I now have comprehensive content from the latest orthopaedic textbooks (Campbell's 15th Ed 2026, Rockwood & Green 10th Ed 2025) and PubMed recent reviews. Let me compile the complete answer.
Recent Advances in Musculoskeletal Infection in Orthopaedics
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, Rockwood & Green's Fractures in Adults 10th Ed 2025, Harrison's 22nd Ed 2025, PubMed 2024-2025 reviews
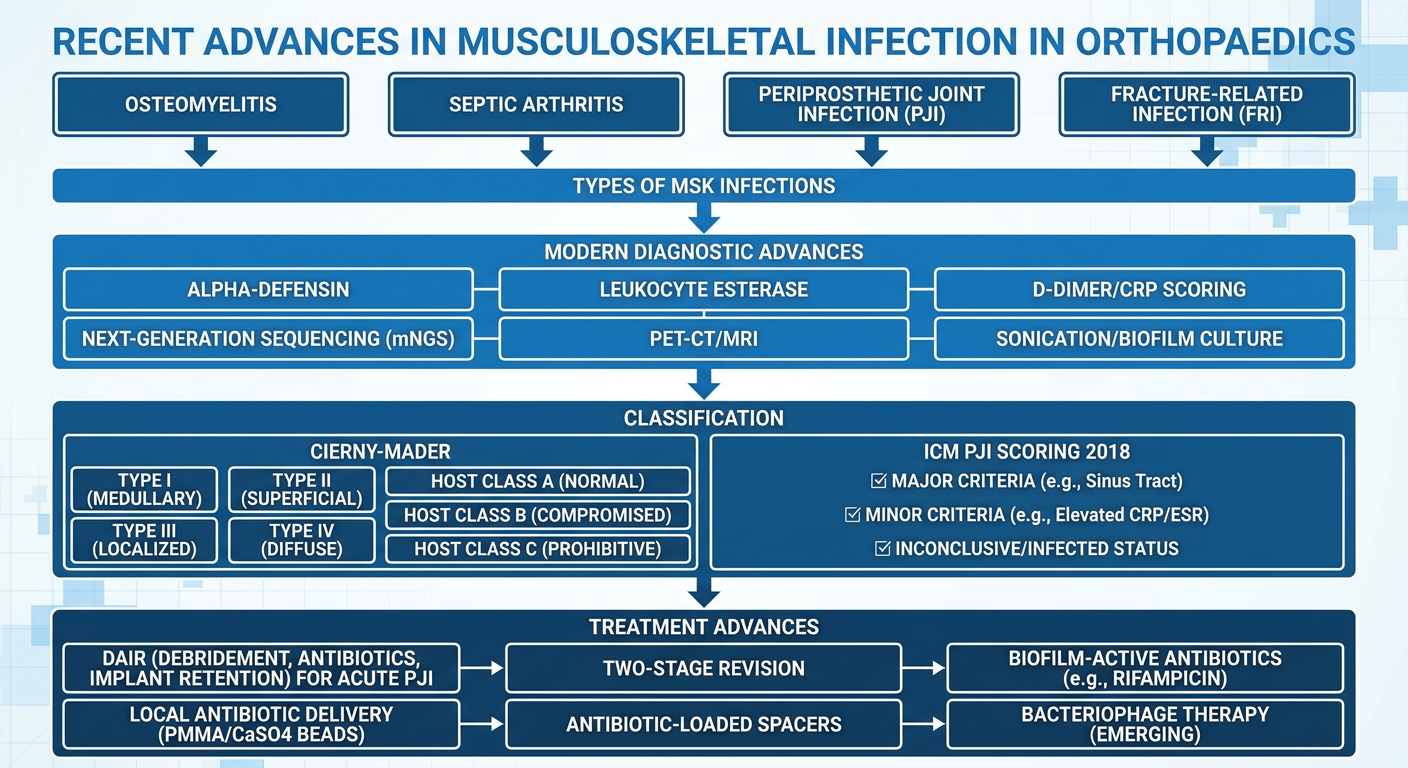
FLOWCHART
TYPES OF MUSCULOSKELETAL INFECTION
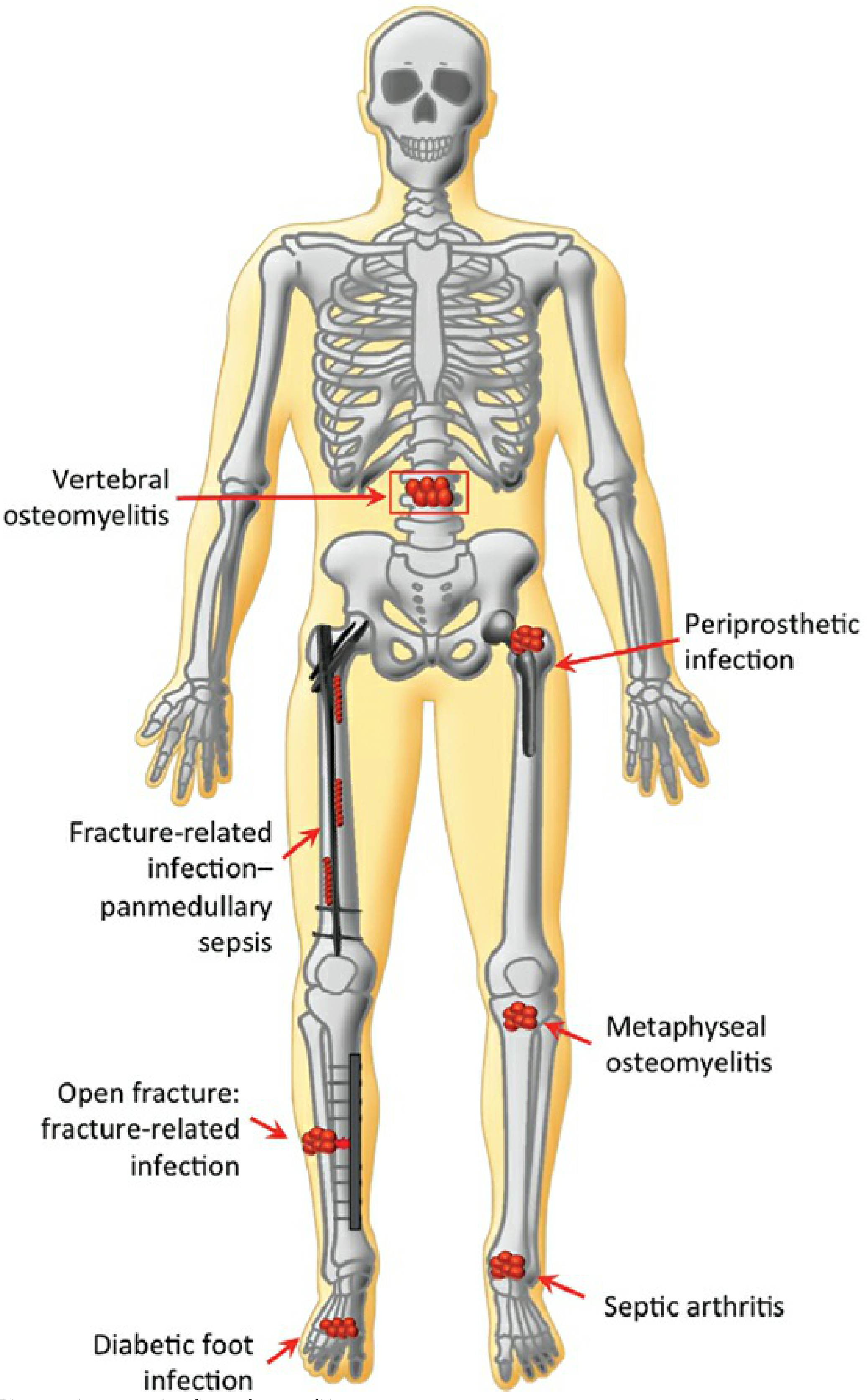
Figure 29-2: Types of Musculoskeletal Infections (Rockwood & Green 10th Ed 2025)
MSK infections are classified into:
- Osteomyelitis (hematogenous, contiguous-focus, post-traumatic)
