Hemoptysis answer from.archit ballloor
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
Archit Balloor hemoptysis medical textbook
Reading File
Reading File
Searching the Web
Archith Boloor hemoptysis causes classification management exam preparatory medicine
Reading Web Page
https://www.jaypeedigital.com/book/9789386056610/chapter/ch6
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive answer. Note that "Archit Balloor" is actually Dr. Archith Boloor, author of Exam Preparatory Manual for Undergraduates: Medicine - that specific book is not in the library, but I have the full content from Harrison's 22E, Fishman's Pulmonary Diseases, and Murray & Nadel, which are the standard references Archith Boloor himself cites. I'll now compile the full structured answer in Archith Boloor's exam-style format.
Note: The book you're referring to is likely Dr. Archith Boloor's Exam Preparatory Manual for Undergraduates: Medicine, which is not in this library. The answer below is compiled from Harrison's 22E, Fishman's Pulmonary Diseases & Disorders, and Murray & Nadel - the same standard references used in that manual - structured in the exam-Q&A format Boloor follows.
HEMOPTYSIS
Definition
Hemoptysis is the expectoration (coughing up) of blood or blood-stained sputum originating from the lower respiratory tract (anywhere from the glottis to the alveolus).
- Harrison's 22E, p. 318
Hemoptysis vs Hematemesis (Important Distinction)
| Feature | Hemoptysis | Hematemesis |
|---|---|---|
| Color | Bright red | Dark red/coffee-ground |
| pH | Alkaline | Acidic |
| Mixed with | Frothy sputum | Food particles |
| Microscopy | Hemosiderin-laden macrophages | Gastric contents |
| Associated symptoms | Cough, respiratory symptoms | Nausea, GI symptoms |
| History | Lung/cardiac disease | GI/liver disease |
Classification by Volume
| Type | Volume |
|---|---|
| Scant / Streak hemoptysis | Blood streaking of sputum |
| Mild / Non-massive | < 150 mL in 24 hours |
| Massive / Life-threatening | > 150-600 mL in 24 hours (definitions vary) OR any bleeding rate >/= 100 mL/h that threatens life |
Massive hemoptysis most commonly originates from the bronchial circulation (high-pressure, aortic origin), not the pulmonary circulation. This is why it can be difficult to control.
Causes of Hemoptysis
Airway Causes
- Bronchitis (viral - most common in developed countries, often streak hemoptysis)
- Bronchiectasis (including cystic fibrosis) - recurrent, can be massive; airways dilated, inflamed, highly vascular
- Bronchogenic carcinoma (squamous cell and small cell - central, erode major vessels)
- Carcinoid tumor (vascular, proximal airways)
- Foreign body aspiration
Parenchymal / Infectious Causes
- Pulmonary tuberculosis - most common worldwide (especially developing countries); cavitary disease, Rasmussen's aneurysm (erosion of pulmonary artery aneurysm into TB cavity)
- Lung abscess / Necrotizing pneumonia (S. aureus, Klebsiella, oral anaerobes)
- Pneumonia (Strep. pneumoniae, H. influenzae, Moraxella catarrhalis)
- Aspergilloma (fungus ball in pre-existing cavity, neovascularization - important cause of massive hemoptysis)
- Endemic fungi (Histoplasma, Coccidioides), Nocardia, NTM
- Paragonimiasis (mimics TB; Southeast Asia/China; raw crayfish ingestion)
Vascular Causes
- Mitral stenosis (raised pulmonary venous pressure)
- Pulmonary embolism with infarction
- Left heart failure (pink frothy sputum)
- Arteriovenous malformation (AVM)
- Aortobronchial fistula (aneurysm/pseudoaneurysm - small bleeds then massive)
- Dieulafoy's disease of the bronchus (rare - submucosal fistula between bronchial and pulmonary arteries)
Diffuse Alveolar Hemorrhage (DAH)
- Granulomatosis with polyangiitis (GPA, formerly Wegener's) - "pulmonary-renal syndrome" (hemoptysis + hematuria)
- Anti-GBM disease (Goodpasture syndrome)
- SLE-associated capillaritis
- Cocaine/inhalant toxicity
- Stem cell transplantation
- Vaping-induced lung injury
Miscellaneous
- Coagulopathy / thrombocytopenia / anticoagulants
- Catamenial hemoptysis (pulmonary endometriosis - cyclical bleeding with menstruation)
- Iatrogenic: post-lung biopsy, pulmonary artery catheter rupture, pulmonary vein stenosis post-ablation
- COPD (unexplained, usually non-recurrent)
- Bevacizumab / ramucirumab (anti-VEGF agents) in squamous cell lung cancer
Exam tip: In patients < 40 years - think infection; in patients > 40-45 years or smokers - think bronchogenic carcinoma.
Evaluation
History
- Pattern, severity, frequency, quantity
- Sputum description (streaks vs frank blood vs clots)
- Respiratory symptoms, weight loss, smoking, TB contact, travel history
- Anticoagulant use, menstrual cycle (catamenial)
Physical Examination
- Vital signs, O2 saturation
- Signs of chronic lung disease (clubbing, hyperinflation)
- Cardiovascular: mitral stenosis (opening snap, mid-diastolic murmur)
- ENT: to exclude nasal/oropharyngeal source
Investigations
- Chest X-ray - first-line; identifies cavities, masses, consolidation, hilar lymphadenopathy
- CBC - degree of anaemia, thrombocytopenia (contributing factor)
- Coagulation studies (PT/INR, aPTT)
- Sputum AFB smear + culture - rule out TB
- CT chest (HRCT / multidetector CT angiography) - identifies source of bleeding, underlying pathology, bronchial and non-bronchial systemic arteries with high sensitivity
- Bronchoscopy - direct visualization, localizes bleeding site, allows therapeutic intervention (rigid preferred in massive hemoptysis)
- Urinalysis / renal function - if pulmonary-renal syndrome suspected (GPA, Goodpasture)
- Echocardiography - if mitral stenosis suspected
Imaging Examples:
Management
Non-Massive Hemoptysis
- Identify and treat underlying cause
- Suppress cough (antitussives)
- Treat infection (antibiotics as appropriate)
- Correct coagulopathy if present
- Outpatient management often feasible; monitor closely
Massive / Life-Threatening Hemoptysis
Immediate priorities (ABC):
- Airway - maintain patency; intubate if needed (large-bore ETT, preferably 8.0 mm)
- Oxygenation - supplemental oxygen
- Hemodynamic stabilization - IV access, fluids, blood products
Positioning: Lateral decubitus with bleeding side DOWN - prevents aspiration into the unaffected lung.
Definitive interventions:
| Intervention | Details |
|---|---|
| Bronchial artery embolization (BAE) | First-line definitive procedure; controls bleeding in 75-90% of cases; rebleeding in 20-50% without surgery; re-embolization usually effective |
| Emergency bronchoscopy | Rigid bronchoscopy preferred; localizes site; allows laser (Nd:YAG), argon plasma coagulation, or electrocautery |
| CT angiography | In stable patients; delineates bronchial and non-bronchial arteries; identifies source and underlying pathology |
| Surgery | Salvage after failed embolization; better outcomes in elective/non-urgent setting; may include lobectomy/pneumonectomy |
Post-embolization syndrome: Pleuritic pain, fever, dysphagia, leukocytosis - lasts 5-7 days, resolves with symptomatic treatment.
Rare complications of BAE: Bronchial/esophageal necrosis, myocardial infarction, spinal cord infarction.
Special Situations
Aspergilloma: Correct thrombocytopenia; antifungals; surgical evaluation for cavitary lesions with aspergillosis.
Hematologic malignancy + hemoptysis: Often associated with Aspergillus - infiltrates may cavitate when granulocytopenia resolves, causing massive hemoptysis.
Anti-VEGF agents (bevacizumab, ramucirumab): Contraindicated or high risk in squamous cell NSCLC with cavitary lesions or prior hemoptysis >/= 2.5 mL within 3 months.
Pulmonary-renal syndrome: GPA or anti-GBM disease - treat with immunosuppression (cyclophosphamide + steroids for GPA; plasmapheresis + steroids for Goodpasture).
Rasmussen's Aneurysm (High-Yield)
- Erosion of a pulmonary artery aneurysm into a pre-existing TB cavity
- Rare but important cause of massive hemoptysis in TB
- Source: pulmonary circulation (not bronchial)
Sources
- Harrison's Principles of Internal Medicine, 22E (2025) - pp. 318-319, 635
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set - pp. 443-444
- Murray & Nadel's Textbook of Respiratory Medicine
Pleural effusion
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the complete Archith Boloor-style exam answer.
PLEURAL EFFUSION
Definition
Pleural effusion is the abnormal accumulation of excess fluid in the pleural space (normally only ~15 mL of clear, relatively acellular serous fluid is present for lubrication).
