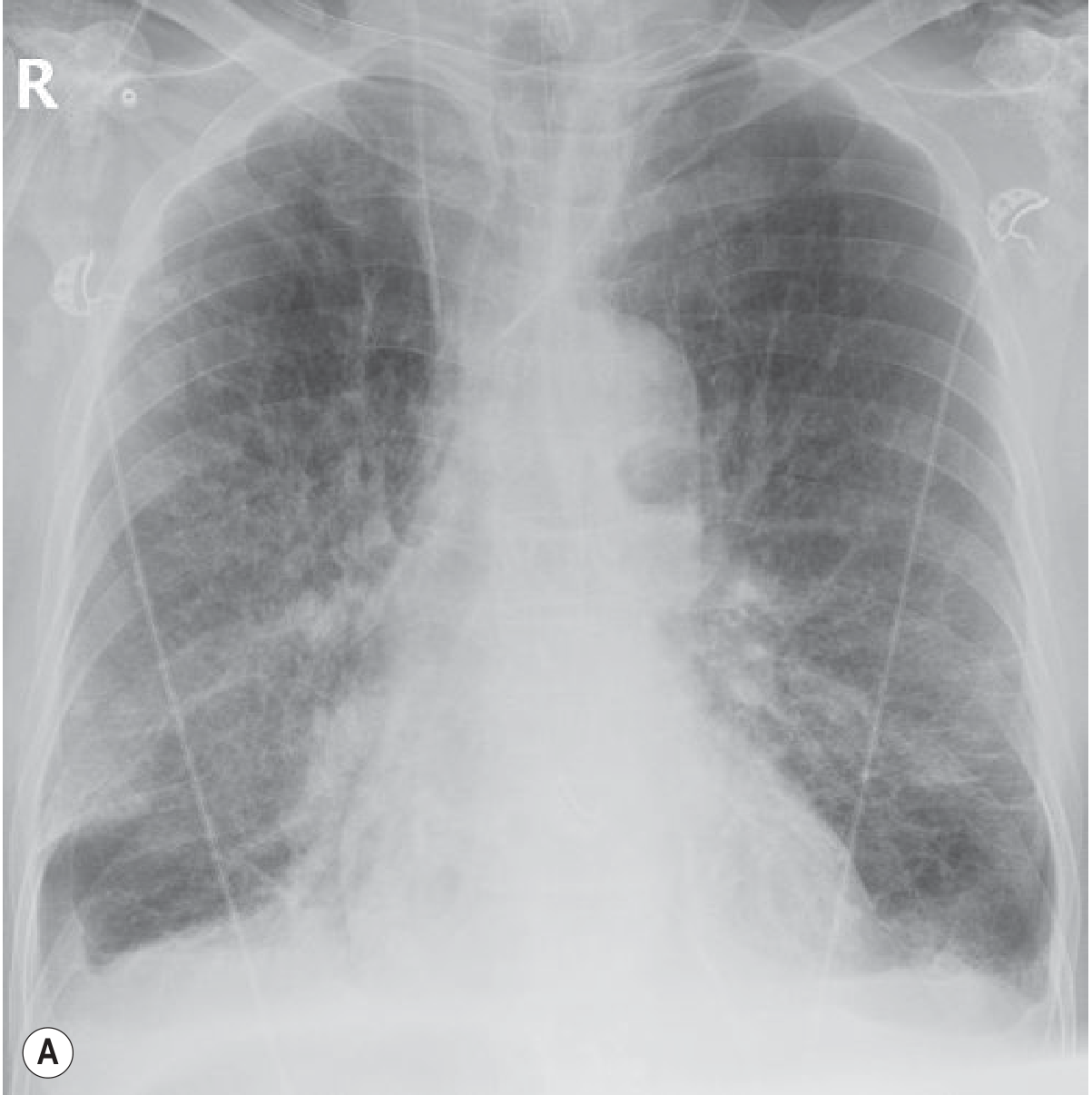

Serial chest radiographs over ~48 hours showing rapid fluctuation in airspace opacification - Grainger & Allison's Diagnostic Radiology
Treatment
Treatment depends on the underlying aetiology. Immediate priorities run in parallel: support oxygenation/ventilation, reduce preload, treat the precipitant, and manage complications (infection, acidaemia, anaemia, AKI).