- Septic Arthritis
- Periprosthetic Joint Infection (PJI)
- Fracture-Related Infection (FRI)
1. OSTEOMYELITIS - CLASSIFICATION
Cierny-Mader Classification System (Most Widely Used)
| Anatomic Type | Description |
|---|
| Type I | Medullary - endosteal disease |
| Type II | Superficial - cortical surface infected due to coverage defect |
| Type III | Localized - cortical sequestrum excisable without instability |
| Type IV | Diffuse - features of I+II+III plus mechanical instability |
| Physiologic Host Class | Characteristics |
|---|
| A | Normal immune system, good local vascularity |
| B-local (BL) | Compromised locally (poor vascularity, scarring) |
| B-systemic (BS) | Compromised systemically (DM, renal failure, malnutrition) |
| C | Treatment worse than disease; suppressive/no treatment |
This gives 12 distinct clinical stages. A type II lesion in a class A host = Stage IIA chronic osteomyelitis. - Campbell's Operative Orthopaedics 15th Ed 2026
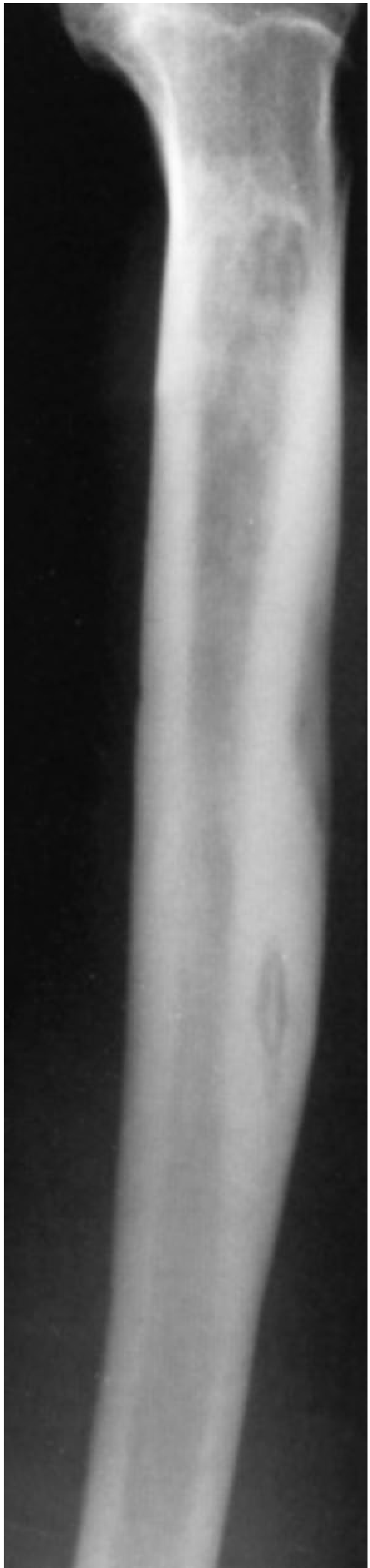
Figure 23.6: Sequestrum of chronic osteomyelitis in tibia
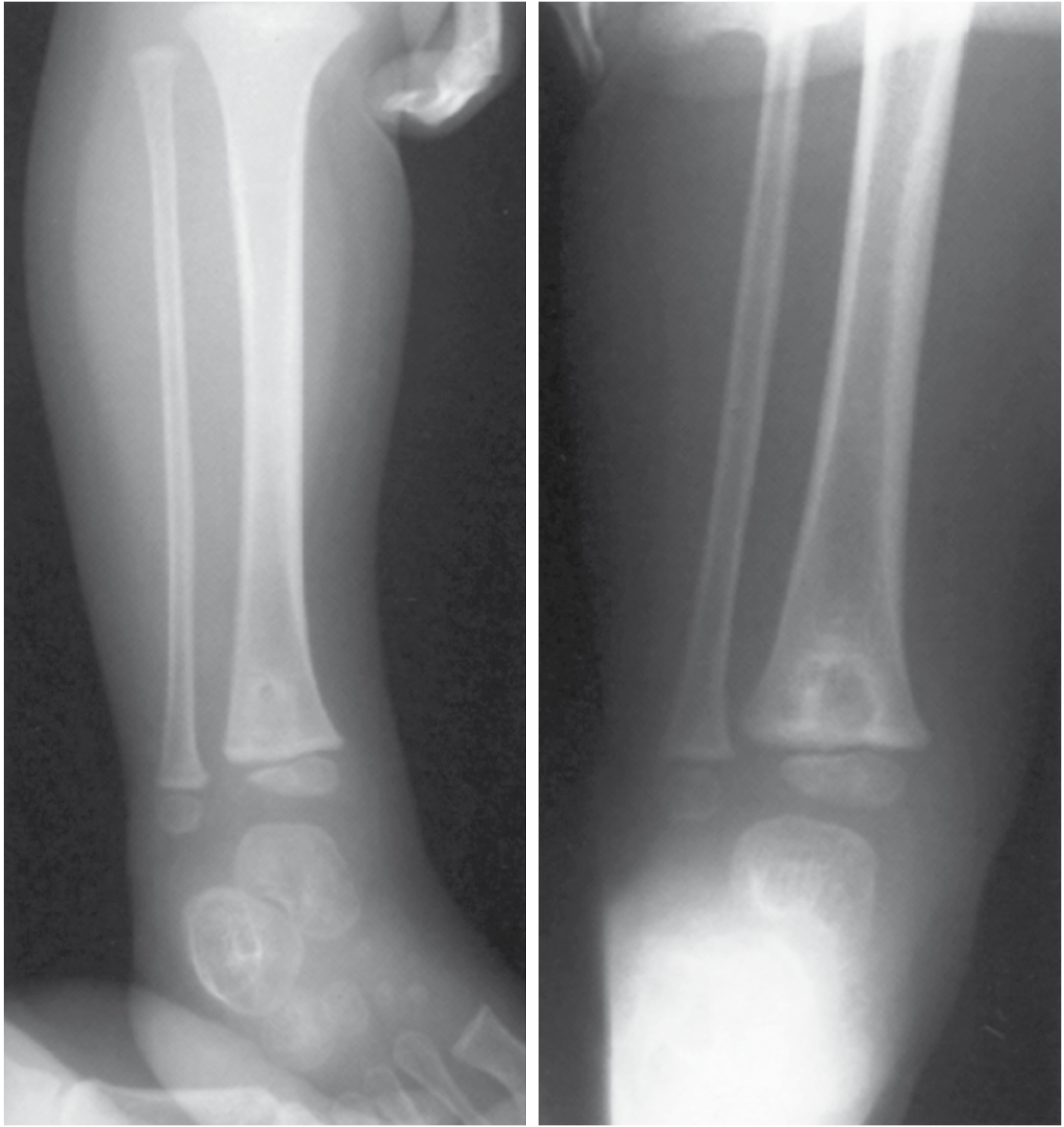
Figure 23.5: Brodie abscess in right distal tibial epiphysis (subacute osteomyelitis)
2. RECENT ADVANCES IN DIAGNOSIS
A. Biomarkers - Novel Synovial Fluid Markers
The ICM (International Consensus Meeting) 2018 scoring-based criteria for PJI use a tiered approach:
Major Criteria (either = Infected):
- Two positive cultures of the same organism
- Sinus tract communicating with joint/prosthesis visible
Minor Criteria (Score-based):
| Marker | Score |
|---|
| Elevated CRP or D-Dimer (serum) | 2 |
| Elevated ESR (serum) | 1 |
| Elevated synovial WBC or Leukocyte Esterase (LE) | 3 |
| Positive alpha-defensin (synovial) | 3 |
| Elevated synovial PMN% or dry tap | 2 |
| Elevated synovial CRP | 1 |
Score: ≥6 = Infected; 2-5 = Possibly Infected; 0-1 = Not Infected - Rockwood & Green 10th Ed 2025
Alpha-defensin is an antimicrobial peptide produced by neutrophils in response to infection - it is now a key novel synovial fluid biomarker for PJI. D-Dimer has been added to the ICM criteria (2018 update) as it outperforms fibrinogen in sensitivity.