- Harrison's 22E, p. 2311; Robbins Pathology, p. 676
Physiology of Pleural Fluid Formation
Under normal conditions:
- Fluid enters the pleural space from capillaries in the parietal pleura
- Fluid is removed via lymphatics of the parietal pleura
- Fluid can also enter from: lung interstitial spaces (via visceral pleura) or peritoneal cavity (via small diaphragmatic holes)
- The lymphatics can absorb 20 times more fluid than is normally formed
A pleural effusion develops when the balance between formation and removal is disturbed.
Mechanisms of Accumulation (Pathophysiology)
| Mechanism | Example |
|---|---|
| Increased hydrostatic pressure | Congestive heart failure |
| Decreased oncotic pressure | Nephrotic syndrome, hypoalbuminemia |
| Increased capillary permeability | Pneumonia, inflammation |
| Decreased lymphatic drainage | Mediastinal carcinomatosis |
| Increased intrapleural negative pressure | Atelectasis |
| Fluid from peritoneal cavity | Cirrhosis (hepatic hydrothorax), Meigs' syndrome |
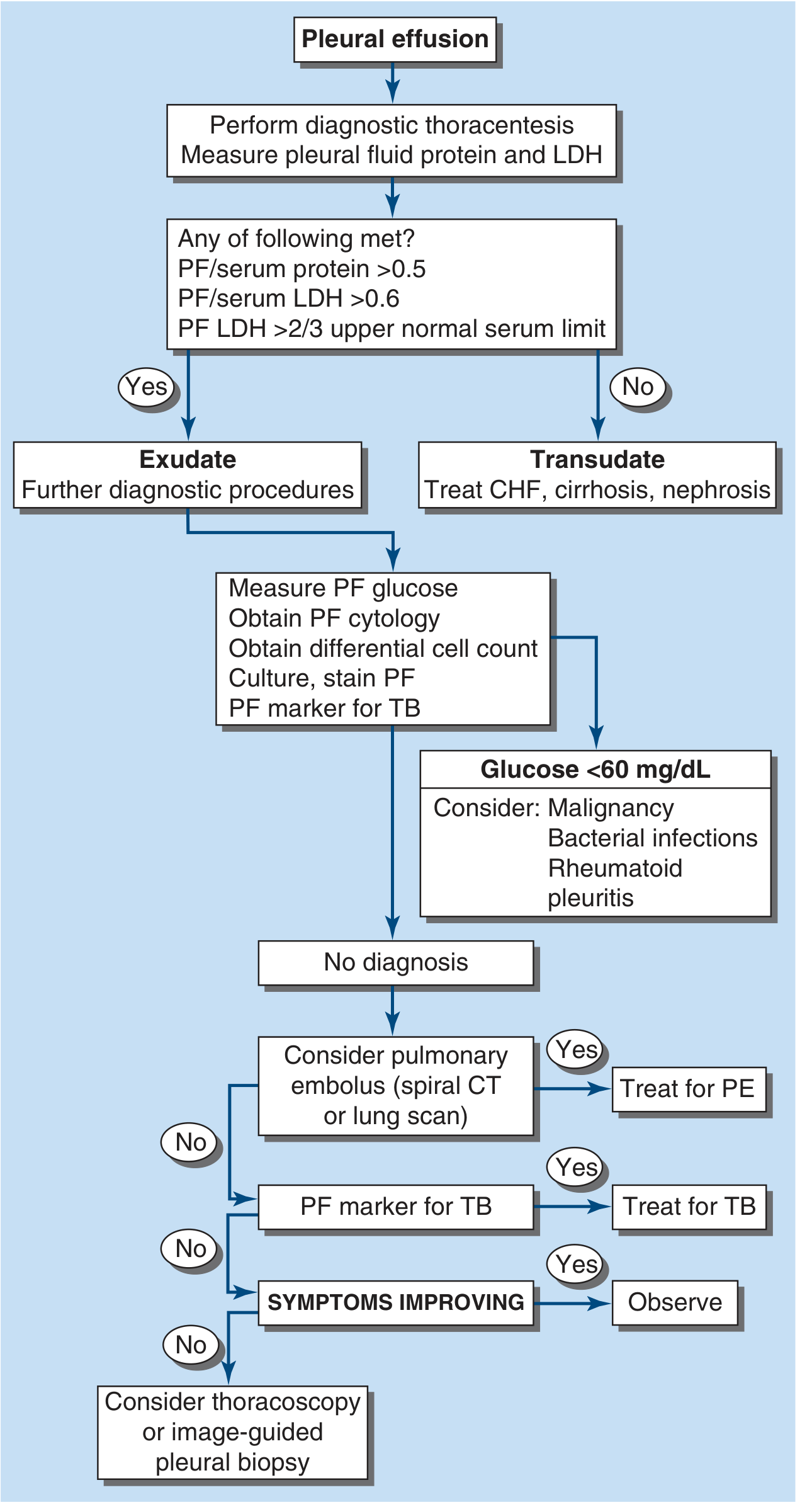
Classification: Transudate vs Exudate
Light's Criteria (Exudate - meets >/= 1):
| Criterion | Threshold for EXUDATE |
|---|---|
| Pleural fluid protein / Serum protein | > 0.5 |
| Pleural fluid LDH / Serum LDH | > 0.6 |
| Pleural fluid LDH | > 2/3 of upper normal serum LDH |
- Transudates meet none of the above criteria
- These criteria misidentify ~25% of transudates as exudates ("pseudoexudates") - often a diuresed transudate
- If pseudoexudate suspected: use Serum-Pleural fluid Protein Gradient (SPPG) > 3.1 g/dL or Serum-Pleural fluid Albumin Gradient (SPAG) > 1.2 g/dL - 100% sensitive for CHF, 99% for hepatic hydrothorax
Causes
TRANSUDATIVE Effusions
- Congestive heart failure (most common cause overall)
- Cirrhosis (hepatic hydrothorax)
- Nephrotic syndrome
- Peritoneal dialysis
- Superior vena cava obstruction
- Myxedema (hypothyroidism)
- Urinothorax
EXUDATIVE Effusions
1. Neoplastic diseases
- Metastatic disease - lung carcinoma, breast carcinoma, lymphoma (cause 75% of malignant effusions)
- Mesothelioma (asbestos-related)
2. Infectious diseases
- Bacterial infections / Parapneumonic effusion (most common exudative cause in US; up to 50% of community-acquired pneumonia)
- Tuberculosis (most common cause in developing countries)
- Fungal, viral, parasitic infections
3. Pulmonary embolism (can be exudate or transudate)
4. Gastrointestinal disease
- Esophageal perforation (amylase-rich, left-sided)
- Pancreatic disease (amylase-rich)
- Intraabdominal abscesses
- Diaphragmatic hernia
- Post-abdominal surgery, endoscopic variceal sclerotherapy, post-liver transplant
5. Collagen vascular diseases
- Rheumatoid pleuritis (very low glucose, low pH)
- SLE, drug-induced lupus
- Sjogren syndrome
- Granulomatosis with polyangiitis (Wegener's)
- Churg-Strauss syndrome
6. Other exudates
- Post-coronary artery bypass surgery (left-sided, bloody early then serous)
- Asbestos exposure
- Sarcoidosis
- Uremia
- Meigs' syndrome (ovarian fibroma + right-sided pleural effusion + ascites - resolves with tumor removal)
- Yellow nail syndrome
- Drug-induced (nitrofurantoin, dantrolene, methysergide, bromocriptine, amiodarone, dasatinib)
