Varicose veins surgery srb
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the essential information to provide a comprehensive answer on varicose veins surgery as covered in SRB-style surgery textbooks (Bailey & Love + Pye's Surgical Handicraft). Let me compile the full answer.
Varicose Veins Surgery
(Sources: Bailey & Love's Short Practice of Surgery 28e, Pye's Surgical Handicraft 22e, Schwartz's Principles of Surgery 11e)
Definition and Anatomy
Varicose veins are tortuous, dilated superficial veins resulting from valvular incompetence. The most common site is the great saphenous vein (GSV) system (~60% of cases) due to incompetence at the saphenofemoral junction (SFJ). The small saphenous vein (SSV) is involved in ~20% of cases at the saphenopopliteal junction (SPJ).
Aetiology
- Hereditary predisposition
- Prolonged standing (occupation)
- Pregnancy (increased venous pressure)
- Previous deep vein thrombosis (secondary varicose veins)
- Obesity, increasing age, female sex
Primary varicose veins = intrinsic venous wall abnormality
Secondary varicose veins = associated with deep venous insufficiency or obstruction
Clinical Features
Symptoms: Aching, heaviness, throbbing, burning, itching. Symptoms worsen with prolonged standing and are relieved by elevation. Ankle swelling towards end of day.
Signs:
- Tortuous dilated subcutaneous veins along the GSV or SSV distribution
- Medial thigh/calf varicosities = GSV incompetence
- Posterolateral calf varicosities = SSV incompetence
