emergency contraceptive pills
Reading File
Finding Sources
Finding Sources
Searching PubMed
"emergency contraception"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a complete overview:
Emergency Contraceptive Pills (ECPs)
Emergency contraception (EC) refers to methods used after unprotected or inadequately protected intercourse to prevent pregnancy. There are three oral regimens and one highly effective non-oral option.
Why It's Needed
The probability of pregnancy from a single act of unprotected intercourse varies with cycle timing:
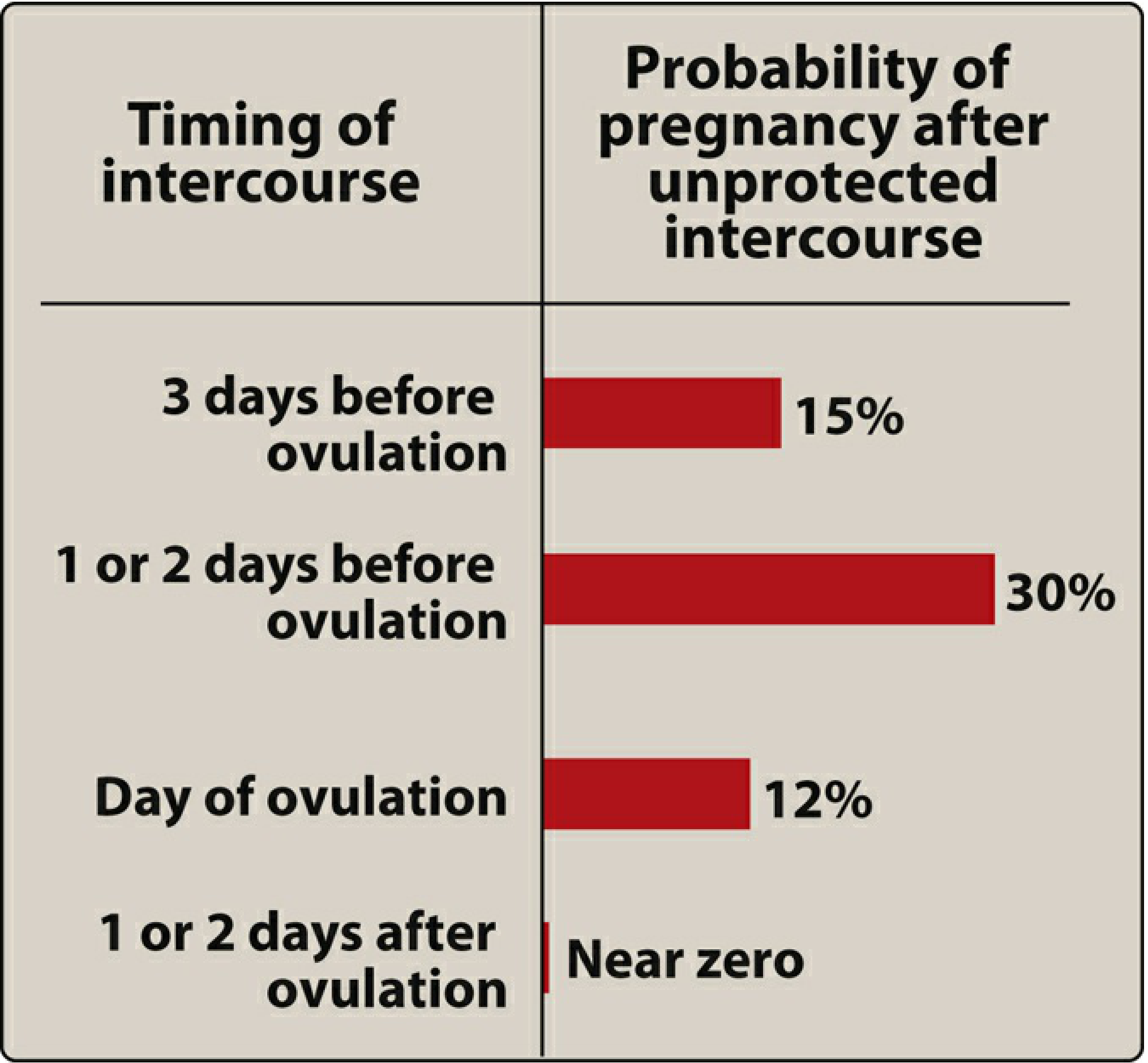
(Risk is highest 1–2 days before ovulation at ~30% — Lippincott Illustrated Reviews: Pharmacology)
Available Options
1. Levonorgestrel (Progestin-Only) — First-line OTC option
| Feature | Details |
|---|---|
| Dose | Single 1.5 mg dose or two 0.75 mg doses 12 h apart (single dose preferred) |
| Window | Up to 72 hours after intercourse (labeled); WHO allows up to 120 h |
| OTC status | Available without prescription (Plan B One-Step and generics) |
| Efficacy | Reduces pregnancy risk to ~1.1%; most effective in the first 24 h |
| Mechanism | Delays or inhibits ovulation; works only before ovulation occurs — not an abortifacient |
BMI consideration: Efficacy is significantly reduced in women with BMI >30 kg/m². Levonorgestrel levels are lower in obese women due to distribution volume; ulipristal is preferred in this population. — Berek & Novak's Gynecology
2. Ulipristal Acetate (ella) — Preferred when >72 hours or obese
| Feature | Details |
|---|---|
| Dose | Single 30 mg tablet |
| Window | Up to 120 hours (5 days) after intercourse |
| Rx status | Prescription only |
| Efficacy | At least as effective as LNG up to 72 h; superior beyond 72 h. Odds of pregnancy 42% lower at 72 h vs. LNG, 65% lower in first 24 h |
| Mechanism | Progesterone receptor modulator — inhibits LH release and blocks follicular rupture even near/at the LH surge |
Important drug interaction: Ulipristal is metabolized by CYP3A4. Inducers (rifampin, barbiturates, certain anticonvulsants) reduce its efficacy.
Starting hormonal contraception after UPA: Wait 5 days before initiating any hormonal method — combining desogestrel the day after ulipristal caused ovulation in 45% of cycles. Levonorgestrel-based EC has no such restriction; hormonal contraception can start immediately. — Berek & Novak's Gynecology
3. Combined Estrogen-Progestin (Yuzpe Regimen) — Largely obsolete