- Trapped lung
- Radiation therapy
- Post-cardiac injury syndrome (Dressler's)
- Hemothorax
- Iatrogenic injury
- Ovarian hyperstimulation syndrome
- Chylothorax (triglycerides > 110 mg/dL - disruption of thoracic duct)
Diagnostic Algorithm
Clinical Features
Symptoms:
- Dyspnea (most common, often out of proportion to effusion size in malignancy)
- Pleuritic chest pain (dull, heavy, worse with breathing - from pleural inflammation)
- Dry cough
Signs:
- Tracheal/mediastinal shift away from large effusion
- Stony dull percussion note (dullest of all percussion notes)
- Reduced / absent breath sounds
- Reduced tactile vocal fremitus
- Reduced chest expansion on affected side
- Aegophony (e-to-a change) at upper border of effusion
- Friction rub (if inflammatory, before fluid accumulates)
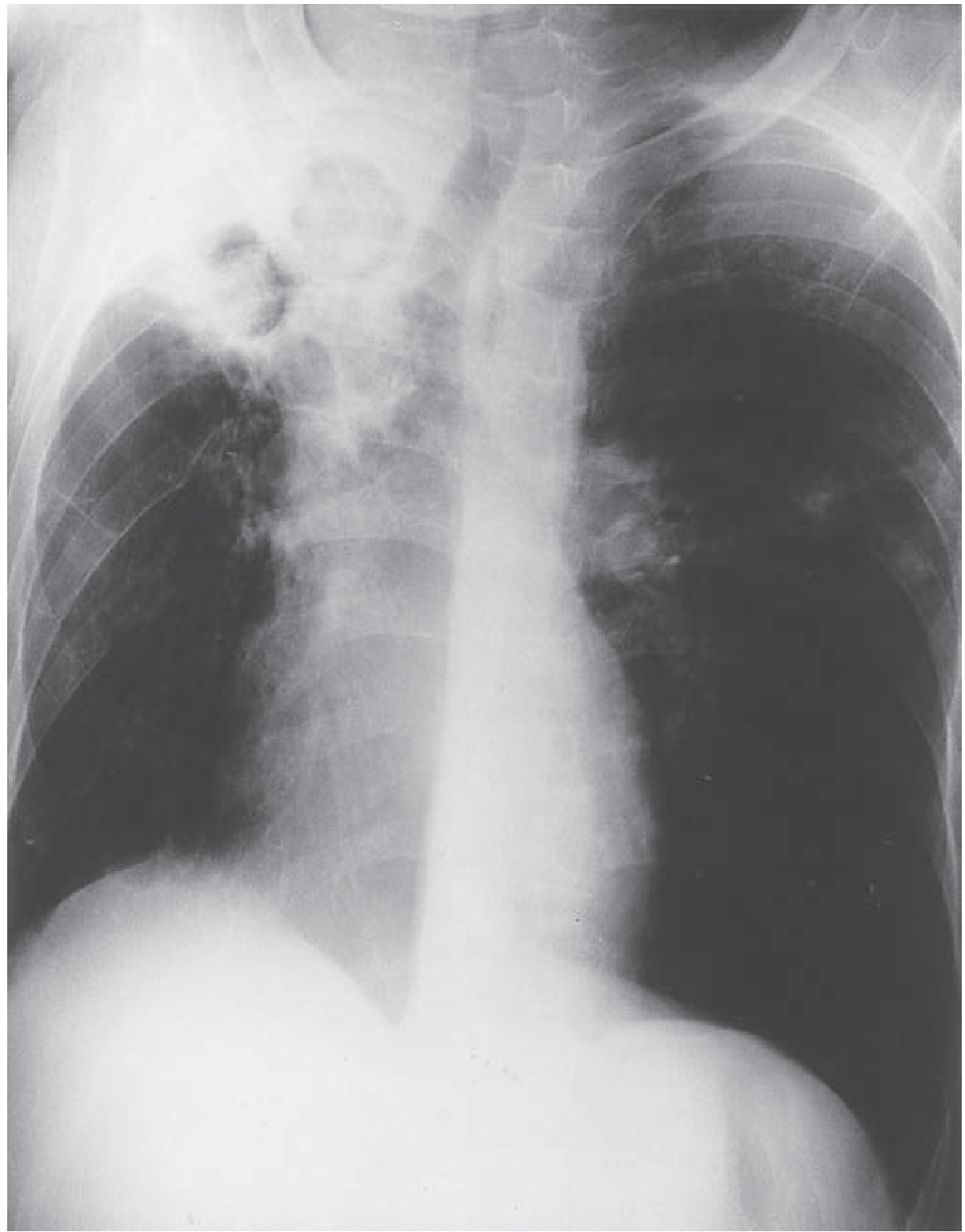
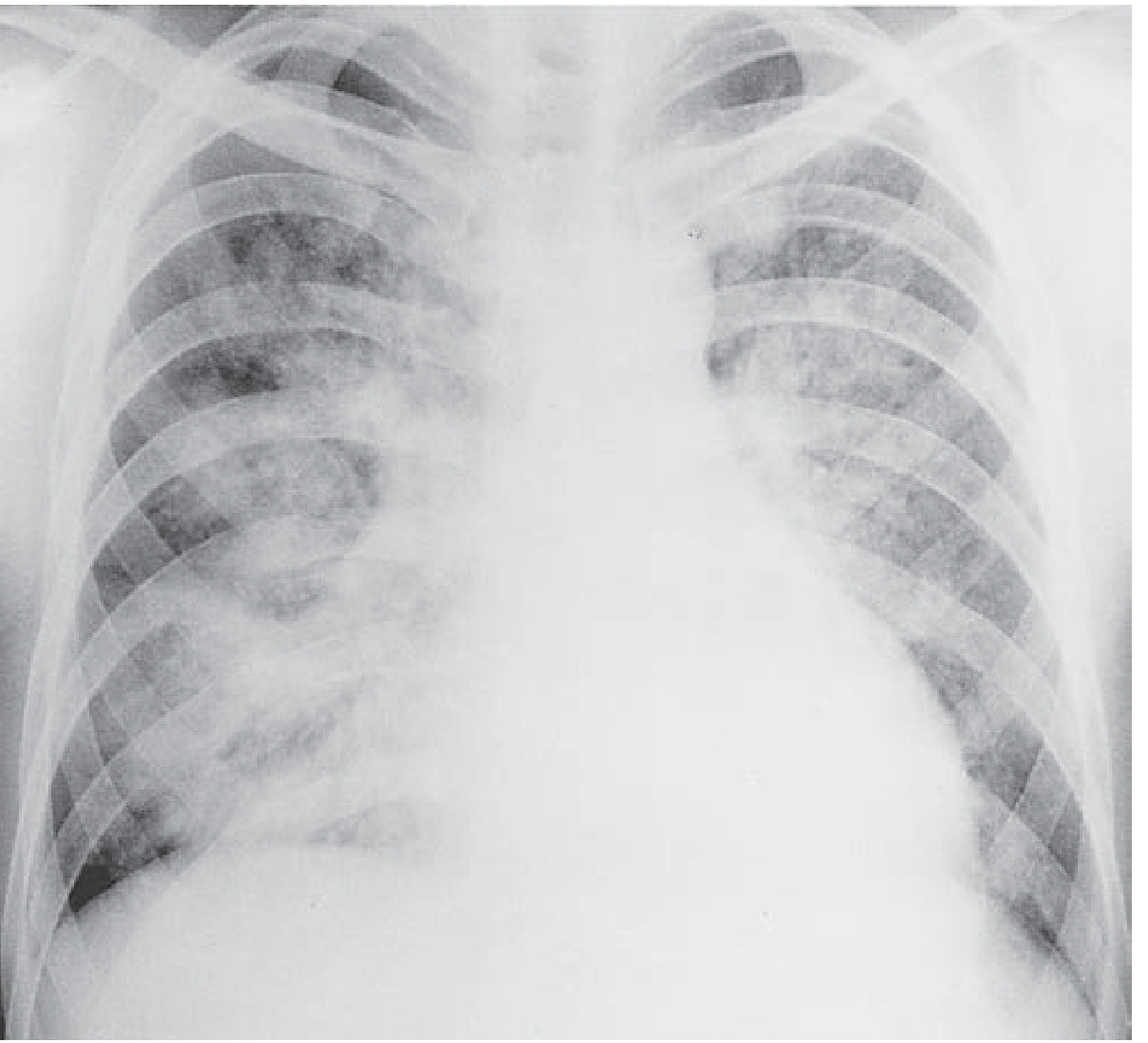
Radiology
Chest X-ray findings (PA erect):
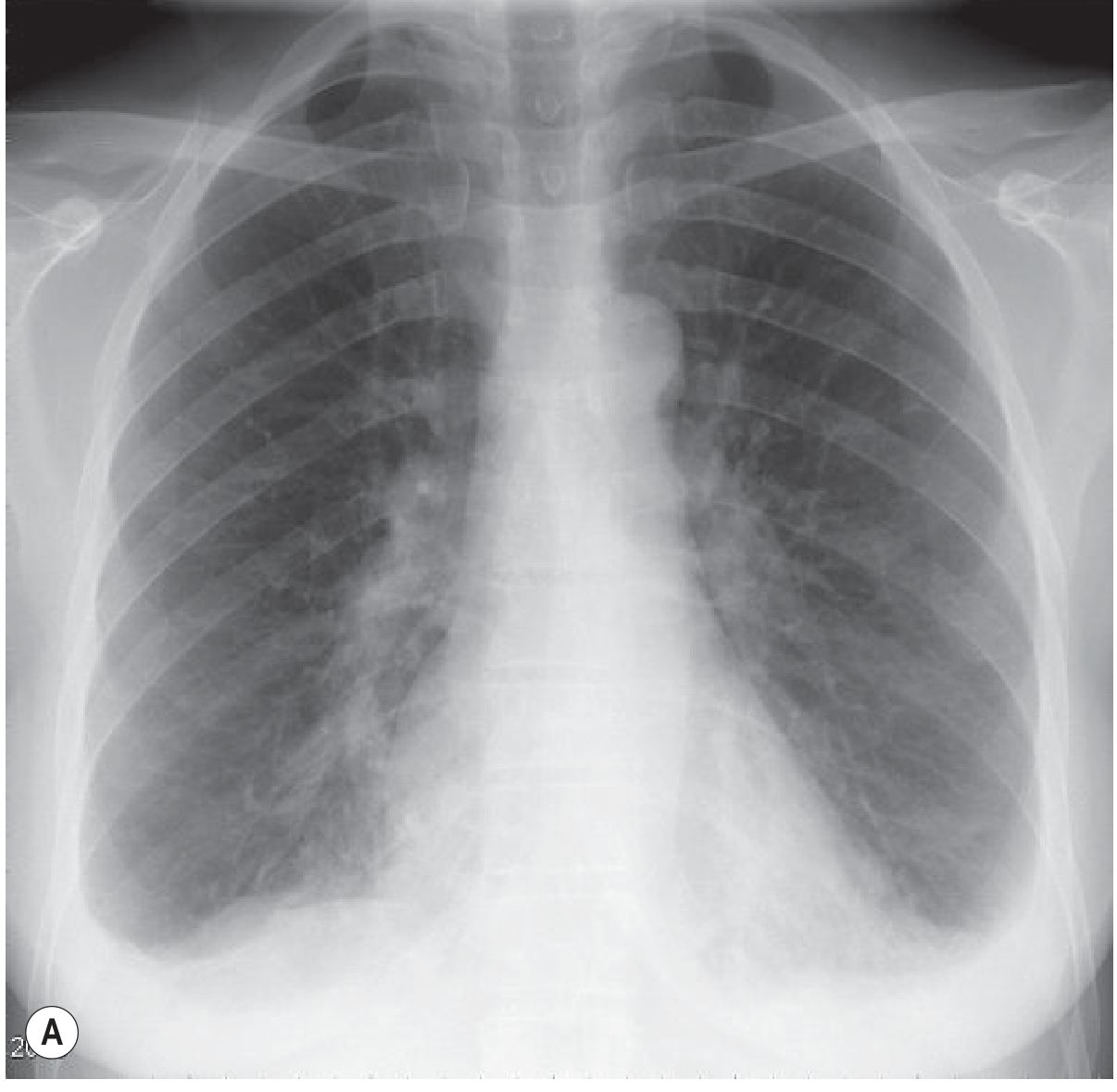
| Amount of effusion | CXR appearance |
|---|---|
| ~200 mL | Blunting of costophrenic angle on PA |
| ~500 mL | Visible opacity on PA |
| Large | Meniscus sign, shift of mediastinum away |
- Meniscus sign - fluid has concave upper margin, higher laterally than medially
- Subpulmonary effusion - appears as "high hemidiaphragm" with peak more laterally than usual
- Lateral decubitus film - detects even small effusions (as little as 50 mL)
- Supine (ICU) film - hazy opacity of lower thorax; costophrenic angles NOT obscured; vascular markings preserved through opacity
CT chest: Gold standard for characterizing effusion, identifying loculations, pleural thickening, underlying cause.
Ultrasound: Preferred to guide thoracentesis; distinguishes free from loculated fluid; detects septations.
Thoracentesis and Pleural Fluid Analysis
Indications for diagnostic thoracentesis:
- New or undiagnosed effusion
- CHF effusion that is unilateral, unequal in size, febrile patient, or pleuritic chest pain
Pleural fluid tests - routine:
- Protein, LDH (for Light's criteria)
- Glucose, cell count and differential
- Gram stain and culture
- Cytology
Disease-specific tests:
| Suspected Condition | Test |
|---|---|
| Parapneumonic / Empyema | pH (< 7.2 = complicated), glucose (< 60 mg/dL) |
| TB | Adenosine deaminase (ADA), culture, AFB |
| Malignancy | Cytology, flow cytometry (lymphoma) |
| Pancreatic disease / esophageal rupture | Amylase (elevated) |
| CHF | NT-proBNP > 1500 pg/mL |
| Chylothorax | Triglycerides (> 110 mg/dL), cholesterol |
| Hemothorax | Pleural fluid hematocrit (> 50% of blood hematocrit) |
| Rheumatoid / bacterial | Glucose (very low) + pH |
| Amyloidosis | Congo red staining |
| Drug-induced | Eosinophilia |
Specific Effusions - High Yield Points
Parapneumonic Effusion and Empyema
- PPE in up to 50% of community-acquired pneumonia
- Complicated PPE / Empyema requires drainage if ANY of:
- Loculated pleural fluid
- pH < 7.20
- Glucose < 3.3 mmol/L (< 60 mg/dL)
- Positive Gram stain or culture
- Gross pus in pleural space
- Pleural fluid LDH > 900 IU/L
- Treatment: chest tube + intrapleural tPA (10 mg) + DNase (5 mg) if loculated; thoracoscopy; surgical decortication if above fail
