Teacg me how to manage a patient with dka
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetic ketoacidosis" AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative sources. Let me compile the full, detailed DKA management guide.
Management of Diabetic Ketoacidosis (DKA)
DKA is defined by the biochemical triad of hyperglycemia, ketonemia/ketonuria, and metabolic acidosis. Management involves simultaneous correction of fluid deficits, electrolyte imbalances, and insulin deficiency, plus identification and treatment of the precipitating cause.
1. Understanding DKA: Quick Pathophysiology
Insulin deficiency + glucagon excess drive three parallel processes:
- Hyperglycemia - reduced glucose uptake + increased hepatic glucose output → osmotic diuresis → dehydration
- Ketogenesis - unrestrained lipolysis → elevated free fatty acids → hepatic conversion to beta-hydroxybutyrate and acetoacetate → anion-gap metabolic acidosis
- Electrolyte depletion - osmotic diuresis flushes Na+, K+, Mg2+, phosphate, and Cl- into the urine (Table below)
Note: Serum K+ may appear normal or even elevated at presentation due to acidosis-driven extracellular K+ shift - but total body K+ stores are always depleted. This is a critical trap.
Average fluid and electrolyte deficits in severe DKA (Rosen's EM):
| Substance | Deficit |
|---|---|
| Water | 70-120 mL/kg |
| Sodium | 8-10 mEq/kg |
| Potassium | 5-7 mEq/kg |
| Chloride | 6-8 mEq/kg |
| Phosphorus | ~3 mEq/kg |
2. Diagnostic Criteria
The three defining features (Goldman-Cecil Medicine):
| Feature | Criteria |
|---|---|
| Hyperglycemia | Blood glucose >250 mg/dL (or known DM) |
| Ketosis | Urine ketones 2+ or more / serum ketones ≥3.0 mmol/L |
| Acidosis | Arterial/venous pH <7.3 and/or serum bicarbonate <18 mmol/L |
DKA Severity Classification:
| Mild | Moderate | Severe | |
|---|---|---|---|
| pH | 7.25-7.30 | 7.00-7.24 | <7.00 |
| Bicarbonate | 15-18 | 10-<15 | <10 |
| Mental status | Alert | Drowsy | Stupor/coma |
Important lab caveats:
- Serum K+ may be falsely elevated - always check before giving insulin
- Nitroprusside ketone tests detect acetoacetate only, NOT beta-hydroxybutyrate (the predominant ketone in DKA) - so they may underestimate severity early in treatment
- Serum amylase is often elevated in DKA without true pancreatitis - use lipase (must be >3x ULN for pancreatitis diagnosis)
- Leukocytosis reflects the degree of ketosis, not necessarily infection - band neutrophilia is the more reliable infection marker
- Serum creatinine may be falsely elevated on autoanalyzer
3. Common Precipitants
(Goldman-Cecil Medicine)
Most Common:
- Infections (most frequent)
- Inadequate insulin / non-adherence to therapy
- New-onset diabetes (~25% of DKA episodes)
- Acute coronary syndrome
Other Causes:
- Cerebrovascular accident, pulmonary embolism, acute pancreatitis
- Drugs: corticosteroids, SGLT2 inhibitors (euglycemic DKA!), clozapine, olanzapine, cocaine, lithium
- Endocrinopathies: Cushing syndrome, thyrotoxicosis, acromegaly
- Severe burns, hyperthermia/hypothermia
SGLT2 inhibitor-associated DKA is a special case - blood glucose may be only mildly elevated (euglycemic DKA), making diagnosis easy to miss. The medication's effect persists 10-14 days after stopping.
4. Initial Assessment
History: Polyuria, polydipsia, polyphagia, weight loss, weakness, nausea/vomiting, abdominal pain (50% of patients, especially children). Abdominal pain in adults more often signals a true intra-abdominal precipitant.
Examination: Kussmaul breathing (deep rapid respirations - respiratory compensation for acidosis), tachycardia, hypotension/orthostatic changes, dry mucous membranes, acetone odor on breath, altered mental status.
Fever is NOT caused by DKA itself - its presence should prompt a search for an infectious precipitant.
Workup:
- Serum glucose, electrolytes (Na, K, Cl, HCO3), BUN, creatinine
- Arterial or venous blood gas
- Serum/urine ketones (or point-of-care beta-hydroxybutyrate)
- CBC with differential
- Urinalysis and urine culture
- Blood cultures if infection suspected
- ECG (to assess for ACS as precipitant and to monitor K+ effects)
- Chest X-ray
- Calculate anion gap: Na - (Cl + HCO3); normal = 8-12
5. Treatment: The Four Pillars
Pillar 1: Fluid Resuscitation
This is the first priority, before insulin.
- Start with 0.9% Normal Saline (NS)
- Rate: 1-2 L over the first 1-2 hours (or 15-30 mL/kg in the first hour)
- Continue NS at 250-500 mL/h thereafter, guided by vital signs and urine output
- Total fluid deficit is typically 4-10 liters
- In children: 20 mL/kg NS in the first hour
Do NOT give insulin before adequate fluid resuscitation in very dehydrated patients - insulin-mediated glucose uptake moves water out of the intravascular space, which can precipitate cardiovascular collapse.
When to switch fluids:
- Once blood glucose falls to ≤250-300 mg/dL → switch to D5W/0.45% NS (or add dextrose to ongoing NS) to allow insulin to continue without causing hypoglycemia
Pillar 2: Potassium Replacement
This is the most critical electrolyte management step in DKA.
| Serum K+ | Action |
|---|---|
| <3.3 mEq/L | Hold insulin - give IV KCl aggressively first (20-40 mEq/h) until K+ ≥3.3 |
| 3.3-5.5 mEq/L | Add 20-40 mEq KCl to each liter of IV fluid; start insulin |
| >5.5 mEq/L | Hold potassium; recheck in 1-2 hours |
- Continuous cardiac monitoring is required when K+ replacement rate exceeds 10 mEq/h
- Recheck K+ every 1-2 hours during treatment
- Ensure adequate urine output (>0.5 mL/kg/h) before adding potassium to fluids
Pillar 3: Insulin Administration
- Do NOT start insulin until K+ ≥3.3 mEq/L (risk of fatal cardiac arrhythmia)
- Mild-moderate DKA: Can be treated with subcutaneous rapid-acting insulin analogs
- Severe DKA: Requires IV regular insulin
IV Insulin Protocol (standard):
- Option A: Start IV infusion at 0.1 units/kg/hour (no bolus)
- Option B: Give 0.1 units/kg IV bolus, then infusion at 0.1 units/kg/hour
- If blood glucose does NOT fall by ≥10% in the first hour → give 0.1 units/kg IV bolus
Titration:
- Target glucose decline: ~50-75 mg/dL/hour
- When glucose reaches 250 mg/dL: add dextrose to IV fluids AND reduce insulin infusion to 0.05 units/kg/hour
- Goal is to keep glucose ~150-200 mg/dL while continuing insulin until ketoacidosis clears
Transition to subcutaneous insulin:
- Only transition when DKA has resolved: pH >7.3, HCO3 >15, ketones cleared, patient tolerating oral intake
- Overlap IV insulin with the first subcutaneous dose by 1-2 hours before discontinuing the infusion (to prevent relapse)
Pillar 4: Identify and Treat the Precipitant
- Review history, cultures, ECG, imaging
- Treat infection with appropriate antibiotics
- Address MI, PE, or other acute illness
6. Other Electrolytes and Bicarbonate
Phosphate:
- Routine phosphate replacement is not recommended in most patients
- Consider replacement if severe hypophosphatemia develops (risk of respiratory muscle weakness)
Magnesium:
- Correct if low: 1-2 g MgSO4 IV
- Note: serum Mg may not reflect true body stores
Bicarbonate:
- Routine use is not recommended - multiple studies show no benefit in resolution of acidosis or time to discharge
- Only consider if: pH <6.9, or hemodynamic instability with pH <7.1
- Give 100 mEq NaHCO3 in 400 mL sterile water IV over 2 hours if criteria met
7. Monitoring During Treatment
Keep meticulous flow sheets tracking:
| Parameter | Frequency |
|---|---|
| Vital signs, mental status | Every 1-2 hours |
| Blood glucose | Every 1-2 hours (or continuous) |
| Serum K+, electrolytes | Every 2-4 hours |
| Venous pH / HCO3 | Every 2-4 hours |
| Fluid input and urine output | Hourly |
| Anion gap | Every 2-4 hours |
8. Resolution Criteria
DKA is resolved when ALL of the following are met:
- Blood glucose <200-250 mg/dL
- Serum bicarbonate ≥15-18 mEq/L
- Venous pH >7.30
- Anion gap normalized (<12)
- Ketonemia resolved (or beta-hydroxybutyrate <1.0 mmol/L)
9. Complications to Watch For
| Complication | Notes |
|---|---|
| Cerebral edema | Most feared in children; presents with headache, altered consciousness, bradycardia; treat with mannitol or hypertonic saline |
| Hypokalemia | From insulin + fluid therapy shifting K+ intracellularly; can cause arrhythmias |
| Hypoglycemia | From excessive insulin; prevented by adding dextrose when glucose reaches 250 mg/dL |
| Hypophosphatemia | Can impair ventilation from respiratory muscle weakness |
| Venous thrombosis | DKA increases coagulability |
| ARDS | Rare but serious complication |
| Hyperchloremic acidosis | From large volumes of NS; the anion gap resolves but non-gap acidosis persists |
10. DKA vs. Alcoholic Ketoacidosis (Important Differential)
- Alcoholic KA occurs in malnourished alcoholics after acute intoxication
- Patient is euglycemic or hypoglycemic (NOT hyperglycemic)
- Predominant ketone is beta-hydroxybutyrate - nitroprusside test may be weakly positive, underestimating severity
- Treatment is dextrose + IV fluids - NOT insulin
Recent Evidence (2024-2026)
A 2024 meta-analysis (PMID 39090718) comparing subcutaneous insulin vs. continuous IV insulin infusion in adult DKA found no significant difference in clinical outcomes, supporting that subcutaneous insulin analogs are a valid option for mild-moderate DKA and may reduce ICU admissions.