- Saphena varix - dilated vein at SFJ presenting as a painless groin swelling, disappears on lying, cough impulse present (may mimic femoral hernia - distinguished by fluid thrill on percussion lower down the thigh)
Complications:
- Superficial thrombophlebitis
- Bleeding (from thin-walled varicosity)
- Lipodermatosclerosis, skin pigmentation
- Venous ulceration (medial malleolus area)
Clinical Assessment / Tests
Trendelenburg Test (Two-Stage Test)
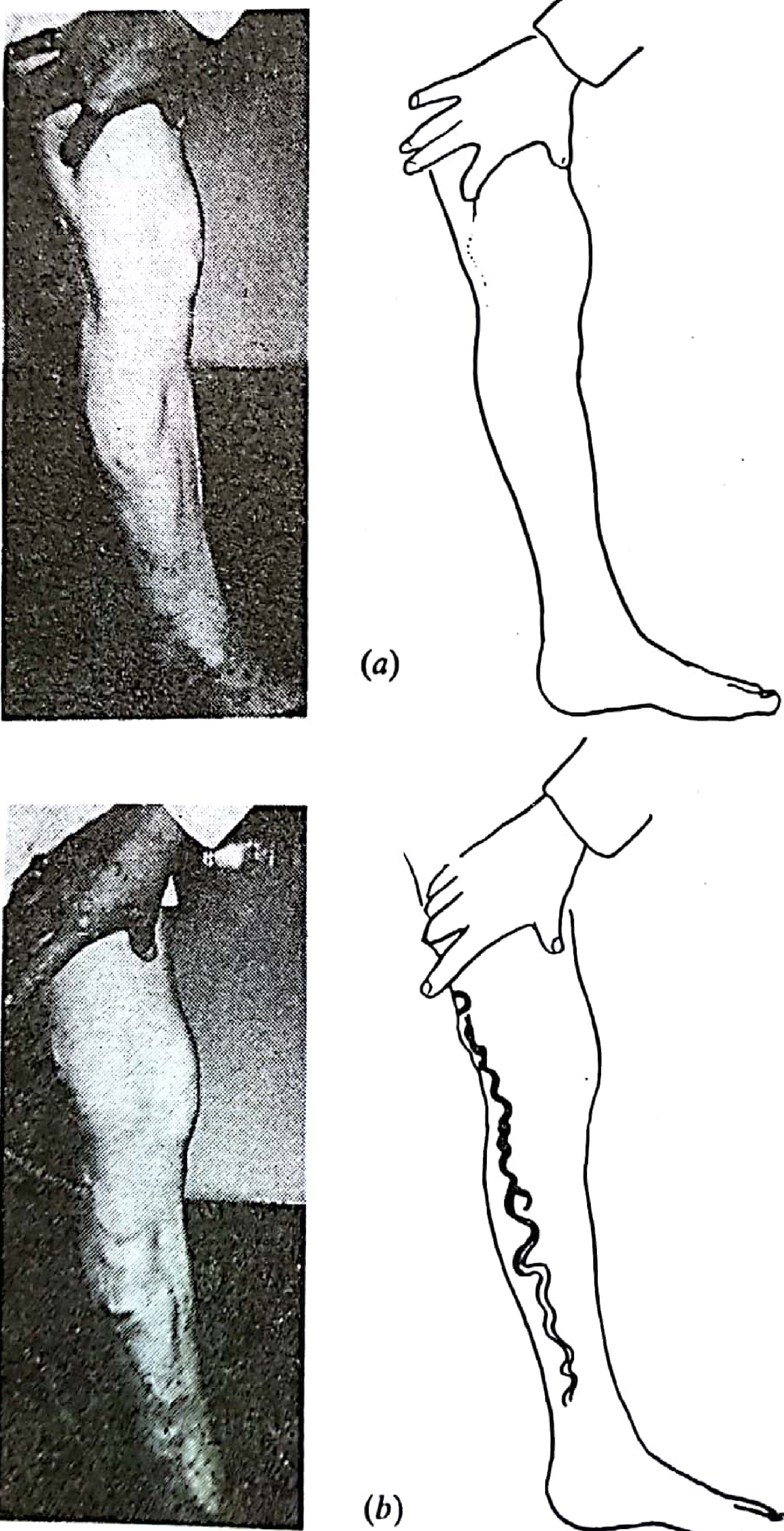
- Patient lies supine - leg elevated to drain varicose veins
- Compress the suspected incompetent proximal vein (SFJ) with thumb/tourniquet
- Patient stands up
- Tourniquet controls filling (veins stay empty) → incompetence at that level confirmed
- Release tourniquet → veins fill rapidly from above = SFJ incompetence
- If veins fill even with tourniquet in place → incompetence at a lower level (perforators)
Multiple tourniquet tests (at different levels) can localize the exact site of incompetence.
Other Tests
- Cough impulse test: Cough impulse felt over the SFJ (Sicard's sign)
- Percussion/tap test (Schwartz test): Fluid thrill transmitted along the vein column
- Hand-held Doppler: Can demonstrate reflux at junctions (largely replaced by duplex now)
Modern practice: Duplex ultrasound scanning is now the standard of care for ALL patients before any intervention. Tourniquet tests and hand-held Doppler have largely been abandoned as the sole investigation. - Bailey & Love 28e, p. 1054
Treatment
1. Conservative
- Elastic compression stockings (20-30, 30-40, or 40-50 mmHg)
- Leg elevation
- Suitable for mild disease, elderly, unfit patients