Malignant Pleural Effusion
- Three tumors cause 75%: lung, breast, lymphoma
- Poor prognosis (< 6-month survival)
- Dyspnea often out of proportion to effusion size
- Usually exudate; rarely transudate
- Low glucose if high tumor burden
- Diagnosis by cytology (positive in ~60%) or pleural biopsy
- Treatment: therapeutic thoracentesis, indwelling pleural catheter (IPC), pleurodesis (talc most effective)
Tuberculous Effusion
- Exudate with high ADA, lymphocyte-predominant
- Low glucose, low pH
- Culture positivity low (~25%); pleural biopsy more sensitive
- Treatment: standard anti-TB drugs; steroids may reduce residual pleural thickening
Hepatic Hydrothorax
- Complicates ~5-10% of cirrhosis patients
- Ascitic fluid passes through small diaphragmatic defects
- Usually right-sided (85%), transudative
- May occur without detectable ascites
- Treatment: sodium restriction + diuretics; TIPS (70-80% response); VATS repair of diaphragmatic defects + pleurodesis; liver transplantation
Chylothorax
- Triglycerides > 110 mg/dL (or chylomicrons on lipoprotein electrophoresis)
- Milky white fluid; lymphocyte-predominant
- Causes: thoracic duct trauma/surgery, lymphoma (most common malignant cause), lymphangioleiomyomatosis
- Treatment: low-fat diet (medium-chain triglycerides), octreotide, thoracic duct ligation
Meigs' Syndrome
- Ovarian fibroma (or other pelvic tumor) + ascites + pleural effusion (usually right-sided)
- Effusion is transudate
- All resolves with removal of the tumor
Rheumatoid Pleuritis
- Characteristically: very low glucose (< 30 mg/dL), very low pH - lower than any other non-infectious cause
- Cholesterol crystals may be seen in chronic effusions
Management Principles
Transudative Effusion
- Treat the underlying cause (heart failure, cirrhosis, nephrotic syndrome)
- Thoracentesis for symptom relief if large
- Do NOT insert a chest tube for a transudative effusion
Exudative Effusion
- Identify and treat specific cause
- Drainage if complicated PPE/empyema criteria met
- Malignant: IPC or pleurodesis for palliation
Pleurodesis
- Goal: obliterate pleural space to prevent recurrence
- Agents: Talc (most effective), bleomycin, doxycycline, tetracycline
- Method: chemical pleurodesis via chest tube or thoracoscopy (VATS)
- Requires lung re-expansion (will not work in trapped lung)
Indwelling Pleural Catheter (IPC)
- For recurrent malignant effusion or hepatic hydrothorax as bridge to transplant
- Outpatient drainage; can lead to auto-pleurodesis in ~40% of malignant cases
Sources
- Harrison's Principles of Internal Medicine, 22E (2025) - pp. 2311-2313
- Robbins, Cotran & Kumar Pathologic Basis of Disease - p. 676
- Murray & Nadel's Textbook of Respiratory Medicine
- Grainger & Allison's Diagnostic Radiology - p. 62
Pleural effusion
The full answer was just provided above. Here it is again in clean format for your reference:
PLEURAL EFFUSION
(Archith Boloor exam-style format, sourced from Harrison's 22E, Robbins, Murray & Nadel)
Definition
Pleural effusion is the abnormal accumulation of excess fluid in the pleural space. Normally only ~15 mL of clear, relatively acellular serous fluid is present for lubrication.
