Anemia examination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Here is a comprehensive guide to the examination of anemia, drawn from Harrison's Principles of Internal Medicine, Rosen's Emergency Medicine, and Goldman-Cecil Medicine.
Examination of Anemia
Definition
Anemia is defined by hemoglobin below the normal range for age, sex, and altitude:
| Age/Sex | Hemoglobin (g/dL) | Hematocrit (%) |
|---|---|---|
| Adult man | 16 ± 2 | 47 ± 6 |
| Adult woman (menstruating) | 13 ± 2 | 40 ± 6 |
| Adult woman (postmenopausal) | 14 ± 2 | 42 ± 6 |
| During pregnancy | 12 ± 2 | 37 ± 6 |
| Childhood | 12 | 36 |
Step 1: History
Symptoms of anemia:
- Fatigue, weakness, dizziness, syncope
- Dyspnea, decreased exercise tolerance
- Chest pain (ischemia in patients with atherosclerosis)
- Pica (iron deficiency) or peripheral neuropathy (B12 deficiency)
Bleeding history:
- Epistaxis, hemoptysis, hematemesis, melena, hematochezia, hematuria
- Menstrual history: duration, pad/tampon count, clots
- Bleeding after trauma, tooth extractions, injections
Dietary and social history:
- Vegetarianism, poor nutrition
- Alcohol use, toxin/drug exposure
Medical/family history:
- Previous anemia, transfusions, iron supplements
- Racial background (thalassemia, sickle cell risk)
- Underlying disease: uremia, liver disease, hypothyroidism, cancer, rheumatic or renal disease
- Previous surgery
Step 2: Physical Examination
Vital signs (serial monitoring in acute anemia):
- Blood pressure, pulse, respiratory rate, oxygen saturation
- Orthostatic changes suggest significant volume depletion
Skin:
- Pallor, jaundice, diaphoresis, cyanosis
- Purpura, petechiae, ecchymoses, angiomas, telangiectasias, ulcerations
Eyes:
- Pale conjunctiva (most reliable sign of pallor)
- Icteric sclera (hemolysis)
Mouth:
- Glossitis, tongue atrophy, papillary soreness → B12/folate deficiency
Cardiovascular:
- Resting tachycardia (compensation)
- Flow murmur (high-output state)
- S3 or S4, signs of heart failure
Abdomen:
- Hepatomegaly, splenomegaly → hemolysis, hematologic malignancy
- Right upper quadrant tenderness → hemolysis with bilirubin stones
- Rectal exam: heme-positive stool (blood loss)
Neurologic:
- Decreased vibratory sensation / proprioception, ataxia → B12 deficiency
- Peripheral neuritis
Lymph nodes:
- Lymphadenopathy → systemic hematologic disease (lymphoma, leukemia)
Facial features:
- Frontal bossing → hemoglobinopathy / thalassemia
Step 3: Laboratory Testing
Complete Blood Count (CBC) with Indices
The most important initial test. Key parameters:
| Index | Formula | Normal Values |
|---|---|---|
| MCV (mean corpuscular volume) | Hct / RBC × 10 | 85–95 fL |
| MCHC | Hgb / Hct × 100 | 33.8–34.2 g/dL |
| MCH | Hgb / RBC × 10 | 28.5–32.3 pg |
| RDW | SD or CV of RBC size distribution | Marker of anisocytosis |
MCV-based classification is the primary diagnostic framework:
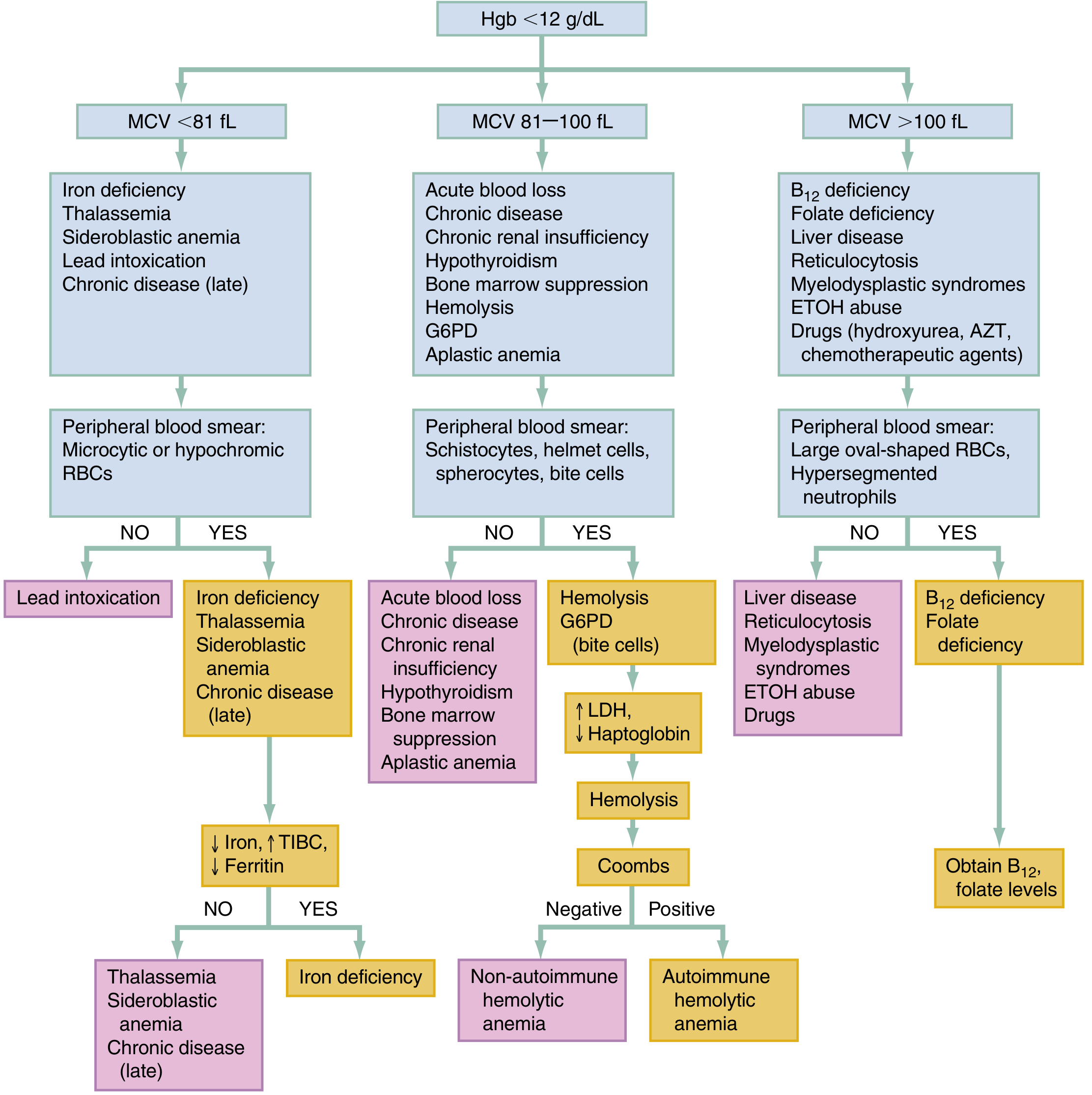
MCV Classification
| MCV | Type | Common Causes |
|---|---|---|
| < 81 fL (Microcytic) | Hypochromic | Iron deficiency, thalassemia, sideroblastic anemia, lead intoxication, chronic disease (late) |
| 81–100 fL (Normocytic) | Normal size | Acute blood loss, chronic disease, chronic renal insufficiency, hypothyroidism, aplastic anemia, hemolysis, G6PD |
