Sedation in icu. Along with viva points
Reading File
Finding Sources
Finding Sources
Searching PubMed
"sedation" AND "ICU" AND "analgesia"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have all the information needed for a comprehensive answer. Let me compile it:
ICU Sedation - Comprehensive Review with Viva Points
1. WHY SEDATE IN THE ICU?
Critically ill patients require sedation for multiple reasons:
- Pain from injuries, procedures, and care
- Anxiety and agitation from the ICU environment (noise, lights, inability to speak)
- Ventilator dyssynchrony - facilitating mechanical ventilation compliance
- Medical conditions requiring deep sedation: Status epilepticus (SE), ARDS, refractory intracranial hypertension, abdominal compartment syndrome
Viva point: The goal is NOT to keep patients deeply sedated. The goal is MINIMUM sedation sufficient for safety and comfort. "Light sedation" (RASS 0 to -2) is now the standard target.
2. HISTORICAL SHIFT
- Pre-2000s: Benzodiazepines + opioids + neuromuscular blockade were routine. Deep sedation was the norm.
- Turn of the 21st century: Recognition that deep sedation is harmful - prolonged ventilation, delirium, ICU-acquired weakness, cognitive dysfunction.
- Modern era: Emphasis on analgesia-first (analgosedation), light sedation, daily interruption, and the PADIS/ABCDEF bundle.
3. SEDATION ASSESSMENT SCALES
Richmond Agitation-Sedation Scale (RASS)
Most widely validated and used scale.
| Score | Label | Description |
|---|---|---|
| +4 | Combative | Overtly combative, violent, immediate danger to staff |
| +3 | Very agitated | Pulls/removes tubes/catheters, aggressive |
| +2 | Agitated | Frequent nonpurposeful movement, fights ventilator |
| +1 | Restless | Anxious, apprehensive |
| 0 | Alert and calm | Target in most patients |
| -1 | Drowsy | Sustained (>10 sec) awakening with eye contact to voice |
| -2 | Light sedation | Brief (<10 sec) awakening with eye contact |
| -3 | Moderate sedation | Movement, no eye contact to voice |
| -4 | Deep sedation | No response to voice, movement to physical stimulation only |
| -5 | Unarousable | No response to voice or physical stimulation |
Target RASS: 0 to -2 for most patients. RASS -4 to -5 only for specific indications (SE, refractory ICP, ARDS with paralysis).
Other Scales
- Riker Sedation-Agitation Scale (SAS): 1-7; SAS 3-4 is the usual target
- Ramsay Scale: Historic; 6-point scale, less commonly used now
- Behavioral Pain Scale (BPS) / CPOT: For pain assessment in non-verbal patients
Viva point: RASS >+1 = risk of self-harm, self-extubation. RASS < -2 = associated with longer ICU stays and prolonged mechanical ventilation. Assess pain, sedation, AND delirium at every encounter.
4. THE PAD / PADIS FRAMEWORK
The SCCM guidelines evolved from PAD (2013) to PADIS (2018):
| Letter | Component |
|---|---|
| P | Pain |
| A | Agitation/Sedation |
| D | Delirium |
| I | Immobility (early mobilization) |
| S | Sleep disruption |
ABCDEF Bundle (ICU Liberation Bundle)
A coordinated, multidisciplinary implementation framework:
| Letter | Action |
|---|---|
| A | Assess, Prevent, and Manage Pain |
| B | Both Spontaneous Awakening Trials (SAT) and Spontaneous Breathing Trials (SBT) - coordinated daily |
| C | Choice of Analgesia and Sedation |
| D | Delirium - Assess, Prevent, Manage |
| E | Early Mobility and Exercise |
| F | Family Engagement and Empowerment |
A 2019 multicenter study of >15,000 patients showed that each 10% increase in ABCDEF bundle compliance was associated with significantly better outcomes (less delirium, coma, restraint use, and mortality).
Viva point: ABCDEF bundle implementation reduces ICU mortality, delirium, coma, mechanical ventilation days, and physical restraint use. SAT + SBT coordination is the cornerstone.
5. ANALGESIA-FIRST (ANALGOSEDATION)
Modern approach: Treat pain first before giving sedatives. Many agitated ICU patients are simply in pain.