A 2026 systematic review (PMID 41208563) examined early subcutaneous basal insulin co-administered with IV insulin infusion in DKA, finding it reduces DKA recurrence and shortens ICU length of stay - this "basal-bolus overlap" strategy is gaining traction.
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 9e - Ch. 115
- Goldman-Cecil Medicine International Edition, 2-Volume Set - Ch. 210
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Ch. 47 (Table 47-14)
Great Now teacg me how to calculate dose of pottasium in pottasium deficit in a case of hypokalemia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough, well-illustrated answer. Here is the complete teaching guide:
Potassium Deficit Calculation and Replacement in Hypokalemia
The Core Concept: Why Simple Serum Math Fails
Potassium is overwhelmingly an intracellular cation - about 98% of the body's ~3,500 mEq total potassium lives inside cells, and only ~2% is extracellular. This has a critical implication:
A low serum K+ dramatically underestimates the true total body deficit because cells shift K+ outward to buffer the extracellular loss.
As Barash's Clinical Anesthesia puts it: "It is deceiving to think that 10 to 30 mEq of potassium will correct low potassium levels... a plasma potassium deficit is indicative of a far greater intracellular deficit."
The Rule of Thumb Formula (Rosen's Emergency Medicine)
This is the most widely used bedside estimate:
Each 0.3 mEq/L drop in serum K+ below normal corresponds to approximately 100 mEq total body deficit
Normal serum K+ = 4.0 mEq/L
So:
| Serum K+ (mEq/L) | Drop from normal | Estimated Total Body Deficit |
|---|---|---|
| 3.7 | 0.3 | ~100 mEq |
| 3.4 | 0.6 | ~200 mEq |
| 3.1 | 0.9 | ~300 mEq |
| 2.8 | 1.2 | ~400 mEq |
| 2.5 | 1.5 | ~500 mEq |
| 2.0 | 2.0 | ~667 mEq |
| 1.5 | 2.5 | ~833 mEq |
Formula written out:
Estimated K+ Deficit (mEq) = [(4.0 − measured K+) ÷ 0.3] × 100
Worked Example:
- Patient's serum K+ = 2.8 mEq/L
- Drop = 4.0 − 2.8 = 1.2 mEq/L
- Estimated deficit = (1.2 ÷ 0.3) × 100 = 400 mEq
The Exponential Relationship - Why Deficit Grows Non-Linearly
The graph below (from Comprehensive Clinical Nephrology) illustrates why mild hypokalemia hides massive total body deficits:
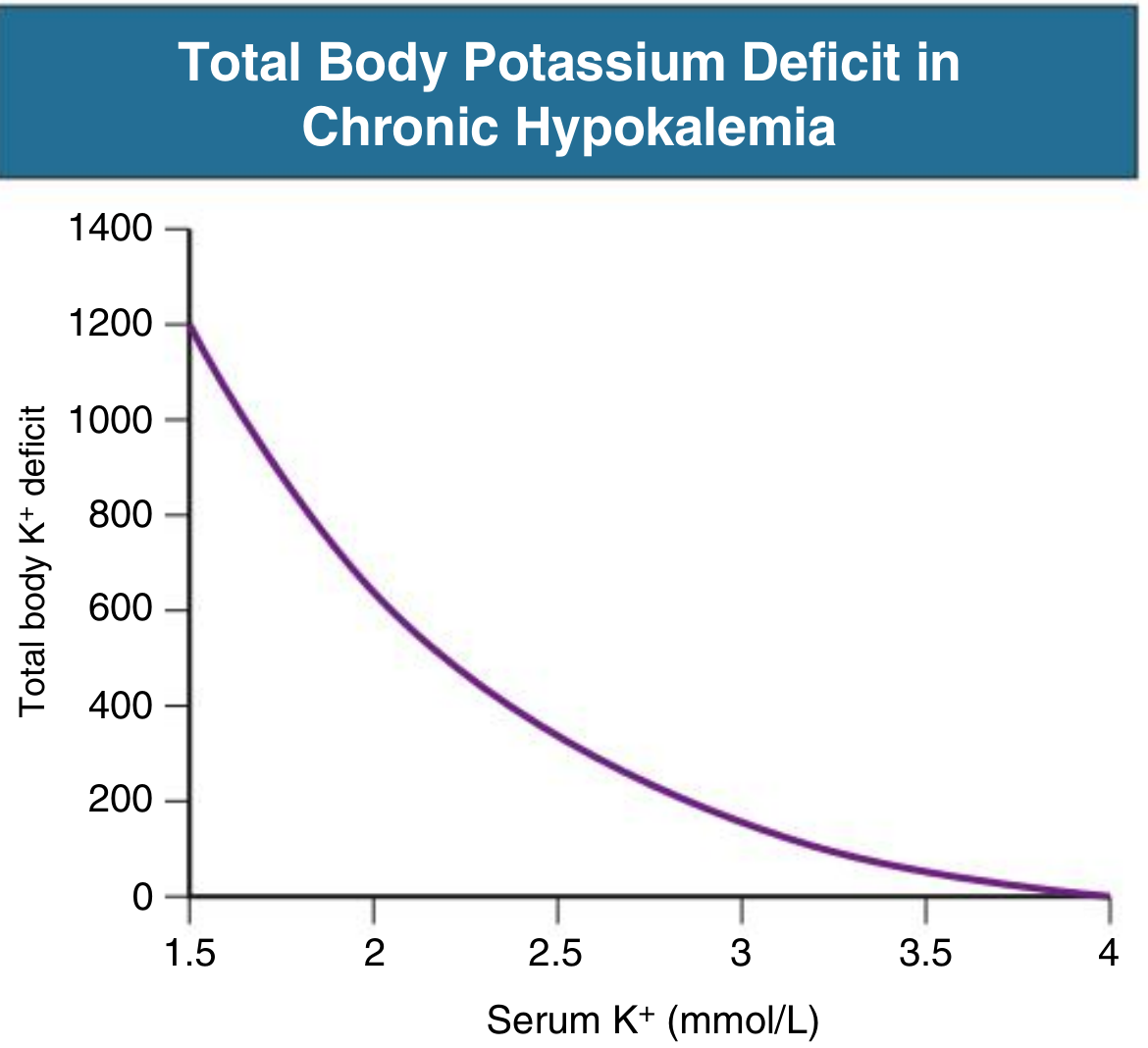
The curve steepens sharply as serum K+ falls below 2.5 mEq/L. At a serum K+ of ~1.5 mEq/L, the total body deficit can exceed 1,200 mEq - yet the serum only shows a 2.5 mEq/L drop.
Why the curve, not a straight line?
