Megaloblastic anemia long answers medicine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive long-answer response. Let me compose it.
Megaloblastic Anemia - Comprehensive Long Answer
Definition
Megaloblastic anemia is defined as an anemia or pancytopenia resulting from failure of DNA synthesis, creating an imbalance between nuclear and cytoplasmic maturation. This results in large cells subject to maturation arrest and early destruction. The unifying feature across all its causes is impaired production of thymidine (and purines) for DNA, causing nuclear maturation to lag behind cytoplasmic development - a phenomenon called nuclear-cytoplasmic asynchrony (dyssynchrony).
The most frequent causes of severe megaloblastic anemia are deficiencies of cobalamin (vitamin B12) and folate.
(Goldman-Cecil Medicine, Ch. 150)
Etiology and Classification
A. Vitamin B12 (Cobalamin) Deficiency
| Category | Examples |
|---|---|
| Lack of intrinsic factor | Pernicious anemia (Type A gastritis), gastrectomy, gastric bypass, congenital IF defect |
| Food cobalamin malabsorption | Atrophic gastritis (Type B), gastric achlorhydria, exocrine pancreatic dysfunction |
| Ileal disease | Ileal resection, Crohn disease, ileal conduit; Imerslund-Gräsbeck syndrome (cubam receptor defect) |
| Competitive/parasitic uptake | Tropical sprue, bacterial overgrowth, blind loops, Diphyllobothrium latum, Giardia lamblia |
| Nutritional deficiency | Strict vegans, lacto-ovo vegetarians, breast-fed infants of deficient mothers |
| Drug-induced | Nitrous oxide abuse, metformin, PPIs/H2-blockers |
| Inborn errors | Transcobalamin deficiency; methylmalonic acidemia + homocystinuria (CblC-J) |
B. Folate Deficiency
| Category | Examples |
|---|---|
| Decreased intake | Inadequate diet, alcoholism, infancy, anorexia nervosa |
| Impaired absorption | Celiac disease, tropical sprue, Crohn disease; drugs (anticonvulsants, oral contraceptives) |
| Increased demand/loss | Pregnancy, hemolytic anemias, psoriasis, leukemias, hemodialysis |
| Impaired utilization | Methotrexate, pemetrexed, trimethoprim, pyrimethamine, sulfasalazine |
C. Other Causes (B12/Folate Independent)
- Metabolic inhibitors of DNA synthesis (cytarabine, hydroxyurea, azathioprine)
- Orotic aciduria (inborn error of pyrimidine synthesis)
- Copper deficiency (excess penicillamine or zinc intake)
- Nitrous oxide inhalation (inactivates methionine synthase)
(Robbins & Cotran Pathologic Basis of Disease, Table 14.5; Goldman-Cecil, Table 150-2)
Pathophysiology
Cobalamin (B12)
Vitamin B12 is required for two key enzymatic reactions in humans:
-
Methionine synthase reaction: Methylcobalamin converts homocysteine → methionine, while simultaneously releasing tetrahydrofolate (FH4) from its "trapped" form N5-methyl-FH4. Without B12, FH4 is unavailable for dUMP → dTMP conversion (DNA synthesis). This is the "folate trap" hypothesis - explains why B12 deficiency mimics folate deficiency hematologically.
-
Methylmalonyl-CoA mutase reaction: Adenosylcobalamin converts methylmalonyl-CoA → succinyl-CoA. B12 deficiency leads to accumulation of methylmalonyl-CoA and methylmalonic acid (MMA) - this is the basis of the neurological damage and the most specific biochemical marker.
The neurological complications of B12 deficiency are NOT improved by folate (and may be worsened) because they depend on the methylmalonyl-CoA pathway, not the folate-dependent pathway.
Folate
Folate (as FH4) is required for:
- Transfer of one-carbon fragments in purine and thymidine synthesis
- The reaction: dUMP → dTMP (via N5,10-methylene FH4 + thymidylate synthase)
Folate deficiency impairs DNA synthesis identically to B12 deficiency hematologically, but does NOT cause neurological disease.
Common Final Pathway
In both deficiencies: impaired DNA synthesis → all proliferating cells affected → ineffective hematopoiesis with intramedullary destruction of abnormal precursors → pancytopenia. Elevated LDH and indirect bilirubin result from this intramedullary hemolysis.