PAD Protocol Algorithm
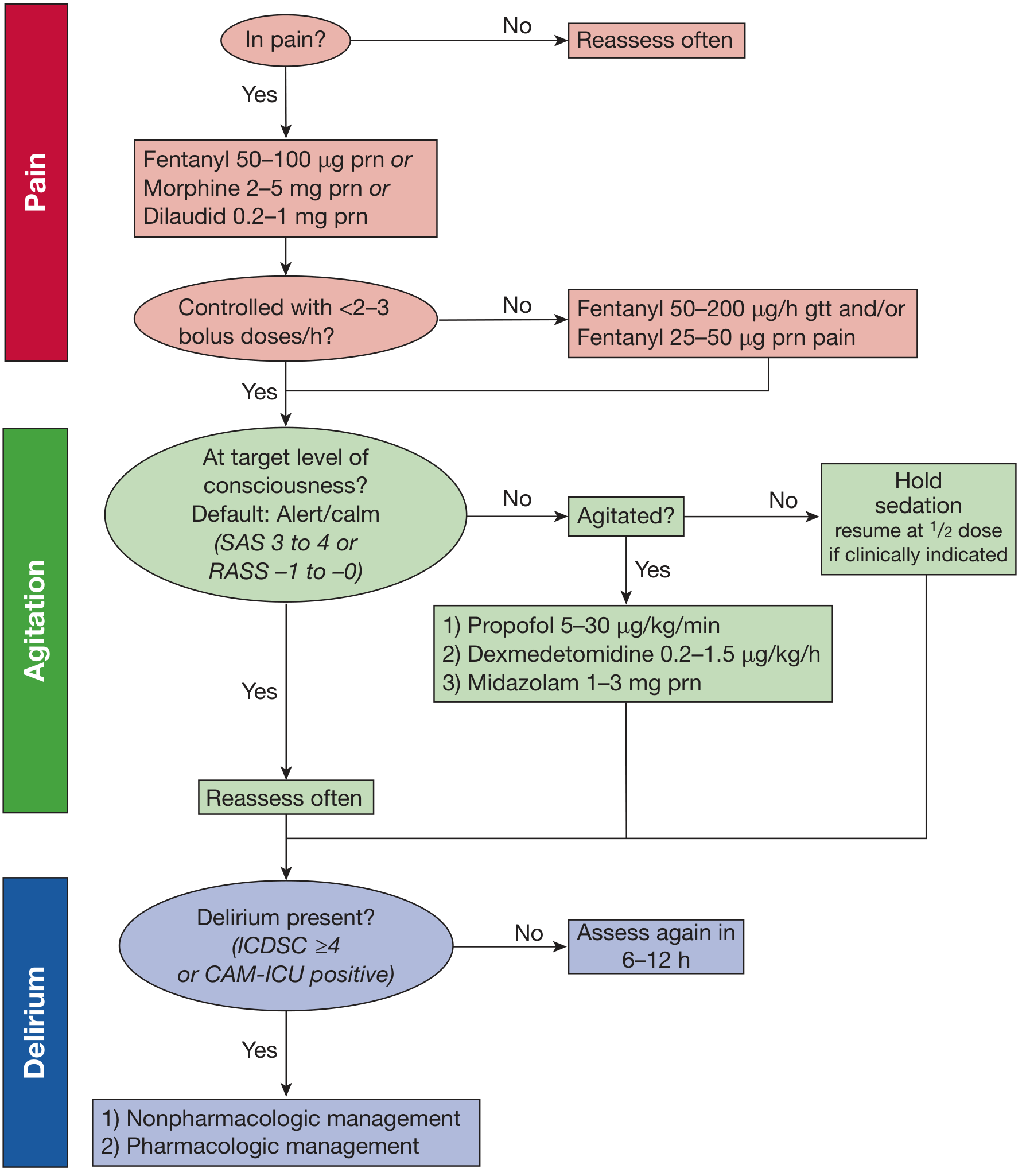
Fishman's Pulmonary Diseases and Disorders, Fig 151-2
Step 1: Assess pain → IV analgesia (fentanyl/morphine/hydromorphone) PRN
Step 2: If >3 boluses/hour needed → start fentanyl infusion
Step 3: Assess level of consciousness (RASS/SAS)
Step 4: If agitated despite analgesia → add propofol or dexmedetomidine
Step 5: Midazolam ONLY if: alcohol withdrawal, propofol intolerance, or propofol >96 hours
Step 6: Daily SAT + SBT
Step 7: Screen for delirium (CAM-ICU or ICDSC)
Opioid Analgesics in ICU
| Drug | Half-life | Intermittent Dose | Infusion Dose | Key Notes |
|---|---|---|---|---|
| Morphine | 2-3 h | 0.01-0.15 mg/kg q 1-2 h | 0.07-0.5 mg/kg/h | Avoid in renal/hepatic failure; histamine release → hypotension |
| Fentanyl | 1.5-6 h | 0.35-1.5 μg/kg q 0.5-1 h | 0.7-10 μg/kg/h | Less hypotension; accumulates in hepatic failure |
| Hydromorphone | 3-7 h | 10-30 μg/kg q 1-2 h | 7-15 μg/kg/h | Use if intolerant of morphine/fentanyl |
| Remifentanil | 3-10 min | - | 0.6-15 μg/kg/h | No accumulation in organ failure; allows rapid emergence and earlier extubation; risk of opioid-induced hyperalgesia |
Viva point: Remifentanil is the only opioid that does not accumulate in renal or hepatic failure (ester hydrolysis). Morphine metabolites (M6G) accumulate in renal failure and cause prolonged sedation.
