Rheumatic heart disease according to Harrison and its management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"rheumatic heart disease" management
Loading Image
I now have all the content needed. Here is the comprehensive answer from Harrison's 22nd Edition (2025):
Rheumatic Heart Disease — Harrison's Principles of Internal Medicine, 22nd Ed (2025)
Overview & Pathogenesis
Acute rheumatic fever (ARF) is a multisystem inflammatory condition triggered by pharyngeal infection with group A Streptococcus (Streptococcus pyogenes). Rheumatic heart disease (RHD) is its most serious sequela, caused by damage to cardiac valves from the immune-mediated inflammation of ARF. The mechanism is molecular mimicry: streptococcal antigens share epitopes with cardiac tissue, triggering cross-reactive antibodies that damage the endocardium, myocardium, and pericardium.
Global Burden
Approximately 45–50 million people (575.5 per 100,000) live with RHD worldwide, with an estimated 300,000 new cases and 233,000 case-fatalities per year. The highest prevalence and age-adjusted mortality are in sub-Saharan Africa, South Asia, Central Asia, and Oceania. RHD accounts for 12–65% of hospital admissions for cardiovascular disease in some endemic countries. While age-standardized mortality declined ~50% between 1990 and 2022, the prevalence of heart failure attributable to RHD increased by nearly 90% over the same period.
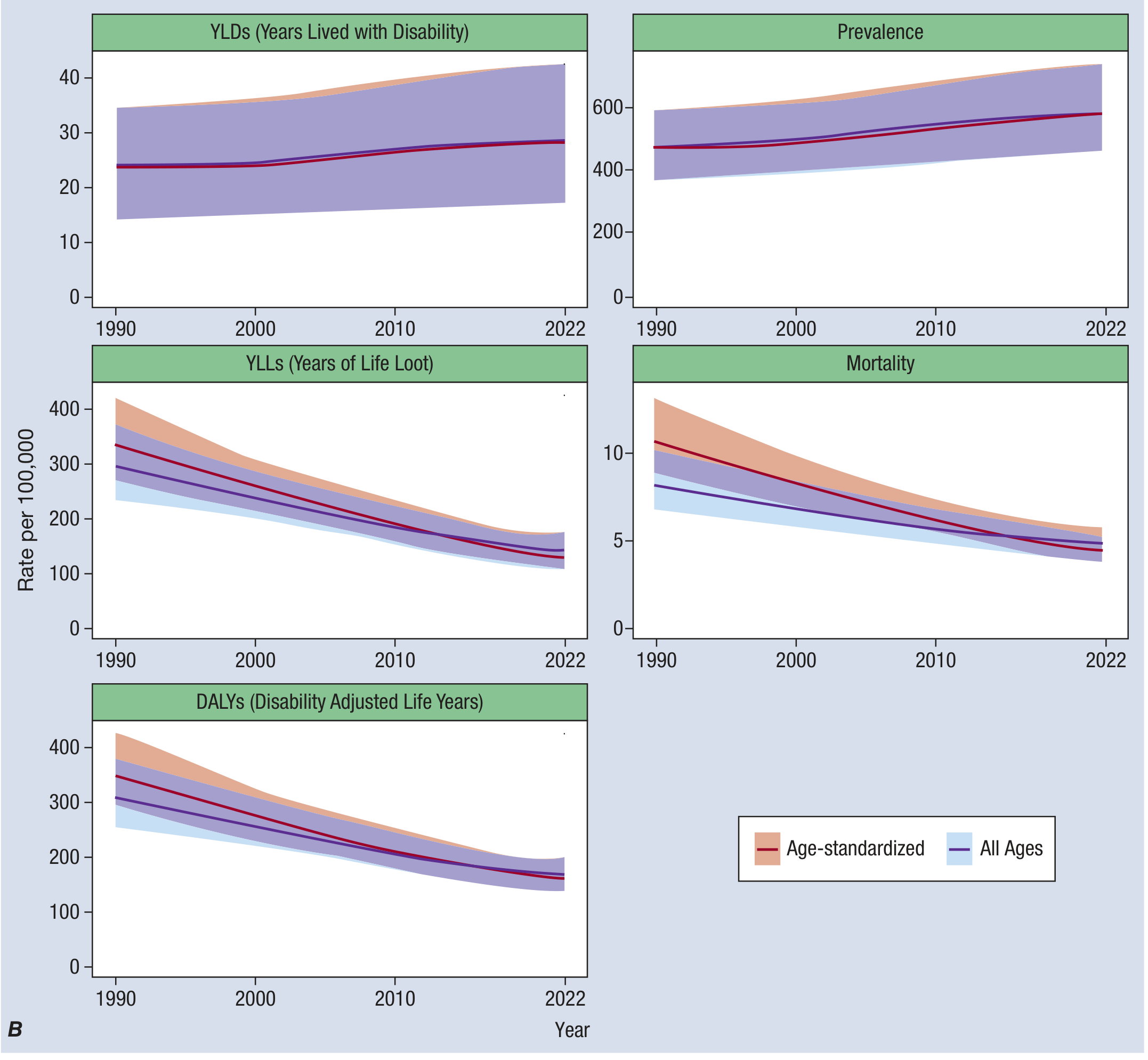
Figure: Global RHD estimates by measure, 1990–2022. Note divergence between declining mortality and rising prevalence (Harrison's, Ch. 272 & 371)
Clinical Manifestations of ARF (the Precursor)
ARF presents with the modified Jones Criteria:
Major criteria: Carditis (clinical or subclinical/echocardiographic), migratory polyarthritis, chorea (Sydenham's), erythema marginatum, subcutaneous nodules
Minor criteria: Fever, elevated ESR/CRP, prolonged PR interval
Required: Evidence of preceding GAS infection (positive throat culture, rapid Ag test, or elevated/rising streptococcal antibody titers)
Key points from Harrison's:
- Carditis is the most dangerous manifestation — presents as pancarditis (endo-, myo-, pericarditis). Mitral and aortic regurgitation are the most common valvular lesions acutely.