B. Advanced Imaging
| Modality | Role |
|---|
| MRI | Gold standard for early osteomyelitis, vertebral infections, soft tissue involvement (sensitivity ~90%) |
| 18F-FDG PET-CT | Detects metabolically active infection; superior for chronic/implant-related infection where MRI artifact limits view |
| SPECT/CT | Improved specificity for osteomyelitis vs. stress reaction |
| Ultrasound | Guides joint aspiration, detects periosteal elevation in early acute osteomyelitis |
C. Molecular Diagnostics - Next-Generation Sequencing (NGS)
Culture-negative infections occur in up to 32% of post-traumatic osteomyelitis and 41% of vertebral osteomyelitis cases. - Rockwood & Green 2025
Recent advances address this:
- Metagenomic NGS (mNGS): Broad-range pathogen detection from sonicate fluid or tissue without prior culture; identifies rare/fastidious organisms
- Targeted NGS/Broad-range PCR: 16S rRNA PCR identifies organisms by partial gene sequencing even in culture-negative cases
- A 2023 systematic review confirmed NGS supports targeted antibiotic therapy in PJI
D. Sonication of Implants
Implant sonication dislodges biofilm organisms into fluid for enhanced culture - sensitivity increases from 60.8% (periprosthetic tissue culture) to 78.5%. This is now a standard technique at major centers for explanted implants.
3. RECENT ADVANCES IN UNDERSTANDING - BIOFILM
The central challenge in MSK infection is biofilm - a structured community of microorganisms enclosed in a self-produced matrix adhering to surfaces.
Key biofilm facts:
- Biofilm organisms are up to 800-fold less susceptible to antibiotics than planktonic organisms - Rockwood & Green 2025
- Pathogens communicate via quorum sensing (autoinducer signal molecules), coordinating biofilm maturation
- Polymicrobial biofilms are more antibiotic-resistant than monospecies biofilms
- Small-colony variants (SCVs) survive in metabolically inactive states, resisting cell wall-active antibiotics and aminoglycosides
4. PERIPROSTHETIC JOINT INFECTION (PJI) - ADVANCES
PJI affects 0.3-2.4% of primary THAs and 1.0-3.0% of primary TKAs; it is the leading cause of TKA revision (15.4-25.0%). Hospitalization cost: $25,692 (TKA revision) to $31,753 (THA revision). - Rockwood & Green 2025
Treatment Algorithm
PJI Confirmed
|
+-- Acute (<4-6 weeks from onset or <30 days from surgery)
| |
| --> DAIR (Debridement, Antibiotics, Implant Retention)
| + biofilm-active antibiotic (Rifampicin for staph)
|
+-- Chronic (>4-6 weeks)
|
--> Two-Stage Revision (GOLD STANDARD)
Stage 1: Explant + antibiotic-loaded cement spacer
Stage 2: (6-12 weeks later) Re-implantation
OR
--> One-Stage Revision (selected patients, known organism)
DAIR (Debridement, Antibiotics, and Implant Retention):
- For early PJI with stable, well-fixed implant
- Success ~50-70% for acute infections
- Exchange of modular components (polyethylene liner) is essential
- Biofilm-active antibiotics: Rifampicin (staphylococci), Ciprofloxacin (Gram-negative)
Antibiotic-Loaded Cement Spacers:
- Gentamicin + Vancomycin combination most common
- Deliver high local concentrations exceeding systemic biofilm MIC
Recent PJI Publications (2024-2025)
5. FRACTURE-RELATED INFECTION (FRI)
FRI is a relatively newly defined entity. The
FRI consensus definition (Metsemakers et al.) distinguishes:
Confirmatory Criteria (definite infection):