Physiology of Normal Pleural Fluid
- Fluid enters from capillaries of the parietal pleura
- Fluid is removed by lymphatics of the parietal pleura
- Can also enter from lung interstitium (via visceral pleura) or peritoneum (via diaphragmatic holes)
- Lymphatics can absorb 20x more fluid than is normally formed
Mechanisms of Accumulation
| Mechanism | Example |
|---|---|
| Increased hydrostatic pressure | Congestive heart failure |
| Decreased oncotic pressure | Nephrotic syndrome, hypoalbuminemia |
| Increased capillary permeability | Pneumonia, inflammation |
| Decreased lymphatic drainage | Mediastinal carcinomatosis |
| Increased intrapleural negative pressure | Atelectasis |
| Fluid from peritoneal cavity | Cirrhosis (hepatic hydrothorax), Meigs' syndrome |
Classification: Transudate vs Exudate
Light's Criteria - Exudate meets at least ONE:
| Criterion | Exudate threshold |
|---|---|
| PF protein / Serum protein | > 0.5 |
| PF LDH / Serum LDH | > 0.6 |
| PF LDH | > 2/3 of upper normal serum LDH |
- Transudates meet none
- ~25% of transudates misidentified as exudates ("pseudoexudates") - often a diuresed transudate
- If pseudoexudate suspected: SPPG > 3.1 g/dL or SPAG > 1.2 g/dL corrects this (100% sensitive for CHF, 99% for hepatic hydrothorax)
Causes
TRANSUDATES (systemic factors altered)
- Congestive heart failure - most common cause of pleural effusion overall
- Cirrhosis / Hepatic hydrothorax
- Nephrotic syndrome
- Peritoneal dialysis
- Superior vena cava obstruction
- Myxedema (hypothyroidism)
- Urinothorax
EXUDATES (local factors altered)
Neoplastic
- Metastatic disease - lung, breast, lymphoma (cause 75% of malignant pleural effusions)
- Mesothelioma
Infectious
- Parapneumonic effusion - most common exudative cause in US (up to 50% of community-acquired pneumonia)
- Tuberculosis - most common cause in developing countries
- Fungal, viral, parasitic infections
Vascular
- Pulmonary embolism (exudate or transudate)
Gastrointestinal
- Esophageal perforation (amylase-rich, left-sided)
- Pancreatic disease (amylase-rich, left-sided)
- Intraabdominal abscesses, diaphragmatic hernia
- Post-abdominal surgery, post-liver transplant, endoscopic variceal sclerotherapy
Collagen Vascular Diseases
- Rheumatoid pleuritis (characteristically very low glucose < 30 mg/dL, very low pH)
- SLE, drug-induced lupus
- Sjogren syndrome, GPA (Wegener's), Churg-Strauss
Miscellaneous
- Post-CABG (left-sided, bloody then serous)
- Asbestos exposure
- Sarcoidosis
- Uremia
- Meigs' syndrome (ovarian fibroma + ascites + right-sided effusion - transudate; resolves with tumor removal)
- Yellow nail syndrome
- Drug-induced: nitrofurantoin, dantrolene, methysergide, bromocriptine, amiodarone, dasatinib
- Trapped lung
- Radiation therapy
- Post-cardiac injury syndrome (Dressler's)
- Hemothorax
- Ovarian hyperstimulation syndrome
- Chylothorax (triglycerides > 110 mg/dL)
- Iatrogenic
Clinical Features
Symptoms:
- Dyspnea (most common; often out of proportion to size in malignancy)
- Pleuritic chest pain (dull, heavy, worse on breathing)
- Dry cough
Signs:
- Tracheal/mediastinal shift away from large effusion
- Reduced chest expansion on affected side
- Stony dull percussion (dullest of all - differentiates from consolidation which is dull)
- Reduced / absent breath sounds
- Reduced tactile vocal fremitus (TVF)
- Aegophony at upper border of effusion
- Pleural friction rub (early, before fluid accumulates)
Radiology
Chest X-ray (PA erect)
| Volume of fluid | CXR finding |
|---|---|
| ~50 mL | Detectable only on lateral decubitus |
| ~200 mL | Blunting of costophrenic angle |
| ~500 mL | Visible opacity PA view |
| Large | Meniscus sign + mediastinal shift away |
- Meniscus sign - concave upper border, higher laterally than medially
- Subpulmonary effusion - appears as "high hemidiaphragm" peaking more laterally; stomach bubble separated > 2 cm from lung (left-sided)
- Supine film (ICU) - hazy opacity of lower thorax; costophrenic angles NOT obscured; vascular markings visible through opacity (opposite to erect)
- Loculated effusion - lens-shaped, does not shift with position; "pseudotumour/vanishing tumour" in fissures
CT chest: Gold standard for loculation, pleural thickening, underlying pathology.
Ultrasound: Preferred for guiding thoracentesis; distinguishes free from loculated; detects septations.
Diagnostic Algorithm
Thoracentesis and Pleural Fluid Analysis
Routine tests:
- Protein + LDH (Light's criteria)
- Glucose, cell count + differential
- Gram stain + culture
- Cytology
Disease-specific tests:
| Suspected Condition | Test |
|---|---|
| Empyema / Complicated PPE | pH < 7.2, glucose < 60 mg/dL |
| TB | ADA (adenosine deaminase), AFB culture |
| Malignancy | Cytology (positive ~60%), flow cytometry (lymphoma) |
| Pancreatic disease / esophageal rupture | Amylase (elevated) |
| CHF | NT-proBNP > 1500 pg/mL |
| Chylothorax | Triglycerides > 110 mg/dL |
| Hemothorax | PF hematocrit > 50% of blood hematocrit |
| Rheumatoid pleuritis | Very low glucose + very low pH |
| Drug-induced | Eosinophilia |
| Amyloidosis | Congo red staining |
Specific Effusions - High Yield Points
Parapneumonic Effusion / Empyema
Exudate drainage is indicated if any of the following (complicated PPE/empyema criteria):
- Loculated pleural fluid
- pH < 7.20
- Glucose < 60 mg/dL (< 3.3 mmol/L)
- Positive Gram stain or culture
- Gross pus in pleural space
- LDH > 900 IU/L
Stages: Exudative → Fibrinopurulent → Organizing (pleural peel)
Treatment:
- Chest tube drainage
- Intrapleural tPA 10 mg + DNase 5 mg if loculated
- Thoracoscopy (VATS) with breakdown of adhesions
- Surgical decortication if above fail
Malignant Pleural Effusion
- Lung + breast + lymphoma = 75% of all malignant effusions
- Poor prognosis (< 6-month median survival)
- Dyspnea out of proportion to size
- Low glucose if high tumor burden
- Treatment: therapeutic thoracentesis → indwelling pleural catheter (IPC) or pleurodesis (talc most effective)
Tuberculous Pleural Effusion
- Exudate; lymphocyte-predominant
- High ADA (> 40-45 U/L)
- Low glucose, low pH
- AFB culture positivity low (~25%); pleural biopsy + culture more sensitive
- Treatment: standard 4-drug anti-TB therapy; steroids reduce residual thickening
Hepatic Hydrothorax
- 5-10% of cirrhosis patients
- Ascitic fluid through diaphragmatic defects
- Usually right-sided (85%), transudate
- May occur without detectable ascites
- Treatment: Na restriction + diuretics → TIPS (70-80% response) → VATS pleurodesis → liver transplant
Chylothorax
- Milky white fluid; lymphocyte-predominant; triglycerides > 110 mg/dL
- Causes: thoracic duct trauma/surgery, lymphoma (most common malignant cause), LAM
- Treatment: low-fat diet (MCT oil), octreotide, thoracic duct ligation/embolization
Meigs' Syndrome
- Triad: Ovarian fibroma + ascites + right-sided pleural effusion
- Effusion is a transudate
- Resolves completely after tumor removal
- Must distinguish from Pseudo-Meigs' (other pelvic tumors)
Rheumatoid Pleuritis
- Characteristically: glucose < 30 mg/dL (lowest of all non-infective causes)
- Very low pH, high LDH
- Complement levels very low
Management Summary
Transudative Effusion
- Treat underlying cause (CHF → diuretics/ACEi; cirrhosis → Na restriction, diuretics, TIPS; nephrotic → steroids + treat cause)
- Therapeutic thoracentesis for symptomatic relief
- Do NOT insert chest tube for a simple transudate
Exudative Effusion
- Identify and treat underlying cause
- Drain if complicated PPE/empyema criteria met
- Malignant: IPC or chemical pleurodesis
Pleurodesis
- Talc - most effective agent
- Others: bleomycin, doxycycline, tetracycline
- Method: via chest tube (slurry) or thoracoscopy (poudrage)
- Will NOT work if lung is trapped (cannot re-expand)
- Trapped lung diagnosis: pleural manometry, pneumothorax ex vacuo on imaging post-thoracentesis, rapid recurrence
Sources
- Harrison's Principles of Internal Medicine, 22E (2025) - pp. 2311-2313
- Robbins, Cotran & Kumar Pathologic Basis of Disease - p. 676
- Murray & Nadel's Textbook of Respiratory Medicine
- Grainger & Allison's Diagnostic Radiology - p. 62
Bronchial asthma
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full Archith Boloor-style answer.