(Robbins & Cotran, p. 608-609)
Morphology and Pathology
Peripheral Blood Smear
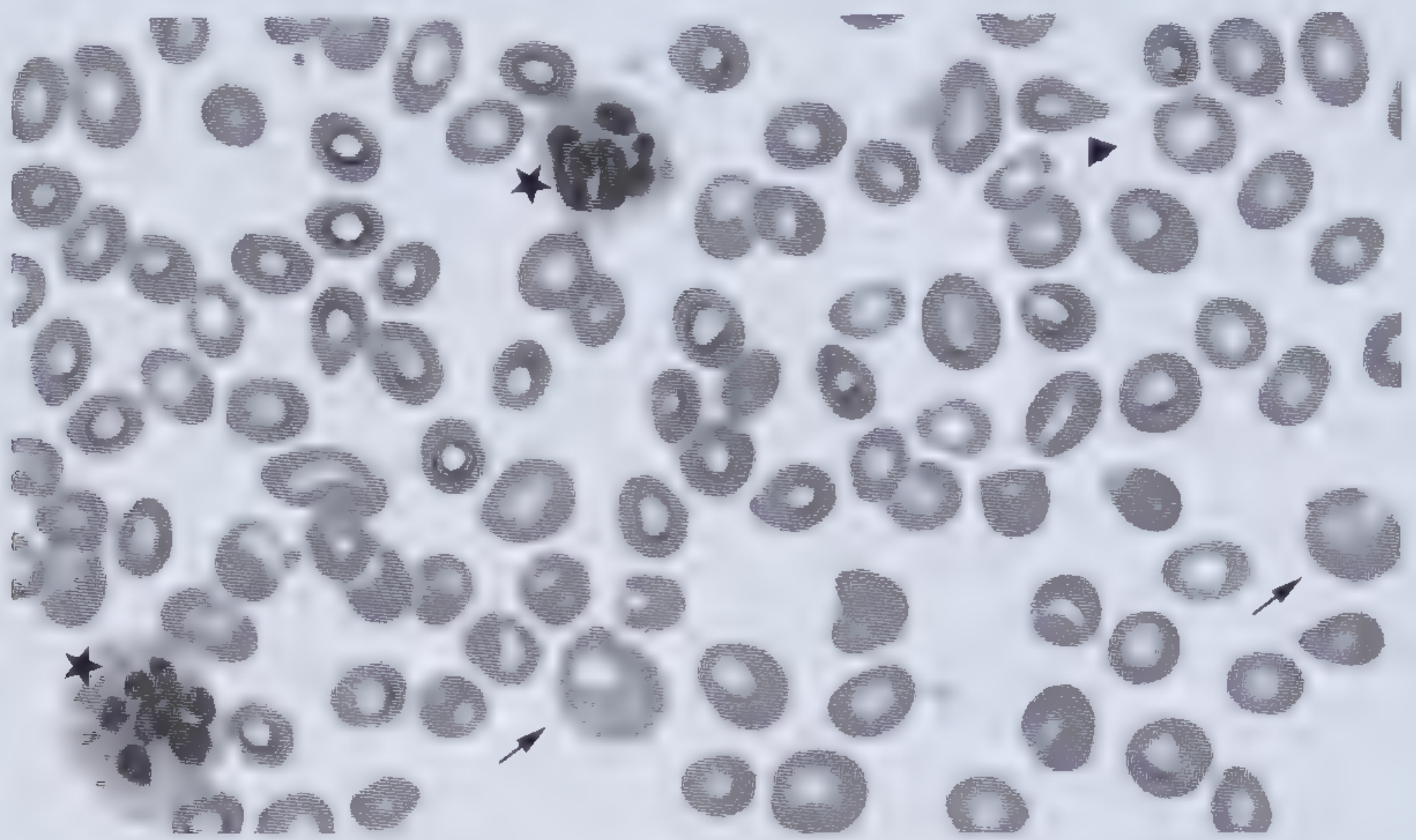
Peripheral blood smear: macro-ovalocytes (arrows), hypersegmented neutrophil (star), teardrop RBCs (arrowhead) - from Wintrobe's Atlas
Key findings:
- Macro-ovalocytes (MCV often >115 fL) - large, oval RBCs without central pallor
- Hypersegmented neutrophils - >5% with ≥5 lobes, or any cell with ≥6 lobes (most specific)
- Anisocytosis and poikilocytosis (teardrop cells)
- Low reticulocyte count (ineffective erythropoiesis)
- Occasional nucleated RBC precursors in severe anemia
- Thrombocytopenia (large, bizarre platelets)
Peripheral Blood Smear - Hypersegmented Neutrophil
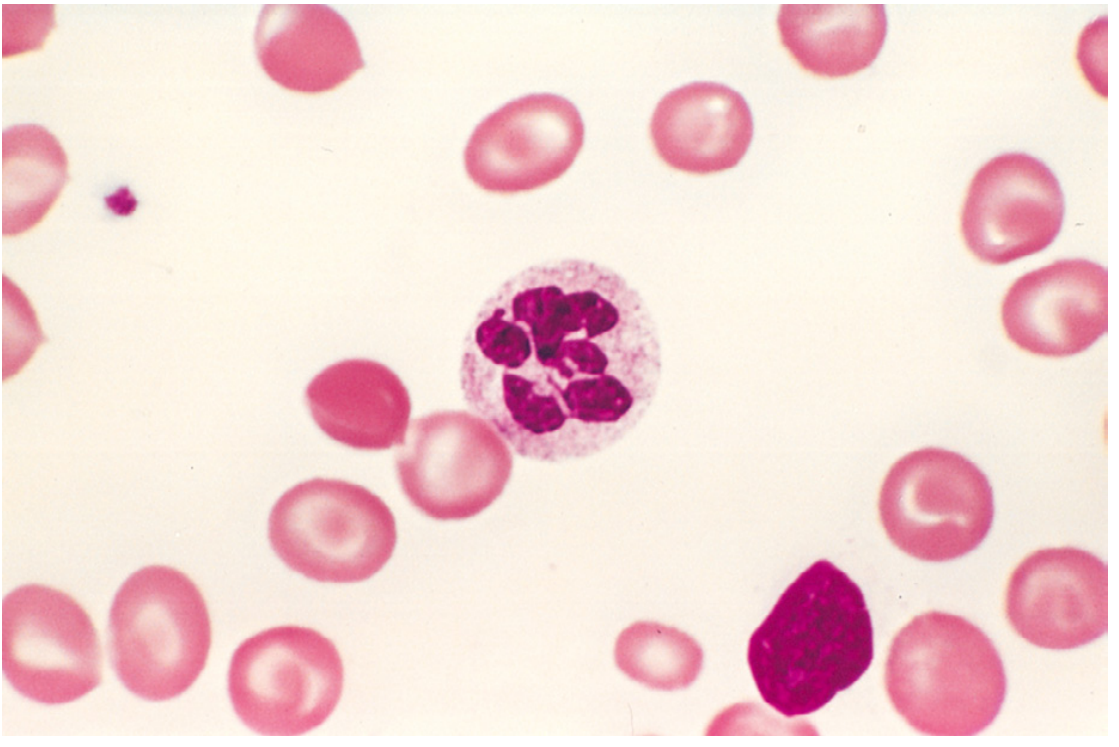
Megaloblastic anemia - hypersegmented neutrophil with six-lobed nucleus (Robbins & Cotran, Fig. 14.15)
Bone Marrow
- Markedly hypercellular (increased erythroid, granulocytic, and megakaryocytic precursors)
- Megaloblasts at all stages of erythroid development:
- Promegaloblasts: large, deeply basophilic cytoplasm, prominent nucleoli, fine "open" nuclear chromatin
- As cells differentiate: nucleus retains finely dispersed chromatin (does NOT condense/pyknose as normal normoblasts do)
- Cytoplasmic maturation and hemoglobin accumulation proceed normally → nuclear-cytoplasmic asynchrony
- Giant metamyelocytes and band forms in granulocytic lineage
- Abnormally large megakaryocytes with bizarre multilobate nuclei
- Despite hypercellularity, marked ineffective erythropoiesis causes peripheral cytopenias
(Robbins & Cotran, p. 609; Frameworks for Internal Medicine)
Pernicious Anemia (Special Subtype)
Pernicious anemia is a specific form of megaloblastic anemia caused by autoimmune gastritis leading to loss of gastric parietal cells and failure of intrinsic factor (IF) secretion.