- Subclinical carditis (detected only by echocardiography) is now recognized as equivalent to clinical carditis for diagnostic purposes in high-prevalence settings.
- Chorea occurs predominantly in females with a prolonged latent period after GAS infection; >50% of chorea cases have associated carditis.
- Erythema marginatum is evanescent, non-facial, begins as pink macules clearing centrally with a serpiginous edge.
- Subcutaneous nodules appear 2–3 weeks after disease onset, are painless, overlie bony prominences, and are strongly associated with carditis.
Echocardiographic Staging of RHD (Harrison's Table 371-1)
| Stage | Who | Risk | Echo Features |
|---|---|---|---|
| A (Minimal) | ≤20 yrs only | Might be at risk of progression | Mild MR or AR without morphologic features |
| B (Mild) | Any age | Moderate/high risk of progression | Mild regurgitation + ≥1 morphologic feature (≤20 yrs) or ≥2 features (>20 yrs); or mild MR + mild AR |
| C (Advanced, asymptomatic) | Any age | High risk of clinical complications | Moderate/severe MR or AR, any MS or AS, pulmonary HTN, decreased LV systolic function |
| D (Advanced, symptomatic) | Any age | Established complications | Same echo features as C + surgery, heart failure, arrhythmia, stroke, or infective endocarditis |
Management
A. Treatment of Acute ARF
1. Antibiotics (eradicate GAS)
- Benzathine penicillin G: single IM dose — 1.2 million units (or 600,000 units if ≤27 kg) preferred
- Oral alternatives: Phenoxymethyl penicillin 500 mg (250 mg <27 kg) PO twice daily × 10 days; or amoxicillin 50 mg/kg (max 1 g) daily × 10 days
- For penicillin allergy: erythromycin or a cephalosporin
2. Anti-inflammatory therapy (arthritis/fever)
- Aspirin: 50–80 mg/kg/day in 4–5 divided doses (up to 100 mg/kg/day, max 8 g/day in adults). Monitor for salicylate toxicity (nausea, tinnitus).
- Naproxen 10–20 mg/kg/day (twice-daily dosing, potentially safer than aspirin) — preferred by many clinicians.
- Duration: higher doses for ~2 weeks, then taper over 2–4 weeks. Rebound symptoms after stopping do not indicate recurrence.
3. Carditis / Heart Failure
- Glucocorticoids: Role remains controversial. Two meta-analyses failed to show benefit over placebo or salicylates for long-term carditis outcomes (all studies >40 years old). Recent data suggest corticosteroids improve echocardiographic parameters in carditis.
- If used for severe carditis with heart failure: prednisone/prednisolone 1–2 mg/kg/day (max 80 mg/day), typically a few days up to 3 weeks.
- Standard heart failure management (see Harrison's Ch. 265) — may be lifesaving.
4. Chorea
- Mild: calm environment is sufficient.
- Severe: carbamazepine or sodium valproate preferred over haloperidol. Continue for 1–2 weeks after symptoms resolve.
- Corticosteroids are effective for severe/refractory chorea (prednisone 0.5 mg/kg/day, weaning after ~1 week).
- IVIg: may hasten resolution of chorea; not recommended for carditis. Reserved for severe chorea refractory to other treatment.
5. Bed Rest
- Traditional long-term bed rest is no longer routinely recommended.