2. Injection Sclerotherapy
- Inject sclerosant (e.g., ethanolamine, sodium tetradecyl sulfate, polidocanol) into vein lumen
- Immediate firm compression bandaging for 7 days post-injection to appose inflamed walls and prevent thrombus
- Elastic stockings for minimum 2 weeks after
- Foam sclerotherapy - sclerosant whipped into foam, more effective for larger veins
- Does NOT remove the source of incompetence; higher recurrence rate than surgery
- Complications: allergy, hyperpigmentation, thrombophlebitis, DVT, skin necrosis
3. Endovenous (Minimally Invasive) Ablation - now first-line
Endovenous Laser Ablation (EVLA) and Radiofrequency Ablation (RFA):
- GSV punctured in distal thigh/proximal calf under ultrasound guidance
- Laser fiber or RFA catheter advanced to just below SFJ (not at the junction itself)
- Tumescent anaesthesia injected around the GSV
- Catheter withdrawn while delivering energy - obliterates the vein
- As effective as open surgery with faster recovery, less morbidity
- Risks: DVT, bruising, saphenous nerve injury
Mechanochemical Ablation (MOCA/ClariVein):
- Spinning wire + simultaneous liquid sclerosant injection
- No tumescent anaesthesia required
- Higher medium/long-term recanalisation rates vs. thermal ablation
Endovenous Glue (Cyanoacrylate):
- 0.1 mL applications of adhesive with vein compression
- Minimal intraprocedural pain
- Highest consumable cost
4. Open Surgery (Ligation and Stripping)
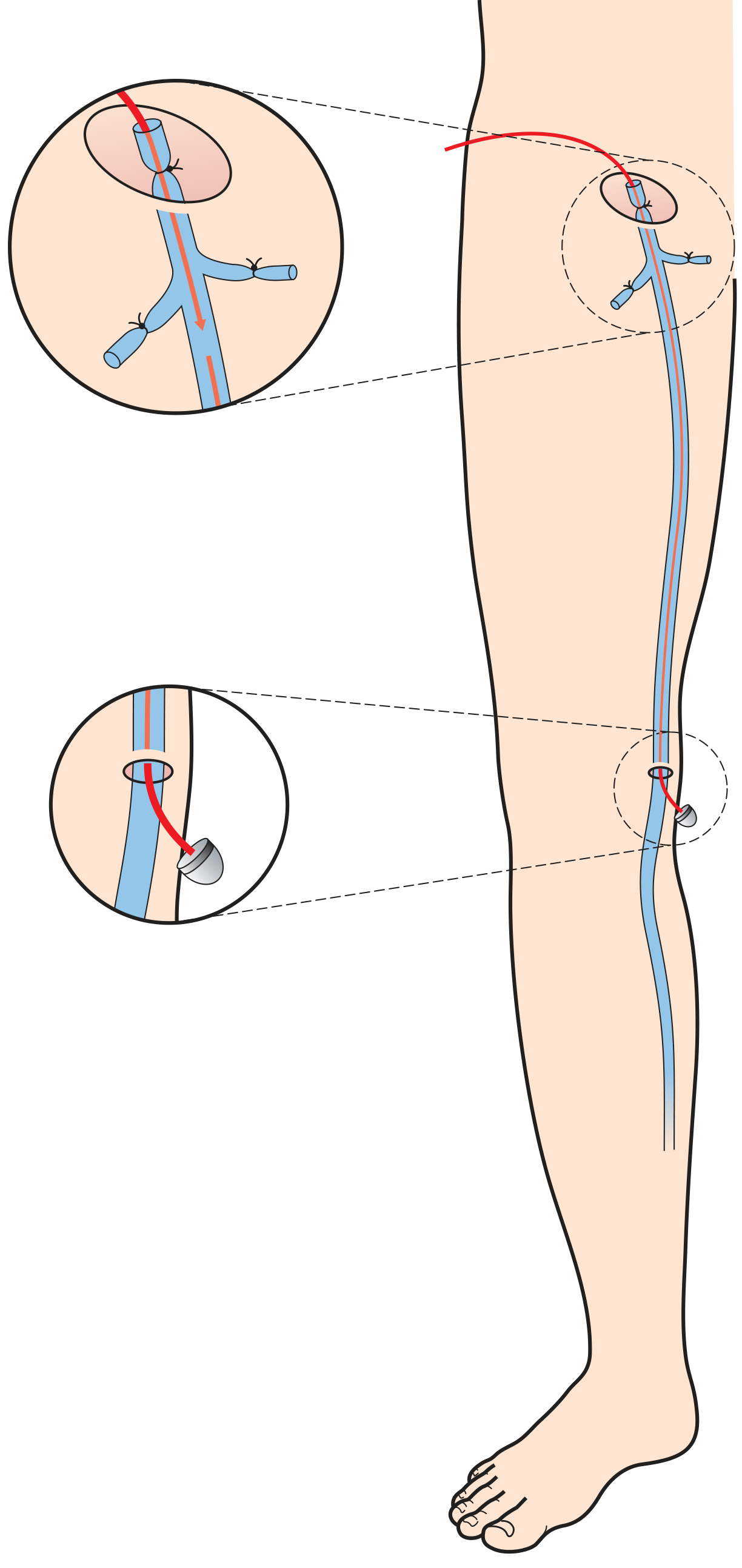
Figure: SFJ ligation with flush division and retrograde stripping of the GSV to knee level.