Pathogenesis
- Autoreactive T-cell response initiates gastric mucosal injury → chronic atrophic gastritis → loss of parietal cells
- Three types of autoantibodies (diagnostically useful but not primary cause):
- Type I (~75%): Blocks B12 binding to intrinsic factor
- Type II (large proportion): Blocks IF-B12 complex binding to cubilin receptor (ileal)
- Type III (85-90%): Anti-gastric proton pump (H+/K+-ATPase) - less specific, seen in 50% of elderly with idiopathic gastritis
Associations
- Median age of diagnosis: 60 years (rare <30 years)
- Associated with other autoimmune diseases: autoimmune thyroiditis (Hashimoto's), type 1 DM, vitiligo, adrenal insufficiency (Addison's)
- Increased risk of gastric carcinoid tumors and adenocarcinoma (screening endoscopy recommended)
- Higher prevalence in people of African and Northern European ancestry
Normal Cobalamin Absorption (relevant to PA)
- Food proteins digested by pepsin → free B12 binds haptocorrin (salivary R-protein) in stomach
- In duodenum, pancreatic proteases cleave haptocorrin → free B12 binds intrinsic factor (IF, from gastric parietal cells)
- IF-B12 complex travels to terminal ileum → binds cubilin receptor → endocytosed
- Within ileal cells, B12 binds transcobalamin II (TC-II) → secreted into plasma
- TC-II delivers B12 to liver and rapidly proliferating cells (marrow, GI tract)
(Robbins & Cotran, p. 609-610)
Neurological Manifestations of B12 Deficiency
Subacute combined degeneration (SCD) of the spinal cord is the hallmark neurological complication. It affects the:
- Posterior columns (dorsal): loss of proprioception, vibration sense → sensory ataxia, positive Romberg sign
- Lateral (corticospinal) tracts: upper motor neuron signs → spasticity, brisk reflexes (except at ankles where LMN loss predominates)
Clinical progression:
- Symmetric paresthesias (lower limbs > upper limbs)
- Loss of vibration and position sense
- Ataxia (gait disturbance)
- Spastic paraparesis
- Cognitive impairment, personality changes, dementia ("megaloblastic madness")
- Optic atrophy (rare)
Key points:
- Neurological disease can occur without anemia (and may be the presenting feature)
- The severity of myeloneuropathy is inversely related to the severity of megaloblastic anemia
- Folate does NOT correct neurological deficits (may worsen them) - this is critical clinically
- Myelopathy is reversible if treated early; established damage may be permanent
(Goldman-Cecil, Ch. 150)
Clinical Features
Symptoms
- Anemia: fatigue, pallor, dyspnea on exertion, palpitations
- Glossitis: "beefy red," smooth, sore tongue (Hunter's glossitis)
- GI symptoms: nausea, anorexia, malabsorption (GI tract cells also megaloblastic)
- Neurological (B12 only): paresthesias, ataxia, weakness, cognitive decline
- Skin: patchy hyperpigmentation
- Jaundice: from intramedullary hemolysis
Signs
- Pallor, mild jaundice (lemon-yellow tinge)
- Smooth, atrophic tongue
- Splenomegaly (mild, from extramedullary hematopoiesis)
- Neurological examination: loss of vibration/proprioception, positive Romberg, brisk knee reflexes, absent ankle reflexes (in SCD)
Investigations
Blood Count and Smear
- MCV markedly elevated (>100 fL, often >115 fL)
- Hemoglobin reduced (may be severely low)
- Pancytopenia in severe cases (leukopenia + thrombocytopenia)
- Peripheral smear: macro-ovalocytes, hypersegmented neutrophils
Key Biochemical Tests
| Test | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Serum B12 | Low (<200 pg/mL) | Normal |
| Serum folate | Normal | Low |
| Red cell folate | Low (secondary trap) | Low (more reliable) |
| Serum homocysteine | Elevated | Elevated |
| Methylmalonic acid (MMA) | Elevated (most specific for B12) | Normal |
| Serum LDH | Markedly elevated | Elevated |
| Indirect bilirubin | Elevated | Elevated |
| Haptoglobin | Low | Low |
MMA is the most sensitive and specific marker of cobalamin deficiency. Normal MMA in the setting of elevated homocysteine points to folate deficiency.
