Abnormal uterine bleeding
Reading File
Finding Sources
Finding Sources
Searching PubMed
"abnormal uterine bleeding"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from multiple textbooks. Let me compose the full answer.
Abnormal Uterine Bleeding (AUB)
Definition
Abnormal uterine bleeding is any bleeding that falls outside the parameters of a normal menstrual cycle. A normal cycle occurs every 24-38 days, with flow lasting 4-8 days. The outdated terms "menorrhagia," "metrorrhagia," and "dysfunctional uterine bleeding" have been replaced by a unified classification system. AUB affects 10-30% of women of reproductive age and is one of the most common gynecologic complaints.
- Sabiston Textbook of Surgery, p. 2937
- Goldman-Cecil Medicine, p. 2555
PALM-COEIN Classification (FIGO, 2011)
The International Federation of Gynecology and Obstetrics (FIGO) established this system to standardize the language around AUB causes:
PALM - Structural Causes (diagnosed by imaging or histology)
| Acronym | Condition |
|---|---|
| P | Polyp (AUB-P) |
| A | Adenomyosis (AUB-A) |
| L | Leiomyoma (AUB-L) - submucosal (LSM) or other (LO) |
| M | Malignancy and Hyperplasia (AUB-M) |
COEIN - Nonstructural Causes (medical/functional)
| Acronym | Condition |
|---|---|
| C | Coagulopathy (AUB-C) |
| O | Ovulatory Dysfunction (AUB-O) |
| E | Endometrial (AUB-E) |
| I | Iatrogenic (AUB-I) |
| N | Not otherwise classified (AUB-N) |
- Rosen's Emergency Medicine, p. 1419
- Sabiston Textbook of Surgery, p. 2937
Causes by Age Group
The causes of AUB vary significantly by the patient's life stage (from Robbins & Kumar Basic Pathology):
| Age Group | Common Causes |
|---|---|
| Prepuberty | Precocious puberty (hypothalamic, pituitary, or ovarian origin) |
| Adolescence | Anovulatory cycles (HPO axis immaturity), coagulation disorders |
| Reproductive age | Pregnancy complications, PCOS, polyps, leiomyomas, endometrial hyperplasia, coagulopathy |
| Perimenopausal | Anovulatory bleeding from incipient ovarian failure, hyperplasia, carcinoma |
| Postmenopausal | Endometrial atrophy (most common), endometrial carcinoma, polyps |
Key facts:
- ~20% of AUB is postmenarchal in adolescents (immature HPO axis)
- ~50% is perimenopausal
- ~75% of cases have no demonstrable organic cause (anovulatory/dysfunctional)
- Up to 20% of women with heavy menstrual bleeding have an underlying coagulopathy; von Willebrand disease is the most common (up to 13% of AUB cases)
Pathophysiology
Anovulatory bleeding is the most common mechanism. Without ovulation, there is no corpus luteum, so progesterone is absent. Estrogen acts on the endometrium unopposed, causing irregular, thickened endometrium that sheds unpredictably. This may result from:
- Hypothalamic/pituitary dysfunction (e.g., prolactinoma reducing GnRH)
- Polycystic ovarian syndrome (PCOS)
- Functioning ovarian tumors (granulosa cell tumors)
- Obesity, malnutrition, or chronic systemic illness
- An inadequate luteal phase (luteal phase defect)
Other structural causes - polyps, fibroids, adenomyosis - cause bleeding through direct endometrial distortion and increased surface area.