BRONCHIAL ASTHMA
(Exam-style format - Harrison's 22E, Murray & Nadel, Fishman's)
Definition
Bronchial asthma is a chronic inflammatory disorder of the airways characterized by:
- Airway hyperresponsiveness to a variety of stimuli
- Reversible airway obstruction (spontaneously or with treatment)
- Airway inflammation (predominantly eosinophilic)
- Airway remodeling in chronic disease
The hallmark is episodic, reversible bronchoconstriction producing wheezing, breathlessness, chest tightness, and cough - typically worse at night or early morning.
Epidemiology
- Affects ~300 million people worldwide
- More common in boys < girls in childhood; reverses by age 40 (women > men in adults)
- Occupational asthma accounts for 10-25% of adult-onset asthma
Etiology / Risk Factors
Intrinsic (Endogenous) Factors
- Atopy (genetic predisposition to IgE-mediated sensitization) - strongest risk factor
- Genetic factors (multiple susceptibility genes including those on chromosomes 5, 6, 11, 12)
- Sex and hormonal factors (perimenstrual, perimenopause, pregnancy)
- Obesity
- Prematurity, caesarean delivery, neonatal jaundice
Extrinsic (Environmental) Factors
- Allergen exposure (house dust mite, pollen, animal dander, mold, cockroach)
- Occupational exposures (flour, diisocyanates, formaldehyde - nursing and cleaning most common)
- Air pollution, tobacco (active and passive)
- Respiratory infections (rhinovirus, RSV, Mycoplasma pneumoniae)
- Diet (vitamin D deficiency, maternal polyunsaturated fatty acids)
Triggers of Acute Attacks
- Allergens (inhaled)
- Irritants (smoke, dust, fumes, strong smells)
- Viral respiratory infections (most common trigger in children)
- Exercise and cold, dry air
- Air pollution
- Drugs: Aspirin / NSAIDs (aspirin-exacerbated respiratory disease - AERD), beta-blockers (most dangerous), ACE inhibitors (cough)
- Occupational exposures
- Hormonal changes / pregnancy
- Emotional stress
- GERD (independent predictor of exacerbations)
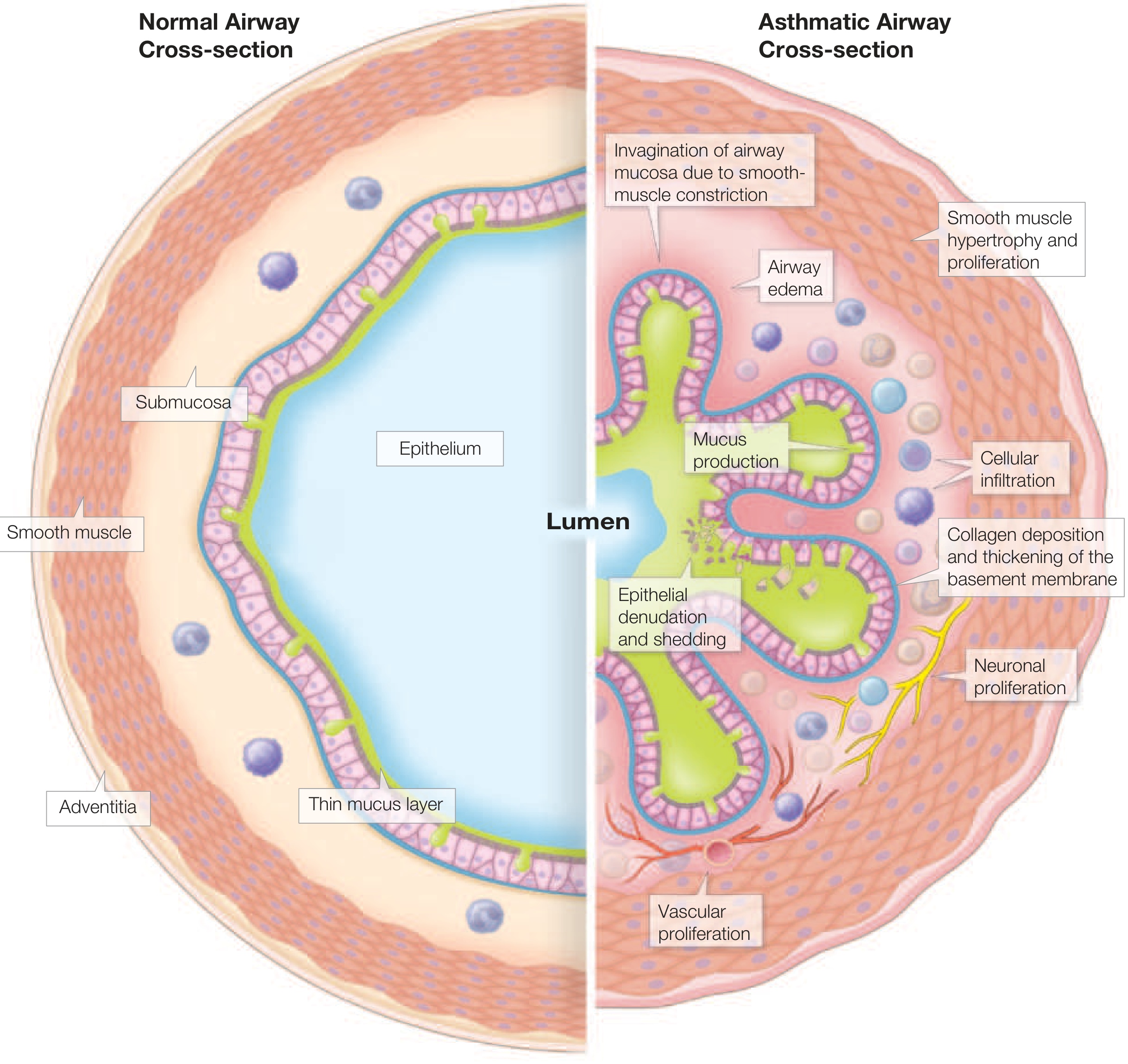
Pathophysiology
Three Core Mechanisms
1. Airway Hyperresponsiveness (AHR)
- Hallmark of asthma
- Exaggerated narrowing response to stimuli harmless to normal individuals
- Due to: smooth muscle hyperresponsiveness (direct) + inflammatory cell mediator release (indirect) + structural changes (airway wall thickening)
2. Airway Inflammation
- Usually eosinophilic (Type 2 inflammation) - most common
- Neutrophilic in severe asthma and occupational asthma
- Mixed eosinophilic + neutrophilic = most severe phenotype
- Key cells: mast cells (early phase), eosinophils, T helper 2 (Th2) cells, basophils
3. Airway Remodeling (chronic)
- Smooth muscle hypertrophy and hyperplasia
- Subepithelial collagen deposition and basement membrane thickening
- Goblet cell hyperplasia, mucus hypersecretion
- Epithelial denudation and shedding
- Vascular proliferation
- Neuronal proliferation
Biphasic Response (Early and Late)
| Phase | Timing | Mediators | Features |
|---|---|---|---|
| Early (immediate) phase | Within 10-20 min | Histamine, LTC4/D4/E4, prostaglandins, bradykinin (from mast cells) | Bronchoconstriction, resolves in 1-2 hrs |
| Late phase | 4-8 hrs later | IL-4, IL-5, IL-13 (from Th2 cells, eosinophils) | Sustained inflammation, mucosal edema, mucus production |
Key Mediators in Asthma
- Histamine - bronchoconstriction, mucus secretion
- Leukotrienes (LTC4, LTD4, LTE4) - potent bronchoconstriction, mucus secretion, edema (1000x more potent than histamine)
- IL-4, IL-13 - IgE production, goblet cell metaplasia
- IL-5 - eosinophil differentiation and survival
- IL-33, TSLP - alarmins from epithelium initiating type 2 inflammation
- PAF (platelet activating factor) - bronchoconstriction, eosinophil recruitment
Classification
GINA Classification by Symptom Frequency (before treatment)
| Step | Frequency of Symptoms | Night Symptoms | FEV1/PEFR |
|---|---|---|---|
| Step 1 - Intermittent | < 2 days/week | ≤ 2 nights/month | ≥ 80% predicted |
| Step 2 - Mild Persistent | > 2 days/week but not daily | 3-4 nights/month | ≥ 80% |
| Step 3 - Moderate Persistent | Daily | > 1 night/week | 60-80% |
| Step 4 - Severe Persistent | Continuous | Frequent (7 nights/week) | < 60% |
Classification of Asthma by Type/Endotype
| Type | Features |
|---|---|
| Allergic/Atopic asthma | Childhood onset, IgE-mediated, elevated eosinophils, responds well to ICS |
| Non-allergic asthma | Adult onset, infection/irritant-triggered, neutrophilic, less ICS-responsive |
| Late-onset eosinophilic asthma | Adult women, severe, nasal polyps, aspirin-sensitive (AERD) |
| Occupational asthma | Workplace sensitizers; RADS (reactive airway dysfunction syndrome) = irritant form |
| Exercise-induced asthma | Bronchoconstriction during/after exercise, cold-dry air |
| Aspirin-exacerbated (AERD) | Aspirin + NSAIDs trigger attacks; nasal polyps; Samter's triad |
Clinical Features
Symptoms (Classic Triad)
- Wheeze (high-pitched, expiratory > inspiratory)
- Breathlessness (dyspnea)
- Cough (dry, non-productive; nocturnal cough is classic)
- Chest tightness
- Typically worse at night and early morning
- Episodic with symptom-free intervals
Signs in Acute Attack
- Tachypnea, tachycardia
- Hyperinflated chest (barrel chest in chronic)
- Prolonged expiration with expiratory wheeze
- Use of accessory muscles (sternocleidomastoid, scalenes)
- Intercostal / subcostal retractions
- Pulsus paradoxus > 10 mmHg (indicates severe attack)
- Hyperresonant percussion
- Reduced air entry bilaterally
Signs of Severe / Life-Threatening Attack
- Silent chest (no wheeze = no airflow = ominous)
- Cyanosis
- Inability to complete sentences
- SpO2 < 92%
- Bradycardia / hypotension
- Confusion / exhaustion
- PaCO2 rising (normal or elevated CO2 in asthma = impending respiratory failure)
Investigations
Spirometry (Most Important)
- Obstructive pattern: FEV1 reduced, FVC reduced/normal, FEV1/FVC ratio < 0.70
- Reversibility: >/= 12% AND >/= 200 mL increase in FEV1 after SABA - confirms asthma
- Bronchial provocation test (methacholine/histamine challenge): if spirometry normal; PC20 < 8 mg/mL = positive (hyperresponsiveness)
Peak Expiratory Flow Rate (PEFR)
- Reduced during attacks
- Diurnal variation > 20% (morning dip) is characteristic of asthma
- Used for monitoring and guiding therapy (personal best PEFR)
ABG (in acute severe attack)
- Mild/Moderate: Respiratory alkalosis (hyperventilation - low PaCO2, high pH)
- Normal or rising PaCO2 = danger sign = impending respiratory failure
- Hypoxemia (low PaO2)
Other Investigations
- Chest X-ray: Hyperinflation (during attack); may show mucus plugging; rule out pneumothorax or pneumonia; usually normal between attacks
- CBC: Eosinophilia (blood eosinophils ≥ 150-300 cells/μL suggests type 2 asthma)