- During chronic depletion, cells release more K+ to maintain ECF K+ - this "buffering" masks the true deficit
- As K+ falls further, the cellular buffer is exhausted, and small additional losses cause steep serum drops
- During replacement, K+ shifts back INTO cells, so you must give much more than the serum change suggests
Severity Classification
| Severity | Serum K+ (mEq/L) | Clinical Features |
|---|---|---|
| Mild | 3.0-3.5 | Often asymptomatic, fatigue, muscle cramps |
| Moderate | 2.5-3.0 | Weakness, ECG changes (T-wave flattening, U-waves) |
| Severe | <2.5 | Paralysis, ileus, arrhythmias (torsades de pointes) |
| Critical | <2.0 | Life-threatening paralysis, respiratory failure, VF |
Route of Replacement: Oral vs. IV
Oral Replacement (Preferred when tolerated)
- Safer - gut sensors blunt acute rises in serum K+, making acute hyperkalemia extremely rare
- Standard regimen: 40-60 mEq orally every 2-4 hours (Rosen's EM)
- Safe total daily dose: up to 60-80 mEq/day in mild cases (Morgan & Mikhail)
- Use KCl as the preferred salt (also corrects common co-existing metabolic alkalosis and chloride deficit)
- Takes days to correct large deficits - plan for ongoing supplementation
IV Replacement (For severe/symptomatic cases)
Use IV when:
- Patient cannot tolerate oral intake (vomiting, post-op, altered consciousness)
- Severe hypokalemia (<2.5 mEq/L) with ECG changes or arrhythmias
- Hypokalemia causing respiratory compromise
- Pre-operative with K+ <3.0 mEq/L
- Acute MI with ventricular ectopy
IV KCl Rate Guidelines:
| Clinical Situation | Max Rate | Access Needed | Monitoring |
|---|---|---|---|
| Standard / routine | 10 mEq/hr | Peripheral IV | Periodic ECG |
| Moderate urgency | 10-20 mEq/hr | Peripheral IV (at 20 mEq/hr, central preferred) | Continuous ECG |
| Life-threatening (paralysis, K+ <2.0, QT >500ms) | 5-10 mEq over 15-20 min, repeatable | Central line | Continuous ECG |
| Maximum daily IV dose | 240 mEq/day | - | - |
Peripheral IV ceiling = 8-10 mEq/hr due to K+'s irritative effect on veins. Faster rates require a central line.
Critical Practical Points
1. Never use dextrose-containing solutions (D5W) as the diluent for KCl
The glucose causes insulin secretion, which drives K+ into cells - this can worsen hypokalemia paradoxically. Always dilute KCl in normal saline or 0.45% saline.
2. Always check and replace Magnesium
Hypokalemia and hypomagnesemia almost always coexist. If magnesium is low, K+ replacement will fail - Mg2+ is required for K+ to move intracellularly and for the Na/K-ATPase pump to function. Unless the patient receives at least 0.5 g/hr of MgSO4 alongside KCl, potassium will not shift intracellularly and will continue to be lost in the urine. (Rosen's EM)
Treat hypomagnesemia first (or simultaneously): 1-2 g MgSO4 IV
3. The goal of IV therapy is to remove from danger, not fill the tank
IV KCl is not intended to correct the entire 200-600+ mEq deficit at once. The goal is to get the patient out of the danger zone (K+ ≥3.0, or ≥3.5 in ACS/heart failure), then switch to oral supplementation over days.
4. Recheck frequently - the deficit is dynamic
After each 40-60 mEq IV infusion, recheck serum K+. Due to the intracellular shift during repletion, rises are often slower than expected.
5. Correct the underlying cause
If renal K+ wasting continues (diuretics, hyperaldosteronism, RTA), replacement alone will fail. Measure a spot urine K+/creatinine:
- >13 mEq/g creatinine = inappropriate renal wasting → search for renal/endocrine cause
- <13 mEq/g creatinine = adequate renal conservation → GI loss or redistribution more likely
6. Target K+ levels by population
| Population | Target Serum K+ |
|---|---|
| General | ≥3.5 mEq/L |
| Heart failure | 4.0-5.0 mEq/L |
| Post-MI / high arrhythmia risk | 4.0-5.0 mEq/L |
| Digoxin therapy | >4.0 mEq/L (risk of digoxin toxicity) |
Preferred Potassium Salt by Context
| Co-existing condition | Preferred K+ Salt |
|---|---|
| Metabolic alkalosis (most common) | KCl - corrects both K+ and Cl- deficit |
| Metabolic acidosis | K+ bicarbonate / K+ acetate / K+ citrate |
| Hypophosphatemia (e.g., DKA) | K+ phosphate |
Discharge Criteria (Rosen's EM)
Do NOT discharge until:
- K+ >3.0 mEq/L
- Patient tolerating oral food and fluids
- QTc <500 ms
- Underlying cause identified or treatable outpatient
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 9e - Ch. 115
- Comprehensive Clinical Nephrology, 7th Edition - Ch. 10 (Fig. 10.5)
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Ch. 49
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Ch. 47
How do I recognize and manage hyperkalemia (the opposite problem)?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed. Here is the complete guide:
Recognition and Management of Hyperkalemia
Definition and Severity
| Severity | Serum K+ (mEq/L) |
|---|---|
| Mild | 5.5-6.0 |
| Moderate | 6.0-7.0 |
| Severe | >7.0 |
| Critical | >8.0, or any level with ECG changes |
Normal serum K+ = 3.5-5.0 mEq/L. Hyperkalemia begins at >5.0-5.5 mEq/L depending on the source.
Step 1: Rule Out Pseudohyperkalemia FIRST
The most common cause of an elevated K+ result is a spurious/false elevation. Always consider this before treating.
| Cause | Mechanism |
|---|---|
| Hemolyzed blood sample | RBC lysis releases intracellular K+ into the tube |
| Marked leukocytosis (WBC >70,000 x 10⁹/L) | WBCs release K+ in vitro after sampling |
| Marked thrombocytosis (platelets >1,000,000 x 10⁹/L) | Platelets release K+ during clotting |
| Sample drawn near a K+-containing IV line | Contamination of specimen |
Action: If no ECG changes and no clinical features, repeat the sample before treating. Get an ECG simultaneously.
Step 2: Recognize - Clinical Features
Symptoms
- Muscle weakness (usually K+ >6.0-7.0 mEq/L)
- Paralysis (K+ >8.0 mEq/L)
- Palpitations, bradycardia
- Nausea, fatigue
- Importantly: Hyperkalemia is often clinically silent until it causes life-threatening cardiac events
A patient with CKD in cardiac arrest should be presumed hyperkalemic and treated empirically while resuscitation proceeds. (Rosen's EM)
ECG Changes - The Hallmark of Severity
The ECG progression follows a predictable sequence with rising K+:
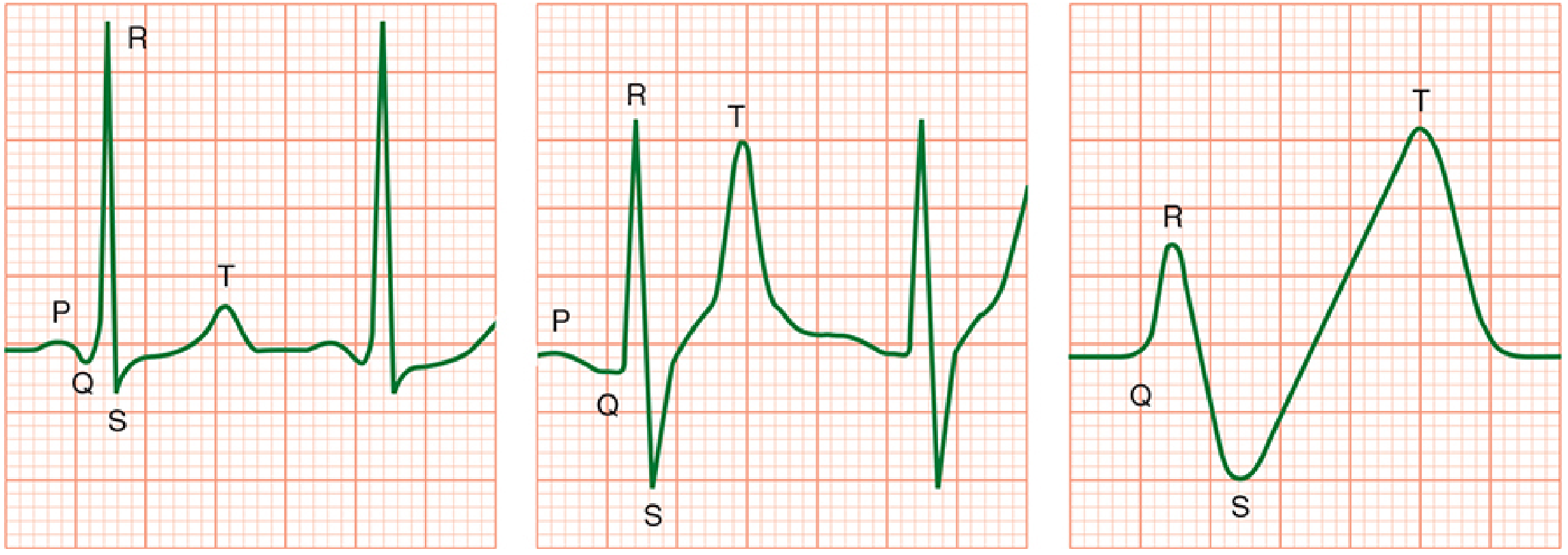
| ECG Change | Typical K+ Level | Clinical Significance |
|---|---|---|
| Peaked, narrow, symmetric T waves (shortened QT) | 5.5-6.5 mEq/L | First sign - narrow base distinguishes from benign T-wave changes |
| Prolonged PR interval, flattened P waves | 6.5-7.5 mEq/L | AV conduction slowing |
| Loss of P wave | >7.0 mEq/L | Sinoatrial block |
| Wide QRS (>0.12s) | 7.0-8.0 mEq/L | Ventricular conduction delay - danger zone |
| Sine wave pattern (QRS-T merge) | >8.0 mEq/L | Pre-terminal - imminent arrest |
| VF / Asystole | >8-9+ mEq/L | Cardiac arrest |
Critical points about ECG:
- ECG changes may be completely absent even with severe hyperkalemia - a normal ECG does NOT rule out dangerous K+ levels
- Hypocalcemia, hyponatremia, and acidosis each worsen the cardiac toxicity at any given K+ level
- Any patient with K+ ≥6.5 mEq/L must be managed aggressively regardless of ECG
Step 3: Common Causes
(Morgan & Mikhail, Rosen's EM)
The 5 most common causes:
- Spurious (hemolysis, WBC/platelet release - most common)
- Renal failure (acute or chronic - impaired excretion)
- Acidosis - H+/K+ exchange shifts K+ out of cells (DKA, Addison's, type 4 RTA)
- Cell death - K+ released from destroyed cells (rhabdomyolysis, tumor lysis syndrome, massive hemolysis, crush injury, burns)
- Drugs - ACE inhibitors, ARBs, K+-sparing diuretics (spironolactone, amiloride, triamterene), NSAIDs, trimethoprim, pentamidine, succinylcholine, digoxin toxicity, K+ supplements
Step 4: Management - The Three-Stage Framework
(Harrison's Principles of Internal Medicine 22e, 2025)
The treatment of hyperkalemia follows three sequential, overlapping stages:
Stage 1: Stabilize the Cardiac Membrane (Immediate)
Goal: Protect the heart NOW. Does NOT lower K+ levels.