- Robbins & Kumar Basic Pathology, p. 609
- Goldman-Cecil Medicine, p. 2555
Normal Menstrual Cycle Diagram
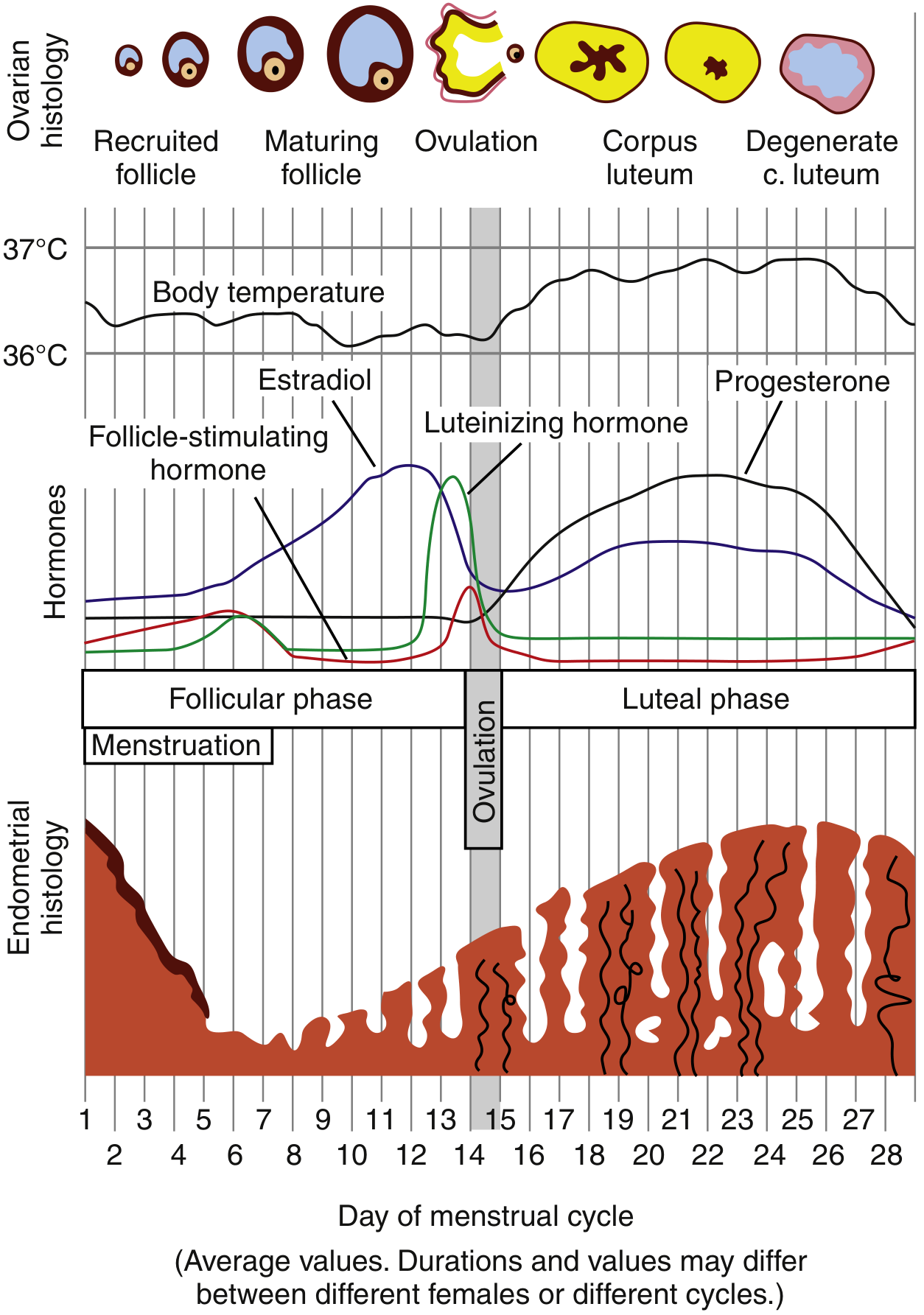
Normal menstrual cycle showing hormonal fluctuations and endometrial changes throughout the cycle. (Rosen's Emergency Medicine)
Clinical Evaluation
History
- Volume, duration, frequency, and pattern of bleeding
- Prospective charting of bleeding days (if pattern is unclear)
- Must exclude: pregnancy complications, bleeding diathesis
- Ask about excessive bruising, family history of bleeding disorders
- Signs/symptoms of thyroid disease, PCOS, or systemic illness
Physical Examination
- Hemodynamic status (signs of hypovolemia/anemia in acute presentation)
- Signs of PCOS: obesity, acne, hirsutism, acanthosis nigricans
- Thyroid palpation
- Skin: petechiae, ecchymosis (coagulopathy)
- Speculum exam: vaginal/cervical lesions
- Bimanual exam: uterine enlargement or fibroid mass
Laboratory Tests
- Urine/serum β-hCG - always first in reproductive-age women
- CBC + platelet count - assess anemia and thrombocytopenia
- Coagulation studies (PT, PTT) - if coagulopathy suspected
- Von Willebrand disease screen - in heavy bleeding since menarche or family history
- TSH - thyroid dysfunction is associated with AUB
- Prolactin, FSH - if anovulation suspected
- Fasting glucose - metabolic workup
- STI testing (Chlamydia) - if risk factors or signs of PID
Imaging
- Transvaginal ultrasound (TVUS): first-line imaging; detects fibroids, polyps, endometrial thickening
- In postmenopausal women: endometrial thickness < 4-5 mm on TVUS reliably excludes endometrial cancer
- A thickened endometrium warrants biopsy
- Sonohysterography (saline infusion): improves detection of intrauterine lesions
- Hysteroscopy + biopsy: gold standard; highest sensitivity and specificity for intracavitary pathology
Endometrial Biopsy Indications
-
All women ≥ 45 years with AUB
-
Women < 45 years with: unopposed estrogen exposure (obesity, PCOS), persistent or treatment-refractory AUB, elevated familial cancer risk (e.g., Lynch syndrome)
-
Any postmenopausal bleeding
-
Sabiston Textbook of Surgery, p. 2941
-
Bailey and Love's Surgery, p. 2753
Management
Acute Heavy Bleeding / Hemodynamic Instability
- Resuscitation: IV fluids, blood products as needed
- IV conjugated estrogens: 25 mg IV every 4-6 hours for up to 3 doses (or 24 hours) until bleeding stops
- Concurrent progestin: medroxyprogesterone acetate 5-10 mg orally to stabilize the endometrium
- Intrauterine tamponade: 26 Fr Foley catheter inflated with 30 mL saline (temporizing measure)
- Surgical options: urgent D&C, uterine artery embolization, endometrial ablation, or hysterectomy
Medical Management (Non-Emergent)
| Option | Details |