- Dose: 100 μg ethinyl estradiol + 0.5–1.0 mg levonorgestrel in two doses 12 hours apart
- Fallen out of favor due to high rates of nausea (50.5%) and vomiting (18.8%) vs. levonorgestrel alone (23.1% nausea, 5.6% vomiting)
- Pregnancy rate ~3.2% vs. 1.1% with LNG alone
Mechanism of Action — Key Clarification
Both LNG and ulipristal delay or inhibit ovulation. They do not terminate an established pregnancy. LNG is effective only if administered before ovulation; no pregnancies occur if taken 1–5 days before ovulation, but all 7 pregnancies in one study occurred when LNG was taken on the day of ovulation or later. — Berek & Novak's Gynecology
EC is not equivalent to medical abortion. It has not been shown to harm a developing fetus if taken during an established pregnancy.
Non-Oral Option: Copper IUD
Though not a pill, it is the most effective EC method and worth knowing:
- Insert within 5 days of intercourse → ~100% efficacy
- Mechanism: inhibits sperm function, fertilized egg transport, and implantation
- Risk: 1/1000 uterine perforation; uterine cramping
- Bonus: provides ongoing contraception for up to 10 years; 94% of patients continue using it at 12-month follow-up
Side Effects of Oral EC
| Effect | LNG | UPA | Yuzpe |
|---|---|---|---|
| Nausea | Moderate | Moderate | High (50%) |
| Vomiting | Low | Low | High (19%) |
| Headache | Yes | Yes (self-limited) | Yes |
| Irregular bleeding | Yes | Yes | Yes |
Irregular menstrual bleeding may occur within 1 week to 1 month but resolves without intervention.
Counseling Points
- Take as soon as possible — efficacy declines with time
- Still possible to become pregnant in the same cycle; use ongoing contraception
- If menstruation is delayed >3 weeks, perform a pregnancy test
- Follow-up pregnancy test if the next period is missed
- EC does not protect against sexually transmitted infections — condoms should always be used
Choosing the Right EC
| Situation | Recommended EC |
|---|---|
| ≤72 h, normal BMI | Levonorgestrel 1.5 mg OTC |
| >72 h but ≤120 h | Ulipristal 30 mg (Rx) |
| BMI >30 kg/m² | Ulipristal preferred over LNG |
| Wants ongoing contraception | Copper IUD (best efficacy overall) |
| On CYP3A4 inducers | Avoid ulipristal; use LNG or copper IUD |
Sources: ROSEN's Emergency Medicine; Berek & Novak's Gynecology; Lippincott Illustrated Reviews: Pharmacology; Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.