When to use: Any ECG changes, K+ ≥6.5, or hemodynamic instability.
Calcium Gluconate or Calcium Chloride:
| Agent | Dose | Route | Onset | Duration |
|---|---|---|---|---|
| 10% Calcium Gluconate | 10 mL IV over 2-3 min | Peripheral IV (safer for veins) | 1-3 min | 30-60 min |
| 10% Calcium Chloride | 3-4 mL IV over 2-3 min | Central line preferred (caustic) | 1-3 min | 30-60 min |
- Calcium raises the action potential threshold, restoring the gap between resting and threshold potentials without changing the resting membrane potential - it reverses depolarization blockade
- Repeat the dose if ECG does not improve within 5 min, or if changes recur
- Special warning - Digoxin patients: Calcium potentiates digoxin toxicity. If calcium is judged absolutely necessary in a patient on digoxin, dilute 10 mL of 10% calcium gluconate in 100 mL D5W and infuse slowly over 20-30 min to avoid acute hypercalcemia
Stage 2: Shift K+ Into Cells (Rapid - buys time)
Goal: Lower serum K+ temporarily (hours). Does NOT remove K+ from the body.
A. Insulin + Glucose (first-line shifter)
- Give: 10 units IV regular insulin + 50 mL of 50% dextrose (25 g glucose) IV
- Onset: 10-20 min; Peak: 30-60 min; Duration: 4-6 hours
- Lowers K+ by ~0.5-1.0 mEq/L
- Do NOT give D50W alone (hypertonic glucose raises osmolality → osmotic K+ shift OUT of cells → worsens hyperkalemia)
- Follow with 10% dextrose infusion at 50-75 mL/h to prevent hypoglycemia (very common complication)
- If patient is already hyperglycemic (glucose ≥200-250 mg/dL): give insulin without glucose
B. Inhaled Beta-2 Agonists (Albuterol) - additive to insulin
- Dose: 10-20 mg nebulized albuterol in 4 mL NS, inhaled over 10 min
- Onset: ~30 min; Peak: ~90 min; Duration: 2-6 hours
- Lowers K+ by ~0.5-1.5 mEq/L
- Additive effect with insulin - use together for severe hyperkalemia
- Caution: ~20% of ESRD patients are resistant to beta-2 agonists - never use alone without insulin
- Side effects: tachycardia, hyperglycemia; use with caution in cardiac disease
C. Sodium Bicarbonate (limited acute role)
- IV bicarbonate has no role as a rapid acute treatment of hyperkalemia
- It may slowly attenuate hyperkalemia over 4-6 hours of isotonic infusion
- Useful primarily when metabolic acidosis co-exists (delayed K+ drop as acidosis corrects)
- Give as: 150 mEq NaHCO3 in 1 L D5W (isotonic), NOT as bolus ampules (risk of hypernatremia/hypertonicity)
- Do NOT give as repeated hypertonic boluses
Stage 3: Remove K+ From the Body (Definitive)
Goal: Actually eliminate K+ from the body. Required for definitive treatment.
A. Loop Diuretics (Furosemide)
- Effective in patients with sufficient residual renal function and adequate volume status
- Furosemide IV - drives renal K+ excretion
- In CKD patients: large doses required; administer by slow infusion (not bolus) to reduce ototoxicity risk
- Combine with IV saline or isotonic bicarbonate to maintain euvolemia
B. Intestinal Potassium Binders
| Agent | Mechanism | Dose | Onset | Notes |
|---|---|---|---|---|
| Patiromer (preferred) | Polymer binds K+ in exchange for Ca2+ in colon | Powder suspension PO | Hours-days | Side effect: hypomagnesemia; preferred over SPS |
| Sodium zirconium cyclosilicate (SZC) (preferred) | Inorganic crystal - exchanges Na+/H+ for K+ in intestine | Powder suspension PO | Hours | Fewer side effects; also preferred over SPS |
| Sodium polystyrene sulfonate (SPS/Kayexalate) | Exchanges Na+ for K+ in GI tract | 15-30 g PO in sorbitol | Up to 24 hours | Avoid when possible - rare but fatal intestinal necrosis (colon/ileum); risk increased post-op or with opioids |
SPS (Kayexalate) was the mainstay for decades but patiromer and SZC are now preferred due to the risk of intestinal necrosis with SPS. (Harrison's 22e, 2025)
C. Hemodialysis (Definitive, most effective)
- The most reliable and effective method to reduce total body K+
- Indicated for: severe hyperkalemia unresponsive to above measures, anuric/oliguric renal failure, K+ >7.0-8.0 with life-threatening features
- Peritoneal dialysis is considerably less effective than hemodialysis for acute K+ removal
- K+ removed depends on: dialysate K+ gradient, dialyzer type, blood/dialysate flow rates, duration
Quick Reference: Treatment Comparison Table
| Treatment | Onset | Duration | K+ Lowering | Removes K+? |
|---|---|---|---|---|
| Calcium gluconate | 1-3 min | 30-60 min | None (membrane protection only) | No |
| Insulin + glucose | 10-20 min | 4-6 h | ~0.5-1.0 mEq/L | No |
| Albuterol (nebulized) | 30 min | 2-6 h | ~0.5-1.5 mEq/L | No |
| Sodium bicarbonate | 4-6 h | Variable | Modest | No |
| Furosemide | 30-60 min | Hours | Variable | Yes |
| Patiromer / SZC | Hours-days | Ongoing | Variable | Yes |
| Hemodialysis | Minutes once started | Session duration | Large (definitive) | Yes |
Connecting Back to DKA
In DKA, K+ is often paradoxically elevated on presentation due to acidosis shifting K+ extracellularly - but total body K+ is depleted. As you treat DKA with insulin and correct the acidosis, K+ rapidly falls into cells. This is why:
- K+ must be rechecked every 1-2 hours during DKA treatment
- Insulin must be withheld if K+ <3.3 mEq/L
- The initial elevated K+ in DKA is NOT true hyperkalemia - it will correct with treatment
Sources:
- Harrison's Principles of Internal Medicine, 22e (2025) - Ch. on Fluid/Electrolytes
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 9e - Ch. 114
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Ch. 49 (Fig. 49-7)
Incontinence and heavy urine passge
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content on both topics. Let me compile the full, well-structured guide.
Urinary Incontinence and Heavy Urine Passage (Polyuria): Recognition and Management
These are two distinct but sometimes overlapping problems. This guide covers both, with a framework to tell them apart.
PART 1: URINARY INCONTINENCE
Definition: The involuntary leakage of urine sufficient to be a health or social problem.