|---|---|
| Combined OCP | 35 μg ethinyl estradiol pill every 6 hours x 5-7 days (acute), then cyclic OCPs for maintenance; bleeding stops within 24 hours |
| Progestin-only | Norethindrone 5 mg orally TID x 1 week, or medroxyprogesterone acetate 5-10 mg x 10 days; for patients with estrogen contraindications |
| Tranexamic acid | Antifibrinolytic; 1.3 g orally every 8 hours x 5 days OR 10 mg/kg IV (max 600 mg) for acute bleeding; more effective than NSAIDs |
| NSAIDs | Reduce heavy menstrual flow and dysmenorrhea; less effective than tranexamic acid or hormonal IUD |
| Levonorgestrel IUD | Excellent long-term option; reduces bleeding significantly; suitable for those wanting contraception |
| GnRH agonists | Elagolix 300 mg BID or relugolix 40 mg daily; for fibroids or endometriosis-related AUB |
Surgical Management
| Procedure | Indication |
|---|---|
| Endometrial ablation | Persistent AUB refractory to medical therapy; not 100% effective |
| Hysteroscopic polypectomy | AUB due to polyps |
| Myomectomy | Symptomatic fibroids (fertility desired) |
| Uterine artery embolization | Fibroids; less invasive alternative to surgery |
| Hysterectomy | Definitive; refractory symptoms, malignancy, or adenomyosis |
- Goldman-Cecil Medicine, p. 2556-2557
- Rosen's Emergency Medicine, p. 1421
- Sabiston Textbook of Surgery, p. 2935
Postmenopausal Bleeding - Special Consideration
Any bleeding in a postmenopausal woman (defined as 12 months without menses) is abnormal and requires thorough evaluation. Common causes:
- Endometrial atrophy (most common) - thinning of the endometrium/vaginal tissue from estrogen deficiency
- Endometrial carcinoma - major concern; must be excluded
- Endometrial polyps
- Vaginal atrophy
Tamoxifen use (in breast cancer treatment) induces uterine abnormalities in 10-40% of women (polyps, hyperplasia, rarely sarcoma) and represents a high-risk group requiring vigilant surveillance.
- Bailey and Love's Surgery, p. 2777
- Sabiston Textbook of Surgery, p. 2943
Key Points Summary
- AUB in reproductive-age women: always exclude pregnancy first
- The PALM-COEIN system is the current standard classification (FIGO 2011)
- Anovulation is the most common underlying mechanism
- Von Willebrand disease is the most common coagulopathy causing AUB
- TVUS is the first-line imaging; endometrial biopsy is indicated at age ≥ 45 or with risk factors
- Acute hemodynamically unstable AUB: resuscitate + IV estrogens + consider surgical options
- Stable AUB: treat with OCPs, progestins, tranexamic acid, or LNG-IUD based on cause and patient preference
- Postmenopausal bleeding: always investigate to exclude endometrial carcinoma
This is a shared conversation. Sign in to Orris to start your own chat.