- Rest prescribed only while arthritis/arthralgia present and during heart failure; mobilize gradually when symptoms controlled.
B. Secondary Prophylaxis
The cornerstone of RHD control. Because patients with a history of ARF are at dramatically higher risk of further ARF episodes with each subsequent GAS infection, long-term penicillin prophylaxis is essential.
Drug of choice: Benzathine penicillin G 1.2 million units IM (600,000 units if ≤27 kg) every 4 weeks
- Can be given every 3 weeks or even 2 weeks for highest-risk patients (though not needed when 4-week compliance is achieved)
- Evidence has emerged that subcutaneous delivery is an acceptable and better-tolerated alternative to IM injection
Oral alternative (if IM not feasible): Oral phenoxymethyl penicillin twice daily — less reliable due to adherence issues.
For penicillin allergy: sulfadiazine, or erythromycin/azithromycin
Duration of prophylaxis (Harrison's):
| Patient Category | Duration |
|---|---|
| ARF without carditis | 5 years after last episode, or until age 21 (whichever is longer) |
| ARF with mild carditis (mild residual valvular disease) | 10 years after last episode, or until age 21 |
| ARF with persistent valvular disease (moderate/severe) | 10 years after last episode, or until age 40 — sometimes lifelong |
A 2024 Cochrane systematic review (PMID 39312290) confirmed that long-term antibiotic prophylaxis prevents recurrence and progression to RHD, supporting these guidelines.
C. Primary Prevention
- Timely antibiotic treatment of GAS pharyngitis: a full course of penicillin commenced within 9 days of onset prevents almost all cases of ARF that would otherwise develop.
- In resource-limited endemic settings where microbiologic diagnosis is unavailable: clinical algorithms or empiric treatment of high-risk sore throats.
- Treatment and prevention of GAS skin infections (impetigo) is increasingly important where skin infections are a major ARF trigger (e.g., Indigenous Australian communities).
- GAS vaccine: international efforts ongoing; not yet available.
D. Management of Chronic RHD (Valvular Disease)
Once RHD has caused significant valvular disease, management follows the principles of valvular heart disease (Harrison's Ch. 272):
Mitral stenosis (MS) — most common chronic RHD lesion:
- Medical: rate control for atrial fibrillation (beta-blockers, digoxin); anticoagulation (warfarin) for AF or prior embolism; diuretics for pulmonary congestion
- Intervention: Percutaneous mitral balloon commissurotomy (PMBC) is preferred for pliable, non-calcified valves without significant MR — achievable in young patients with pure MS. Surgical mitral valve replacement if anatomy unfavorable.
Mitral regurgitation (MR) — common in ARF; may be acute or chronic:
- Severe symptomatic: surgical repair/replacement
- Asymptomatic severe MR: surgery when LV ejection fraction falls to ≤60% or LVESD >40 mm
Aortic stenosis (AS) / Aortic regurgitation (AR) — less common:
- Rheumatic AS/AR: surgical aortic valve replacement generally preferred (anatomy often not ideal for TAVI in rheumatic disease; bicuspid/rheumatic valve anatomy listed as a factor favoring SAVR over TAVI in Harrison's Table 272-3)
Infective endocarditis prophylaxis: recommended for high-risk procedures in patients with RHD-related valvular disease.
E. Investigations in Suspected ARF/RHD
Per Harrison's Table 371-3:
| Always request | Situational |
|---|---|
| ECG, Echocardiogram | Throat/skin swab |
| CBC, CRP | Blood cultures |
| ASO + anti-DNase B titers | Synovial fluid aspirate |
| Pregnancy test | |
| Creatinine (before NSAIDs) | |
| Autoantibodies, anti-dsDNA, anti-CCP (to exclude alternatives) | |
| Serology for viral hepatitis, CMV, parvovirus B19, Ross River virus |
Prognosis
Untreated ARF lasts ~12 weeks. With treatment, hospital discharge within 1–2 weeks. Inflammatory markers normalize in 4–6 weeks; follow-up echocardiogram at 1 month. Rebound of symptoms after stopping anti-inflammatories (up to 3 weeks) does not indicate recurrence.
The risk of developing chronic RHD is directly related to the severity of carditis at initial ARF episode and the number of recurrences — making secondary prophylaxis adherence the single most impactful intervention in preventing progression to severe valvular disease.
Sources: Harrison's Principles of Internal Medicine, 22nd Ed (2025), Chapters 272 (Valvular Heart Disease) and 371 (Acute Rheumatic Fever). Recent evidence: Cochrane review on secondary prophylaxis [PMID 39312290, 2024]; benzathine penicillin G adverse reactions meta-analysis [PMID 40333929, 2025].
This is a shared conversation. Sign in to Orris to start your own chat.