1. Position
- Sit the patient upright, legs dangling (reduces venous return). - Harrison's
2. Oxygenation & Ventilation
| Modality | Notes |
|---|---|
| High-flow nasal cannula (HFNC) | Better outcomes than BiPAP for non-cardiogenic shock (non-CS) acute hypoxaemic failure with normal PaCO₂ |
| NIV (CPAP/BiPAP) | Rests respiratory muscles, improves oxygenation and cardiac function; reduces intubation need in cardiogenic pulmonary oedema |
| Mechanical ventilation with PEEP | For refractory cases. PEEP (1) decreases preload and afterload, (2) redistributes lung water from intraalveolar to extraalveolar space, (3) increases lung volume and prevents atelectasis |
| Target SpO₂ | ≥92% - very high saturation (>98%) may be detrimental |
- Harrison's 22E
3. Preload Reduction
| Agent | Key Points |
|---|---|
| Furosemide (loop diuretic) | First-line. Also acts as a venodilator, reducing preload before diuresis begins. Initial dose ≤0.5 mg/kg; higher (1 mg/kg) for renal insufficiency, chronic diuretic use, or hypervolaemia |
| Sublingual nitroglycerin | 0.4 mg × 3 every 5 min - first-line in acute cardiogenic oedema. Rapidly reduces preload and afterload |
| IV nitroglycerin | 5-10 µg/min if oedema persists without hypotension |
| IV nitroprusside | 0.1-5 µg/kg/min; potent venous and arterial vasodilator; useful with hypertension; avoid in reduced coronary perfusion states |
| ACE inhibitors | Reduce preload and afterload; recommended in hypertensive patients and acute MI with heart failure |
| Nesiritide (BNP) | Potent arterial/venous vasodilator with diuretic properties; reserved for refractory cases; avoid with ischaemia/MI |
4. Inotropes / Inodilators (when cardiac output is low)
| Agent | Notes |
|---|---|
| Dopamine / Dobutamine | Potent inotropic sympathomimetics |
| Milrinone | PDE-3 inhibitor (inodilator); 50 µg/kg bolus then 0.25-0.75 µg/kg/min; stimulates contractility + causes peripheral/pulmonary vasodilation |
| Digitalis glycosides | Rarely used now; useful for rate control in AF with LV dysfunction and pulmonary oedema |
5. Treat the Precipitant
- Acute MI - immediate revascularisation (PCI/thrombolysis)
- Arrhythmia - cardioversion if primary tachyarrhythmia
- Hypertensive emergency - IV vasodilators
- Sepsis / ARDS - treat underlying source, lung-protective ventilation
- Mitral stenosis - consider balloon valvuloplasty
6. Renal Replacement Therapy
- Consider in refractory volume overload, metabolic acidosis (pH <7.15-7.25), refractory hypoxaemia, or persistent hyperkalaemia
- Continuous renal replacement therapy (CRRT) preferred over intermittent HD if hypotensive or requiring inotropes
- In CKD patients with pulmonary oedema, dialysis is often the most rapidly effective intervention - Rosen's Emergency Medicine
7. Special Consideration - Iatrogenic Cardiogenic Shock
Vasodilator combinations in oedema treatment can cause hypotension and coronary hypoperfusion. Patients with hypertensive response to oedema tolerate and benefit most from vasodilators. - Harrison's 22E
Recent Evidence
A 2025 systematic review and meta-analysis (PMID 40506079) specifically examined low-dose vs. high-dose IV nitroglycerin in sympathetic crashing acute pulmonary oedema (SCAPO), an important area of active investigation.
Summary Mnemonic: LMNOP
A bedside aide-memoire for acute cardiogenic pulmonary oedema:
| Letter | Intervention |
|---|---|
| L | Lasix (furosemide) |
| M | Morphine (reduces anxiety/preload - note: evidence questioned in recent practice) |
| N | Nitrates (sublingual/IV GTN) |
| O | Oxygen (target SpO₂ ≥92%), NIV/CPAP |
| P | Position (upright, legs down) |
Sources: Guyton and Hall Textbook of Medical Physiology | Harrison's Principles of Internal Medicine 22E | Robbins, Cotran & Kumar Pathologic Basis of Disease | Grainger & Allison's Diagnostic Radiology | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.