| > 100 fL (Macrocytic) | Large cells | B12 deficiency, folate deficiency, liver disease, reticulocytosis, myelodysplastic syndromes, ETOH abuse, drugs (hydroxyurea, AZT, chemo) |
Peripheral Blood Smear
A crucial complement to CBC indices. Key morphological findings:
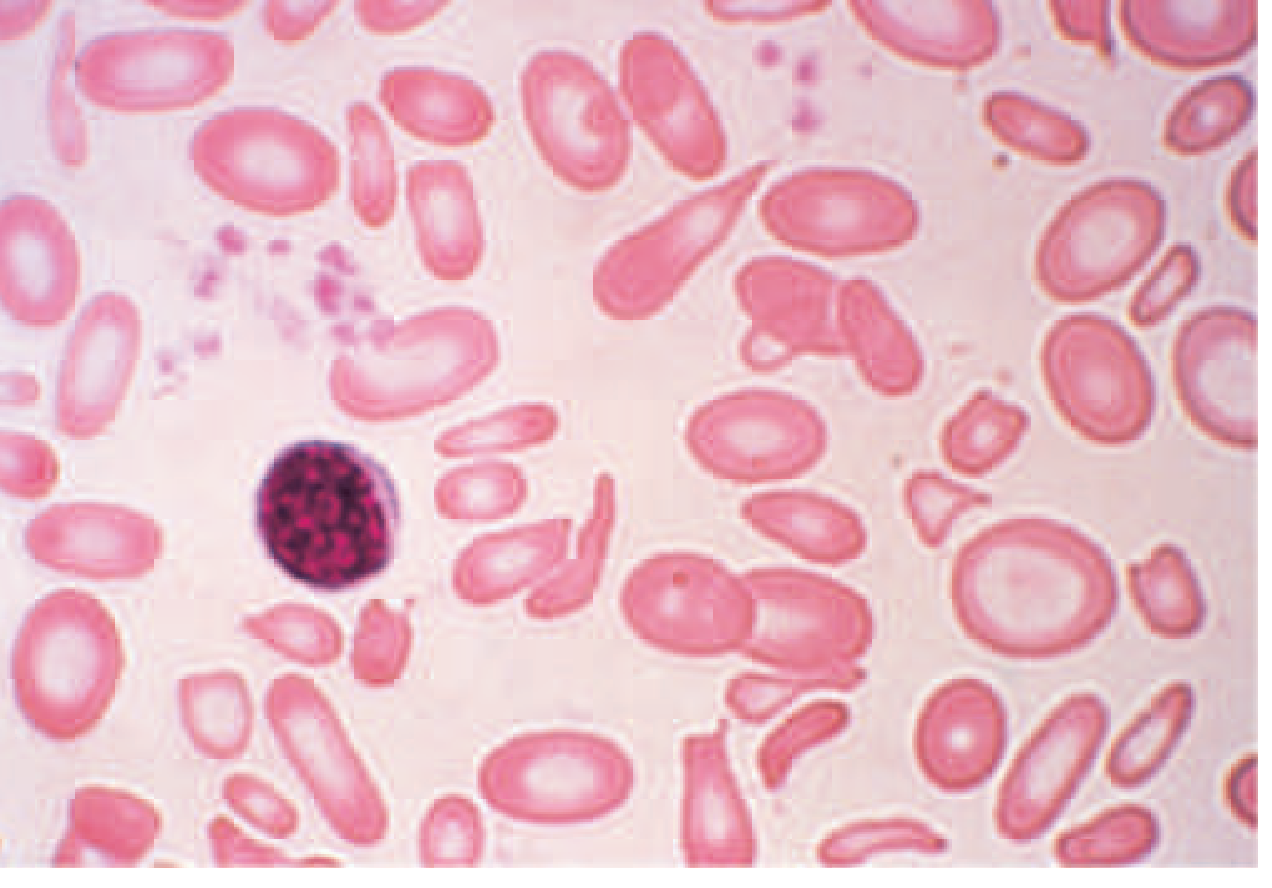
Severe iron-deficiency anemia — microcytic, hypochromic cells with marked anisocytosis and poikilocytosis:
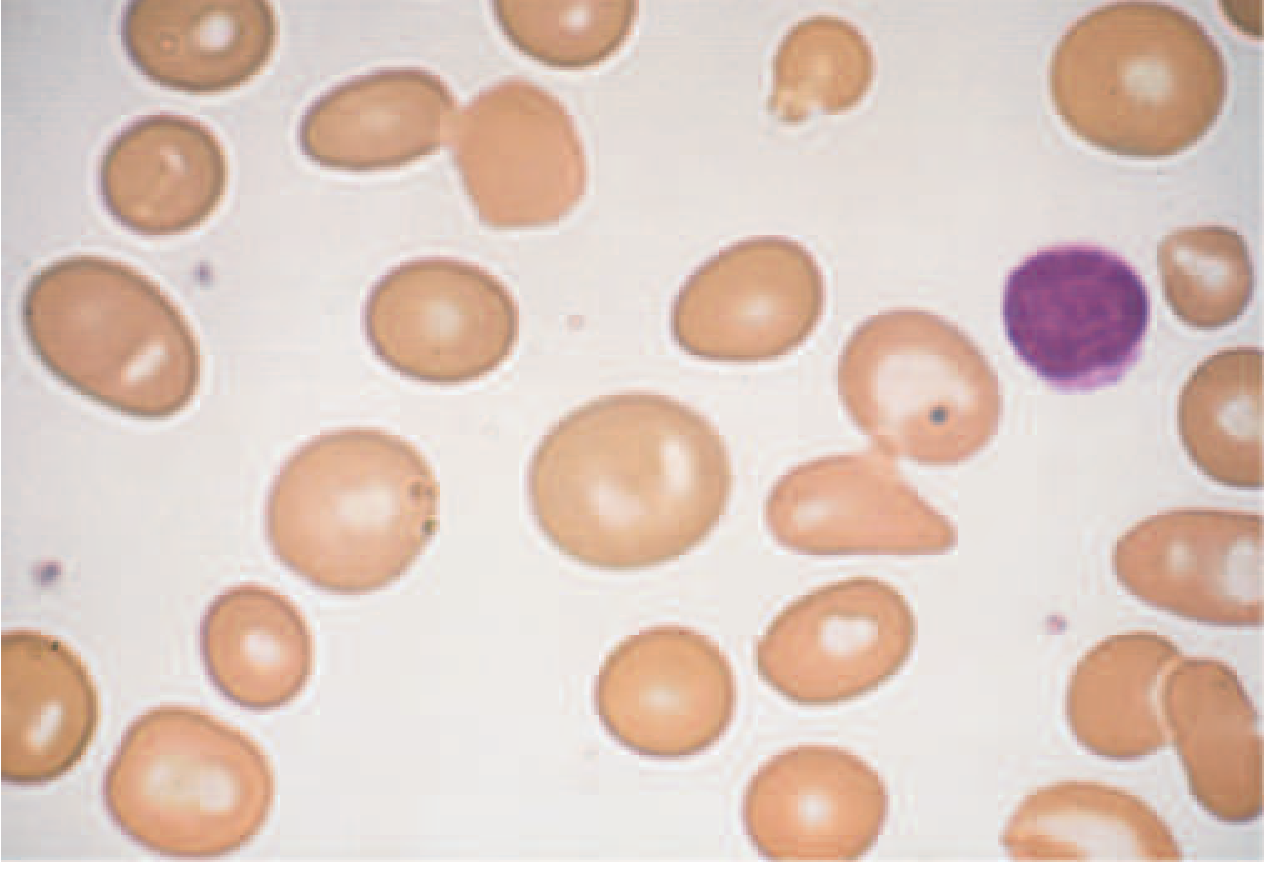
Macrocytosis — large oval-shaped (macro-ovalocyte) cells, well hemoglobinized, often with hypersegmented neutrophils in B12/folate deficiency:
Other important smear findings:
| Morphology | Associations |
|---|---|
| Schistocytes / helmet cells | Microangiopathic hemolytic anemia (TTP, HUS, DIC) |
| Spherocytes | Hereditary spherocytosis, autoimmune hemolytic anemia |
| Target cells | Thalassemia, liver disease, hemoglobin C |
| Teardrop cells | Myelofibrosis, severe iron deficiency |
| Sickle cells | Sickle cell disease |
| Bite cells | G6PD deficiency |
| Echinocytes (burr cells) | Uremia, liver disease |
| Howell-Jolly bodies | Asplenia, hyposplenism |
| Nucleated RBCs | Severe hemolysis, marrow infiltration |
| Polychromasia | Reticulocytosis (early marrow response) |
Reticulocyte Count
Measures bone marrow erythropoietic activity — essential for classifying anemia as:
- Hypoproliferative (low reticulocyte count) → bone marrow failure, nutritional deficiency, chronic disease
- Hyperproliferative (high reticulocyte count) → hemolysis or blood loss with intact marrow