Epidemiology: Affects 11% of women aged 22-27, rising to 15-30% of older adults at home, one third of acute hospital patients, and over half of nursing home residents. More than twice as common in women as men. Predisposes to pressure ulcers, UTIs, falls, fractures, depression, and social isolation.
Types of Urinary Incontinence
There are four main types - identifying which type a patient has guides all subsequent management.
| Type | Mechanism | Key Symptom Pattern | Common Causes |
|---|---|---|---|
| Urge incontinence | Detrusor overactivity (involuntary bladder contraction) | Sudden, intense urge to void → large volume leakage; frequency >8 voids/day; nocturia | Idiopathic, cerebral disease, UMN lesion, bladder irritation (UTI, stone, tumor) |
| Stress incontinence | Urethral sphincter weakness / poor pelvic support | Leakage coincides exactly with cough, sneeze, laugh, exercise; no leakage at night | Pelvic floor damage post-childbirth, menopause, obesity; post-radical prostatectomy in men |
| Overflow incontinence | Detrusor underactivity OR bladder outlet obstruction → overdistension | Constant dribbling, weak stream, incomplete emptying, large postvoid residual | BPH (men), neurogenic bladder, anticholinergic drugs, fecal impaction |
| Mixed incontinence | Combination (usually urge + stress) | Features of both; determine which is most bothersome to guide therapy | Older women especially |
| Functional incontinence | Cognition/mobility impairment despite relatively normal bladder | Cannot reach toilet in time | Dementia, severe arthritis, deconditioning - but always exclude a treatable LUT cause too |
Transient (Reversible) Causes - Check These FIRST
The mnemonic DIAPPERS covers the most common reversible causes:
| Letter | Cause |
|---|---|
| D | Delirium / confusional state |
| I | Infection (symptomatic UTI) |
| A | Atrophic urethritis / vaginitis |
| P | Pharmaceuticals (see below) |
| P | Psychological (depression, severe) |
| E | Excess urine output (CHF, hyperglycemia, hypercalcemia, diuretics) |
| R | Restricted mobility |
| S | Stool impaction |
Drugs that cause or worsen incontinence:
| Drug | Effect |
|---|---|
| Diuretics | Excess urine volume and urgency |
| Anticholinergics | Urinary retention → overflow |
| Alpha-blockers | Sphincter relaxation → stress leakage |
| Alpha-agonists (e.g., nasal decongestants) | Urethral tone → retention in men |
| Calcium channel blockers | Impair detrusor contraction → retention |
| Sedatives / hypnotics | Impair awareness, mobility |
| ACE inhibitors | Cough → stress incontinence |
| Alcohol | Sedation + diuresis |
Treating the transient cause alone may restore continence completely, even when underlying LUT dysfunction co-exists.
Evaluation
History:
- Type: urge, stress, overflow, or mixed
- Frequency, severity, duration
- Pattern: daytime only? nocturnal? linked to medications?
- Precipitants, associated symptoms (straining, incomplete emptying, dysuria)
- Sexual history, obstetric history (women)
- Medical history: diabetes, neurological disease, prior pelvic surgery, BPH
Physical examination:
- Abdomen: distended bladder (overflow), pelvic mass
- Perineum: atrophic vaginitis, pelvic organ prolapse, cystocele
- Rectal exam: fecal impaction, prostate size
- Neurological: perineal sensation, anal sphincter tone, sacral reflexes
- Stress test: ask patient to cough with a full bladder - observe for immediate leakage
Investigations:
- Urinalysis and urine culture (exclude UTI, hematuria)
- Postvoid residual (PVR) by bladder scan or catheter - >150-200 mL is significant
- Blood glucose, calcium (exclude metabolic causes of polyuria)
- Renal ultrasound if PVR >200 mL in men (check for hydronephrosis)
- Urine cytology if hematuria, pain, or unexplained new/worsening incontinence
- Bladder diary: record time/volume of each void and leak for 3 days
- Urodynamics: reserved for diagnostic uncertainty or before complex surgery
Treatment
Principle: Always treat reversible/transient causes first. A multifactorial approach is needed.
1. Lifestyle Interventions (all types)
- Weight loss (overweight women with stress incontinence - significant benefit)
- Reduce caffeine and alcohol intake
- Optimize fluid intake (avoid both excess and restriction)
- Timed voiding / bladder diary self-monitoring
- Smoking cessation
2. Behavioral Therapy
| Technique | Best For | Details |
|---|---|---|
| Pelvic floor muscle exercises (Kegel) | Stress and urge incontinence | Effective; less effective than surgery for stress incontinence |
| Bladder retraining | Urge incontinence | Progressively increase voiding intervals; resist urgency using distraction/relaxation techniques |
| Prompted/timed voiding | Functional incontinence, frail elderly | Caregiver-assisted scheduled voiding |
For urge incontinence: behavioral therapy is as effective as pharmacotherapy; combining both is better than either alone.
3. Pharmacotherapy
For Urge/Overactive Bladder:
| Drug Class | Examples | Mechanism | Side Effects |
|---|---|---|---|
| Antimuscarinics | Oxybutynin, tolterodine, solifenacin, darifenacin | Block M2/M3 receptors → reduce detrusor contractility | Dry mouth, constipation, blurred vision, cognitive impairment (elderly) |
| Beta-3 agonist | Mirabegron | Relaxes detrusor muscle via β3 receptors | Hypertension, urinary retention; safer cognitively vs. antimuscarinics |
Prefer mirabegron over antimuscarinics in elderly patients due to anticholinergic side effects (cognitive impairment, falls, constipation).
For Stress Incontinence:
- Topical vaginal estrogen (postmenopausal women) - reduces urethral and vaginal atrophy
- Duloxetine (SNRI) - increases sphincter tone via pudendal nerve; limited use due to nausea
For Overflow/Obstruction in Men (BPH):
- Alpha-1 blockers (tamsulosin, alfuzosin) - relax smooth muscle in prostate/bladder neck
- 5-alpha reductase inhibitors (finasteride, dutasteride) - shrink prostate long-term
4. Surgical Options
| Procedure | For |
|---|---|
| Mid-urethral sling (TVT) | Stress incontinence in women |
| Colposuspension (Burch) | Stress incontinence in women |
| Sacral neuromodulation (InterStim) | Refractory urge incontinence; non-obstructive retention |
| TURP / prostatectomy | BPH causing obstruction/overflow |
| Artificial urinary sphincter | Post-prostatectomy incontinence in men |
| Periurethral bulking agents | Stress incontinence, elderly/frail patients |
PART 2: POLYURIA (Heavy Urine Passage)
Definition: Urine output >3 L/day in adults (or >40-50 mL/kg/day).
Normal urine output = 1-2.5 L/day. Polyuria must be distinguished from frequency (voiding often in small amounts) and from incontinence.