6. SEDATIVE AGENTS
A. Propofol
- Mechanism: GABA-A receptor agonist (presumed), fat-soluble
- Onset: ~30 seconds (rapid)
- Half-life: Biphasic - 40 min initially; with prolonged infusion up to 6 days (adipose accumulation)
- Dose: Intermittent 0.2-0.6 mg/kg; Infusion 5-80 μg/kg/min
- Advantages:
- Most commonly used sedative for mechanically ventilated ICU patients
- Shorter duration of mechanical ventilation vs. benzodiazepines
- Less delirium vs. benzodiazepines
- Reliable deep sedation
- Disadvantages:
- Hypotension, myocardial depression
- Hypertriglyceridemia (lipid vehicle - contributes to caloric load)
- Propofol Infusion Syndrome (PRIS): Rare (<1%) but 33-66% mortality
- Features: Acute refractory bradycardia, metabolic acidosis, rhabdomyolysis, renal failure, hypertriglyceridemia
- Risk factors: High dose (>4 mg/kg/h), prolonged use (>48-72 h), low carbohydrate intake
- Monitor: Triglycerides every 3 days; if rising, check lipase + CK
- Predisposing: Genetic defects in fatty acid metabolism (e.g., MCAD deficiency)
Viva point (PRIS triad): Metabolic acidosis + rhabdomyolysis + cardiac failure (bradycardia progressing to asystole). Stop propofol immediately. No antidote - supportive care.
B. Dexmedetomidine
- Mechanism: Presynaptic α2-adrenoceptor agonist → inhibits noradrenergic release from locus coeruleus (reticular activating system)
- Key feature: Provides "cooperative sedation" - patient is calm but arousable and can follow commands. Unique among ICU sedatives.
- Half-life: 6 minutes (distribution); up to 6 hours in hepatic impairment
- Dose: 0.2-1.5 μg/kg/h infusion (no bolus loading recommended in ICU)
- Advantages:
- No respiratory depression at standard doses (can sedate non-intubated patients)
- May have some analgesic properties
- Reduces delirium vs. benzodiazepines
- Facilitates extubation in agitated delirious patients (DahLIA trial)
- Disadvantages:
- Does NOT reliably produce deep sedation
- Does NOT reliably produce amnesia → CANNOT be used alone in paralyzed patients
- Bradycardia and hypotension (telemetry monitoring required)
- More expensive than propofol
- Key trials:
- MENDS trial: Dexmedetomidine vs. lorazepam → more days alive and without delirium/coma
- SEDCOM trial: Dexmedetomidine vs. midazolam → less delirium, earlier extubation
- DahLIA (2016): Dex vs. placebo in agitated/delirious patients → more hours alive off ventilator
- SPICE-III (2019): Dex vs. usual care (propofol) → no mortality difference; more days free of delirium/coma with dex
- MENDS2 (2021): Dex vs. propofol in sepsis → NO difference in mortality, delirium-free days, or neurocognition
Viva point: Dexmedetomidine mechanism - locus coeruleus → "cooperative sedation." Cannot produce deep sedation or amnesia. Oral clonidine (also α2 agonist) can be used to wean off IV dexmedetomidine.
C. Benzodiazepines (Midazolam, Lorazepam)
- Mechanism: GABA-A receptor agonist (facilitate Cl- channel opening) → anxiolysis, sedation, amnesia, anticonvulsant, muscle relaxation
- Midazolam: Water-soluble; most common benzodiazepine infusion in ICU
- Sleep quality: EEG shows ↑Stage 2, ↓REM, ↑beta activity - NOT restorative sleep
- Advantages: Deep sedation + amnesia; hemodynamically stable; inexpensive; treatment of alcohol withdrawal
- Disadvantages:
- Associated with longer mechanical ventilation vs. propofol and dexmedetomidine
- Greater delirium risk
- Active metabolites accumulate in renal/hepatic failure
- Withdrawal syndrome with abrupt discontinuation
- Current role: Benzodiazepines are NO LONGER first-line. Reserved for:
- Status epilepticus
- Alcohol/benzodiazepine withdrawal
- When RASS -4 to -5 is required (ARDS, refractory ICP)
- Propofol intolerance or propofol >96 hours
Viva point: Benzodiazepine infusions should be avoided in most ICU patients. Benzodiazepines are independent risk factors for delirium. Intermittent dosing preferred over continuous infusion even when benzodiazepines are necessary.