- Fistula, sinus, wound breakdown communicating with fracture
- Purulent drainage
- Organism on culture from two independent deep specimens
- Positive histopathology
Suggestive Criteria (further investigation needed):
- Pain at fracture site
- Radiologic signs (periosteal reaction, implant loosening)
- Elevated CRP/ESR/PCT
Management:
- Stable implant with good bone healing potential: DAIR + targeted antibiotics
- Stable implant, bone NOT healed: retain implant + local/systemic antibiotics until union, then address infection
- Failed/loose implant: Implant exchange or removal + stabilization + debridement
6. ADVANCES IN ANTIBIOTIC DELIVERY
Local Antibiotic Delivery Systems (LADS)
| System | Antibiotic | Feature |
|---|
| PMMA beads (non-resorbable) | Tobramycin/Gentamicin | Requires second surgery for removal |
| Calcium sulphate (CaSO4) beads | Vancomycin/Tobramycin | Resorbable; no second surgery; fills dead space |
| Calcium phosphate | Broad-spectrum | Osteoconductive scaffold |
| Antibiotic-coated nails | Gentamicin/Vancomycin | For infected tibial nailing |
High local antibiotic concentrations overcome biofilm MIC without systemic toxicity. Dead-space management is a cornerstone principle.
7. EMERGING THERAPIES
| Advance | Status |
|---|
| Bacteriophage therapy | Case reports/early trials for multi-drug resistant biofilm infections |
| Biofilm-disrupting enzymes (e.g., dispersin B) | Preclinical/early clinical |
| Quorum sensing inhibitors | Experimental |
| Silver/zinc nanocoatings on implants | Clinical trials ongoing |
| DAIR + phage cocktail for MRSA PJI | Case series (2024) |
8. SEPTIC ARTHRITIS - DIAGNOSTIC ADVANCES
| Investigation | Finding |
|---|
| Synovial WBC | >25,000/µL with >90% neutrophils |
| Gram stain positivity | ~50% |
| Culture positivity | ~90% of synovial fluid |
| Blood cultures | Positive in 30-50% |
| MRI | Preferred for vertebral/deep joint infections |
The addition of synovial alpha-defensin and leukocyte esterase dipstick test has improved point-of-care diagnosis. - Harrison's 22nd Ed 2025
SUMMARY TABLE - RECENT ADVANCES AT A GLANCE
| Domain | Recent Advance |
|---|
| Diagnosis | ICM 2018 scoring system for PJI (alpha-defensin, D-Dimer, LE) |
| Microbiology | mNGS for culture-negative infections |
| Imaging | PET-CT, SPECT/CT for chronic/implant infections |
| Biofilm | Understanding quorum sensing; 800-fold antibiotic resistance |
| Classification | FRI consensus definition (2018); Cierny-Mader staging |
| Surgery | DAIR concept; one-stage revision for PJI |
| Local delivery | Resorbable CaSO4 beads; antibiotic-coated implants |
| Emerging | Bacteriophage therapy; quorum sensing inhibitors |
Key Teaching Points (for 10-mark answer):
- Biofilm is the central mechanism explaining treatment failure in MSK infection
- The ICM 2018 scoring for PJI is the current gold standard diagnostic criteria
- Culture-negative infections require molecular methods (NGS/PCR)
- DAIR is reserved for acute PJI with stable well-fixed implants
- Two-stage revision remains the gold standard for chronic PJI
- Resorbable local antibiotic delivery (CaSO4 beads) avoids second surgery
- FRI is a distinct entity from osteomyelitis with its own consensus definition (2018)
- PET-CT outperforms bone scan for diagnosing chronic/implant-associated infection