Three Major Categories of Polyuria
| Category | Mechanism | Key Feature |
|---|---|---|
| Osmotic polyuria | Excess solutes in urine drag water out | Urine osmolality typically >300 mOsm/kg |
| Hypotonic polyuria (water diuresis) | Insufficient ADH effect → dilute urine | Urine osmolality <300 mOsm/kg |
| Primary polydipsia | Excess water intake suppresses ADH | Urine dilute, serum Na+ low-normal or low |
Differential Diagnosis by Category
Osmotic Polyuria:
- Diabetes mellitus (glucosuria - most common cause overall)
- Post-obstructive diuresis
- Resolving acute tubular necrosis
- Mannitol infusion, high-protein tube feeds
- Salt-wasting nephropathies
Hypotonic Polyuria (Water Diuresis):
| Type | Cause |
|---|---|
| Central (AVP Deficiency / Cranial DI) | Pituitary/hypothalamic damage: head trauma, neurosurgery, tumors (craniopharyngioma), infiltrative disease (sarcoidosis, histiocytosis), post-hypoxic, idiopathic |
| Nephrogenic DI (AVP Resistance) | Kidney does not respond to ADH: chronic renal disease, hypercalcemia, hypokalemia, lithium toxicity, demeclocycline, genetic (X-linked AVPR2 mutation) |
| Primary polydipsia | Excessive water intake: psychiatric illness (schizophrenia, on antipsychotics), hypothalamic lesion affecting thirst center, habit |
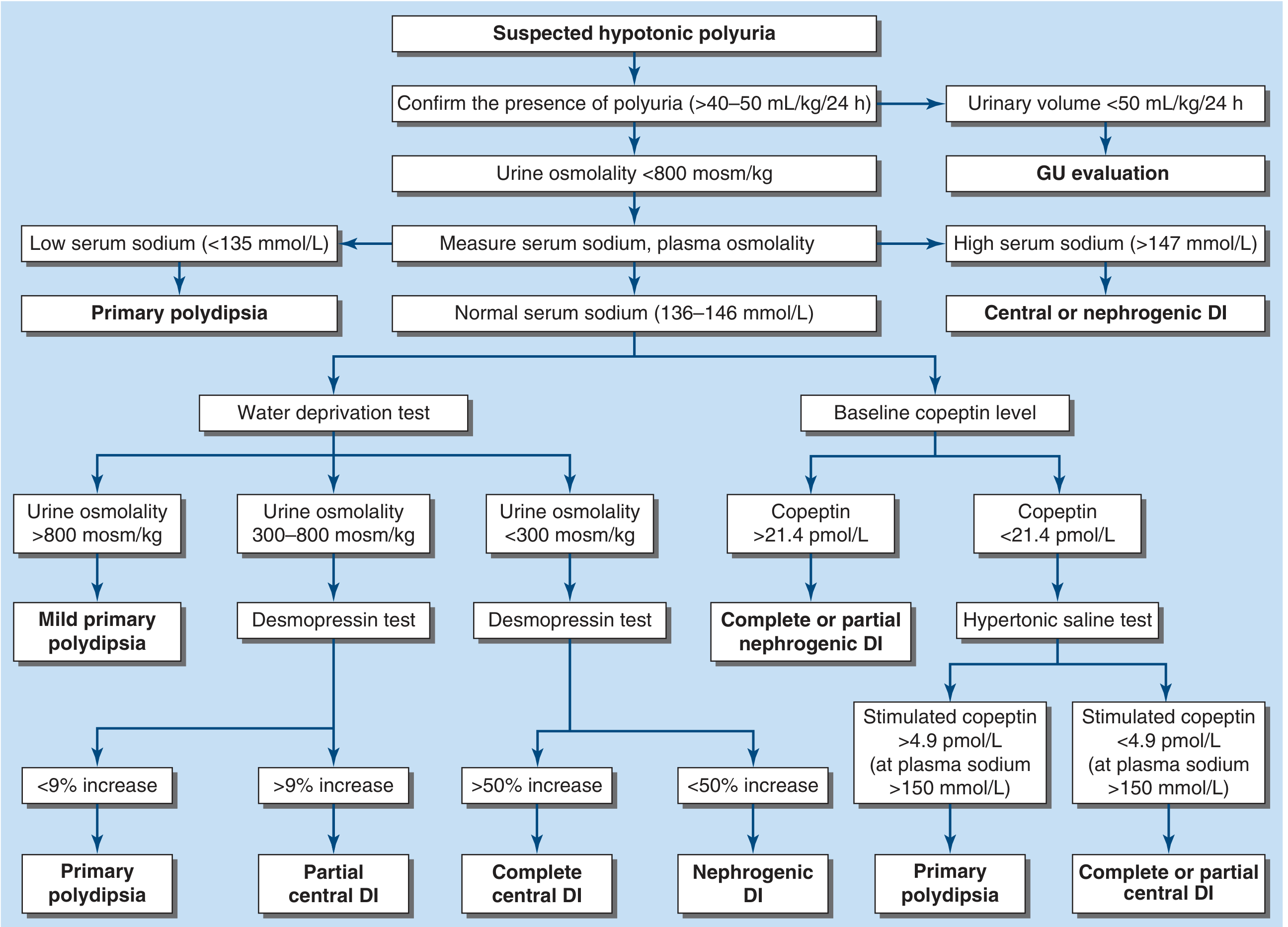
Diagnostic Approach to Polyuria
(Harrison's Principles of Internal Medicine, 22e, 2025)
Step 1: Confirm polyuria - 24-hour urine collection >3 L/day (or >40-50 mL/kg/day)
Step 2: Urine osmolality
- If >300 mOsm/kg → Osmotic polyuria → check urine glucose, BUN, electrolytes
Step 3: If urine dilute (<300 mOsm/kg) → check serum sodium:
The algorithm below guides the differential for hypotonic polyuria:
| Serum Na+ | Diagnosis |
|---|---|
| Low (<135 mmol/L) | Primary polydipsia (patient has drunk themselves into hyponatremia) |
| High (>147 mmol/L) | Central or Nephrogenic DI (ADH deficiency/resistance) |
| Normal (135-146 mmol/L) | Needs further testing (water deprivation test or copeptin) |
Step 4: Water Deprivation Test (indirect) or Copeptin assay (modern preferred method)
Water deprivation test:
- Deprive water under supervision → measure urine osmolality hourly
- Then give desmopressin 2 mcg SC → measure urine osmolality again
| Result | Diagnosis |
|---|---|
| Urine osm >800 mOsm/kg after deprivation | Primary polydipsia (concentrating normally) |
| Urine osm 300-800 → rises >9% after desmopressin | Partial central DI |
| Urine osm <300 → rises >50% after desmopressin | Complete central DI |
| Urine osm <300 → rises <50% after desmopressin | Nephrogenic DI |
Copeptin-based (more accurate, Harrison's 22e):
- Baseline copeptin ≥21.4 pmol/L → Nephrogenic DI
- After hypertonic saline, stimulated copeptin >4.9 pmol/L → Primary polydipsia
- After hypertonic saline, stimulated copeptin <4.9 pmol/L → Central DI
- Diagnostic accuracy ~97% vs. ~70% for water deprivation test
Treatment of Polyuria (by type)
| Type | Treatment |
|---|---|
| Diabetes mellitus | Optimize glycaemic control (insulin, antidiabetic agents) |
| Central DI | Desmopressin (DDAVP) - intranasal, oral, or SC; avoid overtreatment (hyponatremia risk) |
| Nephrogenic DI | Low-sodium diet + thiazide diuretic (paradoxically reduces polyuria by inducing mild volume depletion); indomethacin in some; lithium-induced: stop lithium if possible; amiloride may help |
| Primary polydipsia | Treat underlying psychiatric illness; behavioral restriction of fluid intake |
| Osmotic polyuria (DM) | Control hyperglycaemia; ensure adequate hydration during correction |
Distinguishing Incontinence from Polyuria: Key Clinical Points
| Feature | Incontinence | Polyuria |
|---|---|---|
| Urine volume | Normal total output, leakage is the problem | Genuinely increased 24-h output (>3 L) |
| Control | Cannot control leakage | Can control voiding, but must void frequently due to volume |
| Nocturia | Present (especially urge/overflow type) | Present (often prominent, wakes from sleep) |
| Thirst | Usually not prominent | Prominent in DI and primary polydipsia |
| Key investigation | PVR, urinalysis, urodynamics | 24-h urine, urine osmolality, serum Na |
Both can coexist - a patient with polyuria from DM may also develop urge incontinence because high urine volumes overwhelm bladder capacity, especially at night.
Sources:
- Goldman-Cecil Medicine International Edition - Ch. 115 (Urinary Incontinence)
- Harrison's Principles of Internal Medicine, 22e (2025) - Ch. 393 (AVP Deficiency/DI and Polyuria Algorithm)
- Campbell-Walsh-Wein Urology, 3-Volume Set - Ch. 6
Oxybutanin dose
Finding Sources
Reading File
Reading File
Here is the complete oxybutynin dosing reference:
Oxybutynin Dosing
Oxybutynin is an antimuscarinic (M1/M3 antagonist) with direct smooth muscle relaxant and local anaesthetic properties. It is used for overactive bladder (OAB) / urge incontinence / detrusor overactivity, including neurogenic detrusor overactivity.
Formulations and Doses
1. Immediate-Release (IR) Oral - OXY-IR
| Population | Dose | Frequency | Max Daily Dose |
|---|---|---|---|
| Adults (standard) | 5 mg | 2-3 times daily (up to 4x/day) | 20 mg/day |
| Elderly / frail (start low) | 2.5 mg | Twice daily, then titrate up | 15 mg/day |
| Children (neurogenic bladder) | 2.5-5 mg | 2-3 times daily | Per weight/response |
Start at 2.5 mg twice daily in elderly patients and titrate up as tolerated - the commonly recommended 5 mg TDS is unnecessarily high in many patients and significantly increases side effects. (Campbell-Walsh-Wein Urology)
2. Extended-Release (ER/XL) Oral - OXY-ER
Preferred over IR - same efficacy, fewer side effects (especially less dry mouth) due to reduced first-pass hepatic metabolism.
| Starting Dose | Titration | Usual Effective Dose | Max Dose |
|---|---|---|---|
| 5 mg once daily | Increase by 5 mg weekly if needed | 10 mg once daily | 30 mg once daily |
Take at the same time each day; swallow whole - do NOT crush or chew (osmotic delivery system).