D. Ketamine
- Mechanism: NMDA receptor antagonist (dissociative); partial μ-opioid receptor agonist
- Half-life: ~45 minutes
- Advantages:
- Bronchodilator → useful in asthma/COPD
- Sympathomimetic → maintains hemodynamics (useful in shock states)
- Anti-inflammatory (inhibits TNF-α and IL-6)
- No respiratory depression at low doses → can be used in non-intubated patients
- Historically avoided in elevated ICP, but recent evidence shows it may actually decrease ICP in TBI
- Useful as opioid-sparing adjunct (acts synergistically with opioids)
- Disadvantages:
- Tachycardia and hypertension → avoid in demand ischemia, severe tachycardia
- Increases secretions (salivation and tracheobronchial)
- Emergence phenomenon (less relevant in ICU with continuous monitoring)
E. Barbiturates (Phenobarbital, Pentobarbital, Thiopental)
- Mechanism: GABA-A activation via chloride channel (different site from benzodiazepines)
- Half-lives: 20-120 hours (extremely long)
- ICU indications: Refractory SE, refractory intracranial hypertension
- Disadvantages: Myocardial/respiratory/GI depression; immunosuppression; withdrawal syndrome
F. Antipsychotics (Haloperidol, Quetiapine, Olanzapine)
- Role: Adjunctive - augment IV sedation, facilitate weaning; treat delirium agitation
- Mechanism: Dopamine antagonism (+ antihistamine, anticholinergic, anti-noradrenergic effects)
- Haloperidol IV: Onset 5-20 min; duration 4-12 hours
- Key safety concern: QTc prolongation → risk of torsades de pointes (most concerning with IV haloperidol)
- Evidence: NO evidence that antipsychotics reduce mortality, mechanical ventilation duration, ICU LOS, or hospital discharge time
- Important: Older patients have higher mortality risk with both typical and atypical antipsychotics
Viva point: Antipsychotics do NOT reduce delirium duration or mortality in ICU. They are used only for managing agitation/behavioral disturbance. Always monitor QTc with IV haloperidol.
7. DAILY INTERRUPTION OF SEDATION (DIS) / SAT
- Kress et al. (2000, NEJM): Landmark trial showing daily interruption of sedation → shorter mechanical ventilation and ICU LOS
- Method: Stop sedative infusions each morning. Reassess. If patient comfortable at RASS 0 to -1, do NOT restart. If agitated, restart at HALF the previous dose.
- Coordinate SAT with SBT: Patients who wake up AND pass a breathing trial → earlier extubation
- Caveat: If deeply sedated for medical reasons (RASS -4/-5: SE, ARDS, ICP), do NOT interrupt
Viva point: Patients managed with continuous infusions of benzodiazepines who never wake up may appear to have poor neurological prognosis, leading families to withdraw care - a "self-fulfilling prophecy" that can be avoided with lighter sedation and shorter-acting agents.
8. DELIRIUM IN ICU
- Definition (DSM-5): Acute disturbance in attention/awareness + cognition; fluctuating; due to an underlying medical condition
- Most common subtype: Hypoactive (quiet) delirium - often missed!
- Subtypes:
- Hyperactive (10%) - agitated, combative
- Hypoactive (45%) - withdrawn, lethargic
- Mixed (45%)
- Consequences: Increased ICU/hospital LOS, cognitive impairment, PTSD, long-term dementia
- Assessment Tools:
- CAM-ICU (Confusion Assessment Method for ICU) - Features: (1) Acute onset + fluctuating course, (2) Inattention, (3) Altered LOC OR (4) Disorganized thinking. Positive = features 1+2 AND either 3 or 4
- ICDSC (Intensive Care Delirium Screening Checklist) - Score ≥4 = delirium
Viva point (CAM-ICU): CAM-ICU requires: acute onset + inattention PLUS altered LOC OR disorganized thinking. Can be performed in non-verbal/intubated patients. ICDSC ≥4 is also diagnostic.