Bone Marrow Aspiration
- Hypercellular marrow with megaloblastic changes
- Nuclear-cytoplasmic dyssynchrony
- Giant metamyelocytes and band forms
- Performed to exclude myelodysplasia/leukemia if diagnosis is uncertain
Additional Tests for Pernicious Anemia
- Anti-intrinsic factor antibodies (Type I - highly specific, ~50% sensitive)
- Anti-parietal cell antibodies (Type III - sensitive, less specific)
- Serum gastrin: elevated (loss of parietal cell acid → loss of feedback inhibition)
- Endoscopy with gastric biopsy: confirms atrophic gastritis, screens for gastric malignancy
- Note: The Schilling test is no longer available
(Goldman-Cecil, Ch. 150; Katzung Pharmacology)
Differential Diagnosis
Other Causes of Macrocytosis (Non-megaloblastic)
- Alcohol abuse / chronic liver disease (round macrocytes, not oval)
- Hypothyroidism
- Reticulocytosis (hemolytic anemia, hemorrhage)
- Drugs: hydroxyurea, zidovudine
- Myelodysplastic syndrome (may mimic megaloblastic marrow changes)
- Chronic lung disease with hypoxemia
- Cold agglutinins, paraproteinemias
Key distinguishing feature: Non-megaloblastic causes produce round macrocytes; megaloblastic anemia produces oval macro-ovalocytes and hypersegmented neutrophils.
Treatment
Vitamin B12 (Cobalamin) Deficiency
Parenteral therapy (gold standard, especially for pernicious anemia):
- Severely symptomatic: 1000 μg IM/SC daily for 7 days, then weekly for 8 weeks, then monthly
- Hydroxycobalamin retained better than cyanocobalamin; can be given every 2-4 months after loading
- Loading doses must replace the normal tissue content of 2-5 mg
High-dose oral therapy (alternative for non-PA patients or patient preference):
- 1000-2000 μg/day orally (0.5-2% absorbed by passive diffusion even without IF)
- Randomized trials show equivalent correction of anemia, MMA, and homocysteine compared to IM route
- Patients with severe disease should receive at least 2000 μg/day initially
Important: Treatment must be continued lifelong in pernicious anemia, as the underlying gastric defect persists.
Folate Deficiency
- Folic acid 1-5 mg orally daily for 4 months (until underlying cause addressed)
- Prevent during pregnancy: 400-800 μg/day periconceptionally (reduces neural tube defects)
- Address underlying cause (alcoholism, malabsorption, drug interactions)
Critical Warning
Always exclude B12 deficiency before starting folate therapy. Folic acid will correct the anemia of B12 deficiency but will NOT prevent (and may precipitate/worsen) neurological damage - a potentially catastrophic outcome.
Response to Treatment
- Reticulocytosis begins within 3-5 days of treatment (peaks at 5-7 days) - confirms diagnosis
- Hemoglobin normalizes over 4-8 weeks
- Neurological recovery: begins weeks to months after treatment; extent depends on duration and severity of deficiency
(Goldman-Cecil Medicine, Ch. 150)
Complications
- Subacute combined degeneration of spinal cord (B12 only, irreversible if untreated)
- Infertility (impaired spermatogenesis)
- Cervical pseudo-dysplasia (megaloblastic cervical cells mimic cervical intraepithelial neoplasia)
- Glossitis and GI malabsorption
- Gastric carcinoma and carcinoid tumors (pernicious anemia - 2-3x increased risk)
- Thrombosis: elevated homocysteine is a risk factor for atherosclerosis and venous thromboembolism
- Hypokalemia after treatment (rapid cellular uptake of K+ during hematopoietic recovery - can be fatal)
Summary Table: B12 vs Folate Deficiency
| Feature | Vitamin B12 Deficiency | Folate Deficiency |
|---|---|---|
| Daily requirement | 2.4 μg | 400 μg |
| Body stores | 2-5 mg (last 3-5 years) | 5-20 mg (last 3-4 months) |
| Main sources | Animal products (meat, dairy, eggs, fish) | Green leafy vegetables, legumes, organ meats |
| Common cause | Pernicious anemia; malabsorption | Alcohol abuse; poor diet; pregnancy |
| Neurological disease | Yes (SCD) | No |
| MMA elevated | Yes | No |
| Homocysteine elevated | Yes | Yes |
| Treatment | B12 IM/oral lifelong (in PA) | Folic acid oral 1-5 mg/day |
| Folate therapy for anemia | Works (hematologically) | Works |
| Folate therapy for neuro | Dangerous (worsens) | N/A |
Sources:
- Goldman-Cecil Medicine International Edition, Ch. 150 (Megaloblastic Anemia) - definitions, epidemiology, pathobiology, diagnosis, treatment
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), Ch. 14 - morphology, pernicious anemia, biochemical mechanisms
- Frameworks for Internal Medicine - clinical features, peripheral smear interpretation
- Katzung Basic and Clinical Pharmacology (16th ed.) - differential diagnosis, pharmacological treatment
This is a shared conversation. Sign in to Orris to start your own chat.