3. Transdermal Patch (OXY-TDS)
| Dose | Application | Frequency |
|---|---|---|
| 3.9 mg/day patch | Apply to abdomen, hip, or buttock | Change twice weekly (every 3-4 days) |
- Bypasses hepatic first-pass metabolism entirely → lowest systemic antimuscarinic side effects
- Main local side effect: skin irritation / pruritus at application site (~17%)
- Rotate application sites
4. Topical Gel (OXY-Gel)
| Dose | Application | Frequency |
|---|---|---|
| 1 g gel (= 100 mg oxybutynin) via metered pump | Apply to abdomen, upper arms/shoulders, or thighs | Once daily |
- Similar side-effect profile to patch - reduced dry mouth vs. oral forms
- Allow to dry before covering with clothing; avoid showering/bathing for 1 hour after
5. Intravesical Instillation (specialist use)
Used in spinal cord injury / neurogenic detrusor overactivity when oral route is not tolerated.
- 5-10 mg in 30 mL of normal saline, instilled into bladder via catheter 2-3 times daily
- Bypasses GI absorption - very low systemic side effects
Side Effects (All Oral Forms)
The antimuscarinic side effects are the main limitation and are dose-dependent:
| Side Effect | Frequency | Notes |
|---|---|---|
| Dry mouth | Up to 70-80% with IR | Most common; improves with ER/patch |
| Constipation | Common | |
| Blurred vision | Common | |
| Drowsiness / sedation | Common | |
| Cognitive impairment | Significant in elderly | Crosses blood-brain barrier; consider mirabegron instead |
| Urinary retention | Risk if outflow obstruction | Check PVR before prescribing |
| Tachycardia | Less common | |
| Heat intolerance | Reduced sweating | Warn patients |
In elderly patients, oxybutynin IR has the worst CNS side-effect profile of all antimuscarinics because it freely crosses the blood-brain barrier. Prefer mirabegron (beta-3 agonist) or a more uroselective antimuscarinic (darifenacin, solifenacin) in older patients. If oxybutynin must be used in elderly, use the patch or gel form to minimize CNS exposure.
Contraindications
- Urinary retention / significant outflow obstruction (PVR >200 mL)
- Gastric retention / severe GI motility disorder
- Uncontrolled narrow-angle glaucoma
- Myasthenia gravis
Quick Dosing Summary
| Formulation | Starting Dose | Usual Dose | Max |
|---|---|---|---|
| IR tablet | 2.5-5 mg BD-TDS | 5 mg TDS | 20 mg/day |
| ER tablet | 5 mg OD | 10 mg OD | 30 mg OD |
| Patch | 3.9 mg/day | 3.9 mg/day | 3.9 mg/day |
| Gel | 1 g OD | 1 g OD | 1 g OD |
Sources: Campbell-Walsh-Wein Urology, 3-Volume Set - Ch. 65; Lippincott Illustrated Reviews: Pharmacology

1000055492.jpg
What drugs to give here
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Excellent - comprehensive evidence from Harrison's 22e and Goldman-Cecil. I have everything needed for a clear, clinically actionable answer.
Report Interpretation
Patient: Ms. Rebata Dule, 56-year-old woman | Apollo Diagnostics, July 2026
| Test | Result | Reference | Interpretation |
|---|---|---|---|
| Albumin - Spot Urine | 658 µg/mL | <20 mg/L | Very elevated |
| Creatinine - Urine | 92.8 mg/dL | 28-217 | Normal |
| uACR (Albumin:Creatinine Ratio) | 709.05 µg/mg | <30 | 🔴 CLINICAL ALBUMINURIA |
709 µg/mg creatinine is far above the clinical albuminuria threshold of >300 µg/mg. This is severely elevated albuminuria (previously called macroalbuminuria/overt proteinuria), consistent with diabetic nephropathy / diabetic kidney disease (DKD).
Drugs to Give
This patient needs a multi-drug, evidence-based renoprotective strategy. The treatment priorities are:
1. ACE Inhibitor OR ARB (First-Line - Mandatory)
The cornerstone of treatment for diabetic albuminuria. Both reduce intraglomerular pressure, albuminuria, and slow GFR decline.
| Drug Class | Examples | Dose |
|---|---|---|
| ACE Inhibitor | Ramipril | 2.5-10 mg OD |
| Enalapril | 5-20 mg OD | |
| Lisinopril | 5-40 mg OD | |
| ARB (if ACE inhibitor not tolerated - e.g., cough) | Losartan | 50-100 mg OD |
| Telmisartan | 40-80 mg OD | |
| Irbesartan | 150-300 mg OD |
Do NOT combine ACE inhibitor + ARB - no additional kidney benefit, and significantly increases risk of hyperkalemia and acute kidney injury.
- Monitor: serum creatinine and K+ at 1-2 weeks after starting, then every 3 months
- Target BP: <130/80 mmHg in diabetics with CKD/albuminuria
2. SGLT2 Inhibitor (Add on top of ACE-I/ARB - now standard of care)
SGLT2 inhibitors independently reduce albuminuria, slow GFR decline, reduce risk of kidney failure, and reduce cardiovascular mortality. Recommended for all type 2 DM patients with albuminuria. (Harrison's 22e, Goldman-Cecil Medicine)
| Drug | Dose | Notes |
|---|---|---|
| Dapagliflozin | 10 mg OD | Approved for DKD (DAPA-CKD trial); can use even if HbA1c at target |
| Canagliflozin | 100 mg OD | CREDENCE trial - significant renal benefit |
| Empagliflozin | 10 mg OD | EMPA-REG outcome trial |
Can continue if eGFR ≥20 mL/min/1.73m². Reduce or stop if eGFR <20. Warn about: euglycaemic DKA (rare but serious), genital mycotic infections, UTI risk.
3. Finerenone (Third Agent - Latest Evidence)
A non-steroidal mineralocorticoid receptor antagonist (MRA) proven to further reduce CKD progression and cardiovascular events in type 2 DM with albuminuria on top of maximum ACE-I/ARB therapy (FIDELIO-DKD and FIGARO-DKD trials). FDA approved in 2021.
| Drug | Dose | Notes |
|---|---|---|
| Finerenone | 10-20 mg OD | Start 10 mg if eGFR 25-60; 20 mg if eGFR ≥60 |
Combining SGLT2 inhibitor with finerenone is now recommended - the SGLT2 inhibitor reduces the risk of hyperkalemia caused by finerenone. Monitor K+ - hold if K+ >5.0 mEq/L before starting.
4. GLP-1 Receptor Agonist (If overweight / HbA1c not at target)
Also reduces albuminuria and slows GFR decline in type 2 DM.
| Drug | Dose | Notes |
|---|---|---|
| Semaglutide | 0.5-1 mg SC weekly | FLOW trial: significant renal benefit |
| Liraglutide | 0.6-1.8 mg SC OD | Cardiovascular + renal benefit |
| Dulaglutide | 0.75-1.5 mg SC weekly |
5. Optimal BP Control - Antihypertensives as Needed
Target BP <130/80 mmHg. If additional agents needed after ACE-I/ARB:
- Amlodipine (calcium channel blocker) - add-on for BP
- Thiazide / thiazide-like diuretic (chlorthalidone/indapamide) - if volume overloaded
- Beta-blocker if heart failure coexists
6. Statin Therapy (Cardiovascular protection)
All patients with DKD + albuminuria are at high cardiovascular risk. Give a high-intensity statin:
| Drug | Dose |
|---|---|
| Atorvastatin | 20-40 mg OD |
| Rosuvastatin | 10-20 mg OD |
7. Glycaemic Control
- Target HbA1c ~7% (6.5-7.5% range depending on comorbidities)
- Continue metformin if eGFR >30 (reduce dose if eGFR 30-45)
- The SGLT2 inhibitor contributes to glycaemic control as well
Summary Prescription Table
| Priority | Drug | Purpose |
|---|---|---|
| 🔴 Mandatory | ACE inhibitor or ARB (e.g., Ramipril 5-10 mg OD) | Renoprotection, BP, albuminuria ↓ |
| 🔴 Mandatory | SGLT2 inhibitor (e.g., Dapagliflozin 10 mg OD) | Renoprotection, CV protection |
| 🟠 Recommended | Finerenone 10-20 mg OD | Further renoprotection + CV |
| 🟠 Recommended | High-intensity statin (Atorvastatin 40 mg OD) | CV protection |
| 🟡 If HbA1c high / obese | GLP-1 agonist (Semaglutide 0.5 mg SC weekly) | Glucose, weight, renal |
| 🟡 If BP not controlled | Add amlodipine 5-10 mg OD | BP target <130/80 |
Before Starting - Check These
- eGFR (creatinine-based) - essential to dose SGLT2 inhibitor and finerenone correctly
- Serum potassium - must be <5.0 before starting finerenone or ACE-I/ARB
- HbA1c - assess overall glycaemic control
- Urine culture - rule out UTI as a cause of transient proteinuria
- Fundus examination - diabetic retinopathy (co-exists in diabetic nephropathy)
- Echo/ECG - baseline cardiac status
Sources: Harrison's Principles of Internal Medicine 22e (2025) - Ch. DM Complications; Goldman-Cecil Medicine - Ch. 64 (SGLT2/Albuminuria treatment)
Urea 157 Creatinine 4 What drugs What dose
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I have the key data. Let me now calculate the eGFR and compile the complete answer.