- Prevention and treatment of delirium:
- First: Find and treat underlying cause (hypoxia, infection, electrolytes, drug withdrawal, pain)
- Non-pharmacologic: Reorientation, early mobilization, sleep hygiene, minimize anticholinergics, minimize benzodiazepines
- Pharmacologic: Antipsychotics for agitation (not for prevention/treatment of delirium itself)
9. SEDATION FOR SPECIAL CONDITIONS
| Condition | Preferred Sedation | Avoid |
|---|---|---|
| ARDS (prone positioning, paralysis) | Deep sedation: Benzodiazepine ± propofol | Light sedation |
| Status Epilepticus | Midazolam, phenobarbital, propofol infusion, thiopental | - |
| Refractory ICP | Midazolam, propofol, barbiturate coma | Ketamine (historically, though less concern now) |
| Alcohol withdrawal | Benzodiazepines (lorazepam/diazepam) | Propofol alone |
| Hemodynamically unstable | Ketamine; cautious dexmedetomidine | Propofol (hypotension), midazolam |
| Hepatic failure | Remifentanil (safest) | Morphine, midazolam (accumulate) |
| Renal failure | Remifentanil, fentanyl | Morphine (M6G accumulates), hydromorphone |
| Non-intubated agitation | Dexmedetomidine, ketamine (no resp. depression) | Propofol, benzodiazepines |
10. KEY PHARMACOLOGY COMPARISON TABLE
| Drug | Mechanism | Deep Sedation? | Amnesia? | Resp. Depression? | Analgesia? |
|---|---|---|---|---|---|
| Propofol | GABA-A agonist | ✅ Yes | Partial | ✅ Yes | ❌ No |
| Midazolam | GABA-A agonist | ✅ Yes | ✅ Yes | ✅ Yes | ❌ No |
| Dexmedetomidine | α2 agonist | ❌ No | ❌ No | ❌ Minimal | Partial |
| Ketamine | NMDA antagonist | Dissociative | ✅ Yes | ❌ No | ✅ Yes |
| Barbiturates | GABA-A (Cl- channel) | ✅ Yes | ✅ Yes | ✅ Yes | ❌ No |
11. VIVA POINTS SUMMARY
-
Analgesia-first (analgosedation) - treat pain before giving sedatives. Many "agitated" ICU patients simply have uncontrolled pain.
-
Target RASS 0 to -2 for most ICU patients. RASS -4 to -5 only for specific medical indications.
-
Benzodiazepines are NO longer first-line for ICU sedation. Propofol or dexmedetomidine preferred.
-
Dexmedetomidine = only ICU sedative that allows arousal and cooperation (no deep sedation, no amnesia). Acts on locus coeruleus. Monitor for bradycardia.
-
PRIS features: Metabolic acidosis + rhabdomyolysis + refractory bradycardia + elevated TGs. Mortality 33-66%. Monitor TGs every 3 days on propofol.
-
Propofol vs. dexmedetomidine: Both superior to benzodiazepines. SPICE-III and MENDS2 show NO difference in mortality between propofol and dexmedetomidine.
-
Remifentanil: Only opioid with no organ accumulation (ester hydrolysis). Rapid offset. Risk of opioid-induced hyperalgesia.
-
CAM-ICU: Acute onset + inattention + (altered LOC OR disorganized thinking) = positive for delirium.
-
ABCDEF bundle: Coordinated multimodal approach; each 10% improvement in compliance reduces ICU mortality, delirium, coma, and readmission.
-
Daily SAT + SBT coordination: Patients who can wake up AND breathe spontaneously can be extubated earlier - the most important practice to reduce ventilator days.
-
Deep sedation as a "self-fulfilling prophecy": Patients who don't wake up on heavy sedation may have care withdrawn for apparent poor neurological prognosis - avoidable with lighter sedation and short-acting agents.
-
Ketamine is now considered safe in TBI (may decrease ICP). It is a bronchodilator - useful in asthma/COPD. Avoid in demand ischemia and tachycardia.
-
Antipsychotics do NOT improve ICU outcomes (no change in ventilator days, mortality, LOS). Used only for behavioral agitation control. Monitor QTc.
-
Delirium subtypes: Hypoactive (most common, most missed), hyperactive (most recognized), mixed.
-
Barbiturates have half-lives of 20-120 hours - reserved for refractory SE and refractory ICP. Immunosuppressive.
Sources: Fischer's Mastery of Surgery 8e (p.458-463), Fishman's Pulmonary Diseases & Disorders (Ch.151), Barash's Clinical Anesthesia 9e (p.4857-4858), Miller's Anesthesia 10e | Recent evidence: PADIS guideline implementation meta-analysis (Crit Care Med 2024, PMID 38193764)
This is a shared conversation. Sign in to Orris to start your own chat.