Still used when GSV diameter >2 cm, for recurrent disease, or when endovenous options are unavailable.
A. Saphenofemoral Junction (SFJ) Ligation + GSV Stripping
Steps:
- Incision - oblique groin incision just lateral to pubic tubercle, above groin crease
- Identify the GSV and dissect up to the SFJ (must be clearly identified to avoid inadvertent division of the common femoral vein)
- Ligate all 6 GSV tributaries at SFJ:
- Lateral: superficial inferior epigastric vein, superficial circumflex iliac vein
- Medial: superficial external pudendal vein, deep external pudendal vein
- Distal: anterior accessory GSV (AAGSV), posteromedial thigh vein
- Flush ligation of the SFJ (ligated at its junction with the femoral vein)
- Strip the GSV retrogradely from groin to knee using a blunt-tip catheter or invagination pin stripper (NOT to the ankle - lower half is rarely incompetent, and stripping below knee increases saphenous nerve injury risk)
- Phlebectomy of tributary varicosities through multiple small stab incisions
Complications of GSV stripping:
- Bruising/haematoma (very common)
- Lymphocele/lymph leak (groin wound)
- DVT
- Wound infection
- Saphenous nerve injury (paraesthesia medial calf/ankle) - most common nerve injury
- Recurrence (neovascularisation in the groin)
B. Saphenopopliteal Junction (SPJ) Ligation + SSV Stripping
- Preoperative duplex marking of the SPJ is mandatory (position highly variable)
- Patient positioned prone
- Transverse incision over the pre-marked SPJ in the popliteal fossa
- Divide the fascia, expose the SSV
- Flush ligation of SPJ or high ligation as proximally as possible
- SSV may be stripped or proximal section resected
- Sural nerve injury is the main serious complication
C. Phlebectomy (Stab Avulsion / Ambulatory Phlebectomy / Fegan's Technique)
- Mark varicosities preoperatively with patient standing
- Multiple 2 mm stab incisions directly over marked varicosities
- Vein hooked out with a phlebectomy hook and avulsed proximally and distally as far as possible
- No ligation usually needed; bleeding controlled by elevation + compression + tumescent anaesthesia
- Can be performed under local anaesthetic as sole treatment for isolated tributary incompetence
D. Subfascial Endoscopic Perforator Surgery (SEPS)
- For incompetent perforator veins (Cockett's perforators at medial ankle)
- Mainly indicated in patients with venous ulcers and proven perforator incompetence
- Performed with endoscope under tourniquet control
Indications for Surgery
- Symptomatic varicose veins unresponsive to conservative management
- Recurrent superficial thrombophlebitis
- Bleeding varicose veins
- Skin changes (lipodermatosclerosis, eczema)
- Venous ulceration with proven superficial incompetence
- Cosmetic (patient request)
Contraindications:
- Deep vein obstruction (varicose veins are compensatory)
- Ankle-brachial pressure index <0.8 (peripheral arterial disease)
- Pregnancy (operate 3 months post-delivery if veins persist)
Complications of Varicose Veins (Acute)
| Complication | Features | Treatment |
|---|---|---|
| Superficial thrombophlebitis | Tender, red, indurated cord along vein; painful | NSAIDs, compression, analgesia (7 days) |
| Bleeding | From rupture of thin-walled varix, often spontaneous | Elevation + firm pressure; rarely requires surgery |
Summary
Ultrasound-guided endovenous ablation has become the first-line treatment, minimising procedural morbidity while maintaining excellent efficacy. Open surgery (SFJ ligation + GSV stripping) remains the gold standard when endovenous options are unavailable or for very large GSVs. Phlebectomy (stab avulsion) is an important adjunct in both approaches. - Bailey & Love 28e, p. 1058
This is a shared conversation. Sign in to Orris to start your own chat.