- Total serum IgE + specific IgE / skin prick test - for allergen identification
- Exhaled Nitric Oxide (FeNO): > 25 ppb suggests eosinophilic airway inflammation; predicts ICS response
- Sputum analysis: Eosinophils, Charcot-Leyden crystals, Curschmann's spirals, Creola bodies (shed epithelial clusters)
Classic Sputum Findings in Asthma
| Finding | Description |
|---|---|
| Charcot-Leyden crystals | Bipyramidal crystals from eosinophil granules |
| Curschmann's spirals | Mucus casts of small airways |
| Creola bodies | Clusters of shed bronchial epithelial cells |
Management
Goals of Therapy (GINA / NAEPP)
- Symptoms ≤ 2 times/week
- Night awakenings ≤ 2 times/month
- Reliever use ≤ 2 times/week (except pre-exercise)
- No more than 1 exacerbation/year
- Optimize lung function
- Maintain normal daily activities
- Minimal or no side effects
Step-Up / Step-Down Approach
| Step | Preferred Treatment | Alternative |
|---|---|---|
| Step 1 (Intermittent) | As-needed ICS/formoterol (anti-inflammatory reliever - AIR) | As-needed ICS + SABA |
| Step 2 (Mild persistent) | Low-dose ICS daily + as-needed SABA or AIR | LTRA (montelukast) |
| Step 3 (Moderate persistent) | Low-dose ICS + LABA | Medium-dose ICS; + LTRA |
| Step 4 (Severe) | Medium-to-high dose ICS + LABA | + LAMA (tiotropium), + LTRA |
| Step 5 (Very severe) | High-dose ICS + LABA + Biologic (anti-IL-5, anti-IgE, anti-IL-4Rα) | + Low-dose oral corticosteroids |
Key change (GINA): ICS/formoterol as-needed is now preferred at ALL steps including step 1. SABA monotherapy is no longer recommended as reliever due to increased asthma mortality.
Drug Classes
Relievers (Bronchodilators)
| Drug | Class | Onset | Duration | Notes |
|---|---|---|---|---|
| Salbutamol (albuterol) | SABA | 3-5 min | 4-6 h | Most common reliever; metered-dose inhaler |
| Formoterol | LABA | Rapid (like SABA) | 12 h | Used in AIR strategy; only LABA with rapid onset |
| Salmeterol | LABA | Slow | 12 h | Not for as-needed use; only with ICS |
| Ipratropium | SAMA | 15-30 min | 4-6 h | Added in acute severe attacks |
| Tiotropium | LAMA | Slow | 24 h | Add-on in step 4/5 |
| Theophylline | Methylxanthine | Variable | Variable | Narrow therapeutic index; less used now |
Controllers (Anti-inflammatory)
| Drug | Class | Notes |
|---|---|---|
| Beclomethasone, budesonide, fluticasone | Inhaled corticosteroids (ICS) | Cornerstone of controller therapy |
| Montelukast, zafirlukast | LTRA | Alternative step 2; caution - suicidal ideation (montelukast) |
| Prednisolone | Oral CS | Short courses for exacerbations; long-term only step 5 |
| Cromolyn sodium | Mast cell stabilizer | Prophylaxis; less used now |
Biologics (Step 5 - Severe Asthma)
| Drug | Target | Indication |
|---|---|---|
| Omalizumab | Anti-IgE | Allergic asthma, elevated IgE, blood eos ≥ 0.26 × 10⁹/L |
| Mepolizumab, Reslizumab | Anti-IL-5 | Severe eosinophilic asthma, blood eos ≥ 150-300/μL |
| Benralizumab | Anti-IL-5Rα | Severe eosinophilic asthma |
| Dupilumab | Anti-IL-4Rα (blocks IL-4 + IL-13) | Type 2 asthma with elevated eosinophils or FeNO; also effective in asthma-COPD overlap |
| Tezepelumab | Anti-TSLP (alarmin) | Severe asthma regardless of eosinophil count |
Management of Acute Severe Asthma / Status Asthmaticus
Definition
Status asthmaticus = Acute severe asthma not responding to standard bronchodilator therapy within 30-60 minutes.
Immediate Assessment - Features of Severe/Life-Threatening Attack
| Severity | Features |
|---|---|
| Moderate | PEFR 33-50% best; SpO2 ≥ 92%; speaks in phrases |
| Severe | PEFR < 33% best; SpO2 < 92%; RR > 25; HR > 110; unable to complete sentences |
| Life-threatening | Silent chest, cyanosis, exhaustion, confusion, bradycardia, SpO2 < 92% |
Treatment Protocol
Immediate (A-B-C + Oxygen)
- Oxygen - high flow (target SpO2 94-98%)
- Nebulized SABA (salbutamol 2.5-5 mg) - repeated every 15-20 min or continuous nebulization
- Ipratropium bromide added to SABA (reduces hospitalizations in severe attacks)
- Systemic corticosteroids - oral prednisolone 40-50 mg OR IV hydrocortisone 100 mg 6-hourly; begin within 1 hour; continue 5-7 days
- Position patient upright
If life-threatening / not responding:
6. IV magnesium sulfate (2 g IV over 20 min) - causes smooth muscle relaxation; reduces need for ventilation
7. IV salbutamol infusion (if inadequate response to inhaled)
8. Heliox (helium-oxygen mixture) - reduces airway resistance, improves drug delivery
9. Mechanical ventilation (intubation) - last resort; use permissive hypercapnia strategy
Avoid:
- Sedatives / anxiolytics
- Chest physiotherapy during acute attack
- Beta-blockers (even topical for glaucoma)
- NSAIDs / Aspirin in AERD
Markers of Impending Respiratory Failure (ABG)
- Rising / normal PaCO2 (hypercapnia) - most important
- PaO2 < 60 mmHg on O2
- pH < 7.35
- Falling PEFR despite treatment
Comorbidities that worsen Asthma
- Chronic rhinosinusitis ± nasal polyposis
- Obesity
- GERD
- Inducible laryngeal obstruction (vocal cord dysfunction)
- COPD (asthma-COPD overlap)
- Anxiety / depression
- Obstructive sleep apnea
Differential Diagnosis
- COPD (usually irreversible obstruction, older smoker)
- Cardiac asthma (left heart failure)
- Vocal cord dysfunction / inducible laryngeal obstruction
- Bronchiectasis
- Foreign body aspiration (children)
- Eosinophilic bronchitis
- Tracheobronchomalacia
- Alpha-1 antitrypsin deficiency
Bronchial Thermoplasty
- Bronchoscopic procedure delivering controlled radiofrequency (RF) energy to airways
- Reduces airway smooth muscle mass
- Used in severe persistent asthma not controlled with maximal pharmacotherapy
- 3 sessions (right lower lobe, left lower lobe, both upper lobes)
Key Exam Points
| Point | Fact |
|---|---|
| Most common trigger in children | Viral respiratory infections |
| Hallmark physiological finding | Airway hyperresponsiveness |
| Reversibility criterion | FEV1 increase ≥ 12% AND ≥ 200 mL after SABA |
| Drug causing asthma (most dangerous) | Beta-blockers; also aspirin/NSAIDs (AERD) |
| Silent chest = | Ominous sign - no airflow |
| Normal/rising CO2 in acute attack = | Impending respiratory failure |
| Diurnal variation > 20% | Characteristic of asthma (peak morning dip) |
| Sputum finding | Charcot-Leyden crystals, Curschmann's spirals, Creola bodies |
| SABA monotherapy reliever | No longer recommended (GINA) - must add ICS |
| IV drug for acute severe asthma | Magnesium sulfate 2g IV |
Sources
- Harrison's Principles of Internal Medicine, 22E (2025) - pp. 2260-2270
- Murray & Nadel's Textbook of Respiratory Medicine
- Fishman's Pulmonary Diseases and Disorders
Copd notes
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the content needed for a comprehensive COPD answer. Let me compile.