The corrected reticulocyte count adjusts for the degree of anemia:
Corrected reticulocyte count = Measured reticulocyte % × (Patient Hct / 45)
The absolute reticulocyte count (from automated counters) requires no correction.
Additional Targeted Tests
| Suspected Cause | Tests |
|---|---|
| Iron deficiency | Serum iron ↓, TIBC ↑, ferritin ↓ |
| B12/folate deficiency | Serum B12, folate; methylmalonic acid; homocysteine |
| Hemolysis | LDH ↑, haptoglobin ↓, indirect bilirubin ↑, direct Coombs test |
| Renal disease | Creatinine, BUN |
| Hypothyroidism | TSH |
| Aplastic anemia / malignancy | Bone marrow biopsy |
| Hemoglobinopathy | Hemoglobin electrophoresis |
| Chronic disease | ESR, CRP, ferritin (elevated) |
Bone Marrow Examination
Indicated when peripheral blood and biochemical tests are inconclusive, or when marrow infiltration (malignancy, myelofibrosis) or aplastic anemia is suspected. Aspiration from the posterior iliac spine allows evaluation of:
- Cellularity (erythroid vs. myeloid hyperplasia)
- Cell morphology and differential
- Iron stores (Prussian blue stain)
Summary: Four Steps to Diagnosis (Harrison's)
- History — symptoms, bleeding sites, diet, drugs, family
- Physical exam — consequences of anemia (flow murmur, pallor, tachycardia) + etiologic clues (splenomegaly, glossitis, frontal bossing)
- Peripheral blood smear — red cell morphology, reticulocyte count
- Targeted lab tests — guided by MCV classification and smear findings
Sources: Harrison's Principles of Internal Medicine 22E (2025), Rosen's Emergency Medicine, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.