First: Calculate eGFR
Patient: 56-year-old female, Creatinine = 4 mg/dL
Using the CKD-EPI formula (simplified estimate for female, age 56, Cr 4.0):
eGFR = 141 × min(Cr/κ, 1)^α × max(Cr/κ, 1)^(-1.209) × 0.993^Age × 1.018 (female) For female: κ = 0.7, α = -0.329
With Cr 4.0 mg/dL at age 56 (female):
Estimated eGFR ≈ 11-14 mL/min/1.73 m²
This is CKD Stage 5 (eGFR <15) — approaching or at end-stage renal disease (ESRD).
BUN 157 mg/dL (Urea 157) with Creatinine 4.0 → BUN:Cr ratio = ~39:1 → suggests pre-renal component (dehydration, poor intake) superimposed on CKD, or severe uremia.
⚠️ Critical Alert: Drug Changes Required
At eGFR ~11-14, the drug strategy from the previous visit must be substantially modified. Several drugs are now contraindicated or dangerous.
DRUGS TO STOP / AVOID NOW
| Drug | Why to STOP |
|---|---|
| Metformin | CONTRAINDICATED at eGFR <30 — risk of fatal lactic acidosis |
| SGLT2 inhibitors (dapagliflozin, empagliflozin, canagliflozin) | Not effective at eGFR <20; also risk of euglycaemic DKA in setting of uremia |
| Finerenone | Hold — CONTRAINDICATED if K+ >5.0 or eGFR <25 |
| NSAIDs | Will further destroy residual kidney function |
| Potassium-sparing diuretics (spironolactone, amiloride) | High hyperkalemia risk at this eGFR |
| Sulfonylureas (glibenclamide/glimepiride) | Accumulate → prolonged severe hypoglycemia |
DRUGS TO USE — WITH DOSES ADJUSTED FOR eGFR ~12
1. ACE Inhibitor or ARB — Use with Extreme Caution
Still renoprotective, but at eGFR <15, risk of acute deterioration and hyperkalemia is high. Continue only if K+ <5.0 and creatinine stable (not acutely rising).
| Drug | Dose at eGFR 10-15 | Notes |
|---|---|---|
| Ramipril | 1.25-2.5 mg OD (start very low) | Monitor K+, creatinine weekly |
| Telmisartan (if ACE-I cough) | 20-40 mg OD (half the usual dose) | Same monitoring |
| Losartan | 25-50 mg OD |
Stop immediately if: K+ rises >5.5 mEq/L, creatinine rises >30% from baseline in 2 weeks, or patient develops oliguria.
2. Antihypertensives for BP Control
Target BP: <130/80 mmHg. ACE-I/ARB alone often insufficient at this stage.
| Drug | Dose | Notes |
|---|---|---|
| Amlodipine | 5-10 mg OD | Safe at all eGFR levels; no dose adjustment needed |
| Furosemide (loop diuretic) | 40-80 mg OD or BD | Preferred over thiazide at eGFR <30; also manages fluid overload and hyperkalemia; increase dose as eGFR falls |
| Carvedilol / Atenolol | Carvedilol 3.125-12.5 mg BD | If heart failure or tachycardia present; atenolol accumulates in renal failure — prefer carvedilol |
3. Glycaemic Control — Revised Agents
| Drug | Dose at eGFR ~12 | Status |
|---|---|---|
| Insulin (basal ± bolus) | Start: Glargine 10 units SC at night; titrate | Drug of choice - eGFR does not affect insulin dosing directly, but insulin requirement falls as eGFR worsens (reduced insulin degradation by kidney) → reduce dose by 25-50% to avoid hypoglycemia |
| Gliclazide MR | 30-60 mg OD only (lower risk sulfonylurea) | Use with caution; prefer insulin |
| Repaglinide | 0.5-1 mg with meals | Short-acting; safer in CKD than glibenclamide |
| DPP-4 inhibitors | Sitagliptin 25 mg OD (dose-reduced); Linagliptin 5 mg OD (no renal dose adjustment needed) | Linagliptin is the safest DPP-4 at any eGFR |
Linagliptin 5 mg OD is the preferred oral antidiabetic here - it is excreted via bile (not kidney), so no dose adjustment is needed even at ESRD.
4. Statin (Cardiovascular protection)
| Drug | Dose | Notes |
|---|---|---|
| Atorvastatin | 10-20 mg OD | Hepatically metabolized - safe at all eGFR levels; use lower dose due to increased myopathy risk in severe CKD |
| Rosuvastatin | 5-10 mg OD | Partially renal - use reduced dose at eGFR <30 |
5. Manage Uremia Complications (at eGFR ~12, these are active problems)
| Problem | Drug | Dose |
|---|---|---|
| Metabolic acidosis (very common at eGFR <20) | Sodium bicarbonate | 650 mg BD-TDS, titrate to serum HCO3 22-24 mEq/L |
| Hyperphosphatemia | Calcium carbonate (phosphate binder, with meals) | 500-1000 mg TDS with food |
| Sevelamer (non-calcium binder if Ca high) | 800 mg TDS with meals | |
| Renal anaemia (Hb likely low) | Erythropoietin (EPO/darbepoetin) | After checking iron stores; start if Hb <10 g/dL |
| Iron supplementation (IV iron preferred) | Ferric carboxymaltose or iron sucrose IV if ferritin <200 | |
| Hyperkalemia (K+ likely elevated) | Patiromer or SZC (potassium binders) | Patiromer: 8.4 g OD; SZC: 10 g TDS × 48h then 5 g OD |
| Secondary hyperparathyroidism | Alfacalcidol (activated Vit D) | 0.25-0.5 mcg OD; check Ca, PTH levels |
6. This Patient Likely Needs Nephrology Referral + Dialysis Planning
At eGFR 11-14 with urea 157 and creatinine 4, this patient is at the threshold for renal replacement therapy (RRT). Indications to start dialysis:
- Symptomatic uremia (nausea, vomiting, encephalopathy, pericarditis)
- Refractory fluid overload
- Refractory hyperkalemia (K+ >6.5 despite treatment)
- eGFR <10 with symptoms, or eGFR <6-8 regardless of symptoms
- Severe metabolic acidosis unresponsive to bicarbonate
Plan: Refer urgently to nephrologist for AV fistula creation (takes 6-8 weeks to mature) and haemodialysis planning.
Summary Drug Table
| Drug | Dose | Give / Stop? |
|---|---|---|
| Metformin | — | 🔴 STOP - CONTRAINDICATED |
| SGLT2 inhibitor | — | 🔴 STOP |
| Finerenone | — | 🟡 Hold until K+ and eGFR reassessed |
| Ramipril / Telmisartan | 1.25-2.5 mg OD / 20-40 mg OD | 🟢 Continue cautiously, monitor weekly |
| Furosemide | 40-80 mg OD-BD | 🟢 Start/increase |
| Amlodipine | 5-10 mg OD | 🟢 Safe |
| Linagliptin | 5 mg OD | 🟢 Best oral antidiabetic here |
| Insulin (Glargine) | 10 units nocte, titrate | 🟢 Preferred |
| Atorvastatin | 10-20 mg OD | 🟢 Continue, reduce dose |
| Sodium bicarbonate | 650 mg BD | 🟢 Start |
| Calcium carbonate | 500-1000 mg TDS with meals | 🟢 Start |
| Alfacalcidol | 0.25-0.5 mcg OD | 🟢 Start after checking Ca/PTH |
| Potassium binder | Patiromer 8.4 g OD | 🟢 If K+ >5.0 |
Essential Investigations Now
Before/alongside treatment changes:
- Serum electrolytes (Na, K, HCO3) - K+ is critical
- Full blood count (anaemia of CKD)
- Serum calcium, phosphate, PTH, Vitamin D
- Urine output (oliguria = urgent)
- Renal ultrasound (exclude obstruction - hydronephrosis)
- HbA1c
- Urine culture (exclude acute infection causing deterioration)
Sources: Harrison's Principles of Internal Medicine 22e (2025); Katzung's Basic & Clinical Pharmacology 16e; Goldman-Cecil Medicine; National Kidney Foundation Primer on Kidney Diseases 8e
This is a shared conversation. Sign in to Orris to start your own chat.