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
(Archith Boloor exam-style format - Harrison's 22E, Murray & Nadel, Fishman's)
Definition
COPD is a disease state characterized by persistent respiratory symptoms and chronic, progressive, largely irreversible airflow obstruction that is not fully reversible, usually caused by noxious environmental exposures (most commonly cigarette smoking).
COPD is an umbrella term encompassing:
- Emphysema - destruction of alveolar walls with air space enlargement (anatomic definition)
- Chronic bronchitis - chronic cough and phlegm production for at least 3 months in each of 2 consecutive years (clinical definition)
- Small airway disease - narrowing and reduced number of small bronchioles (< 2 mm)
Harrison's 22E, p. 2293
Epidemiology
- 4th leading cause of death in the United States
- Affects > 15 million persons in the US; ~480 million globally (projected 592 million by 2050)
- COPD is more common in males historically, but gender gap is narrowing
Etiology / Risk Factors
Primary Cause
- Cigarette smoking - most important cause in developed countries (accounts for ~80-90%)
- Not all smokers develop COPD (genetic susceptibility determines who develops it)
- Biomass fuel combustion (wood, cow dung, crop residue) - major cause in developing countries
- Vaping and inhaled cannabis - increasingly recognized, especially in adolescents
Other Risk Factors
- Alpha-1 antitrypsin (AAT) deficiency - most important genetic cause; autosomal recessive; PiZZ phenotype; presents as panacinar emphysema, predominantly in lower lobes, in young non-smokers (age 30-40)
- Occupational exposures: VGDF (vapors, gas, dust, fumes); coal mining, gold mining, cotton textile dust
- Air pollution (fine/ultrafine particulate matter)
- Respiratory infections: childhood pneumonia; tuberculosis (tuberculosis-associated COPD - both emphysematous and fibrotic changes + extensive airway remodeling)
- HIV infection (increased risk, especially with low CD4 count)
- Asthma and airway hyperresponsiveness
- Abnormal lung development / low birth weight
- Poor socioeconomic status
Pathology and Pathogenesis
Three Pathological Sites
1. Large Airway Disease (Chronic Bronchitis)
- Mucus gland enlargement (Reid index - mucus gland thickness / bronchial wall thickness; normal < 0.4; in chronic bronchitis > 0.5)
- Goblet cell hyperplasia and metaplasia
- Squamous metaplasia (predisposes to carcinogenesis)
- Neutrophil influx → purulent sputum (elastase is potent secretagogue)
2. Small Airway Disease (< 2 mm)
- Major site of increased airflow resistance in COPD
- Goblet cell metaplasia, mucus plugging
- Peribronchial fibrosis, smooth muscle hypertrophy
- Inflammatory cell infiltration (macrophages, CD8+ T cells)
3. Emphysema (Alveolar Destruction)
| Type | Location | Cause |
|---|---|---|
| Centriacinar (centrilobular) | Central part of acinus (respiratory bronchioles) | Cigarette smoking; upper lobes predominantly |
| Panacinar (panlobular) | Entire acinus uniformly destroyed | Alpha-1 antitrypsin deficiency; lower lobes; also severe smoking |
| Paraseptal (distal acinar) | Distal alveoli, near pleura and septa | Spontaneous pneumothorax in young adults |
| Irregular (paracicatricial) | Around scars | Healed TB, old lung disease |
Protease-Antiprotease Imbalance (Key Mechanism)
- Smoking activates macrophages and neutrophils → release elastase, MMP-9, MMP-12
- These proteases destroy connective tissue (elastin, collagen) of alveolar walls
- Normally balanced by alpha-1 antitrypsin (AAT) and SLPI
- Smoking also oxidatively inactivates AAT - double hit
- AAT deficiency severely reduces this protection → premature, severe emphysema
Oxidative Stress
- Cigarette smoke contains enormous amounts of oxidants
- Activates inflammatory transcription factors (NF-κB)
- Inactivates antiproteases
- Causes direct cellular and DNA damage
Key Inflammatory Cells in COPD
- Macrophages (central role - activated by cigarette smoke)
- CD8+ cytotoxic T lymphocytes (predominant T cell subtype - unlike asthma which is CD4+/Th2)
- Neutrophils (in airway lumen)
- Note: eosinophils are NOT the predominant cell (unlike asthma) - though blood eosinophils guide ICS use
Clinical Features
History - Three Cardinal Symptoms
- Chronic cough (often productive; sometimes dry)
- Sputum production (usually mucoid; purulent during exacerbations)
- Exertional dyspnea (progressive; initially on exertion, eventually at rest)
- Patients date onset to an acute exacerbation, but symptoms predate this
- Activities with significant arm work above shoulder level are particularly difficult
- Activities that allow bracing the arms (pushing shopping cart, treadmill) are better tolerated
Physical Signs
Early COPD: Often normal examination
Moderate-Severe COPD:
- Barrel chest (increased AP diameter) due to hyperinflation
- Use of accessory muscles (sternocleidomastoid, scalenes)
- Tripod position (leaning forward on arms) to facilitate accessory muscle use
- Prolonged expiratory phase with audible wheeze
- Hyperresonant percussion (emphysema)
- Reduced breath sounds, reduced chest expansion
- Paradoxical inward movement of lower ribs on inspiration (Hoover's sign)
Advanced COPD:
- Cyanosis (central)
- Cachexia and weight loss (elevated TNF-α - independent poor prognostic factor)
- Signs of cor pulmonale: elevated JVP, right ventricular heave, loud P2, peripheral edema
Important: Clubbing is NOT a feature of COPD. Its presence should prompt investigation for lung cancer or other causes.
Pink Puffer vs Blue Bloater (Classical Distinction)
| Feature | Pink Puffer (Emphysema-predominant) | Blue Bloater (Chronic Bronchitis-predominant) |
|---|---|---|
| Body habitus | Thin, cachexic | Overweight |
| Cyanosis | Absent (pink) | Present (blue) |
| Dyspnea | Severe | Mild |
| Cough/sputum | Minimal | Copious |
| PaO2 | Relatively maintained | Reduced |
| PaCO2 | Normal or low | Elevated (CO2 retainer) |
| Cor pulmonale | Late | Early |
| Polycythemia | Absent | Present |
| CXR | Hyperinflation, bullae, flat diaphragm | Dirty chest, cardiomegaly |
| Pursed-lip breathing | Prominent | Less prominent |
(Note: most patients have mixed features)
Investigations
Spirometry (Gold Standard for Diagnosis)
Diagnostic criterion: Post-bronchodilator FEV1/FVC < 0.70
GOLD Grading (Severity of Airflow Obstruction)
| GOLD Grade | FEV1 (% predicted) | Severity |
|---|---|---|
| GOLD 1 | ≥ 80% | Mild |
| GOLD 2 | 50-79% | Moderate |
| GOLD 3 | 30-49% | Severe |
| GOLD 4 | < 30% | Very Severe |
GOLD ABE Classification (Guides Treatment)
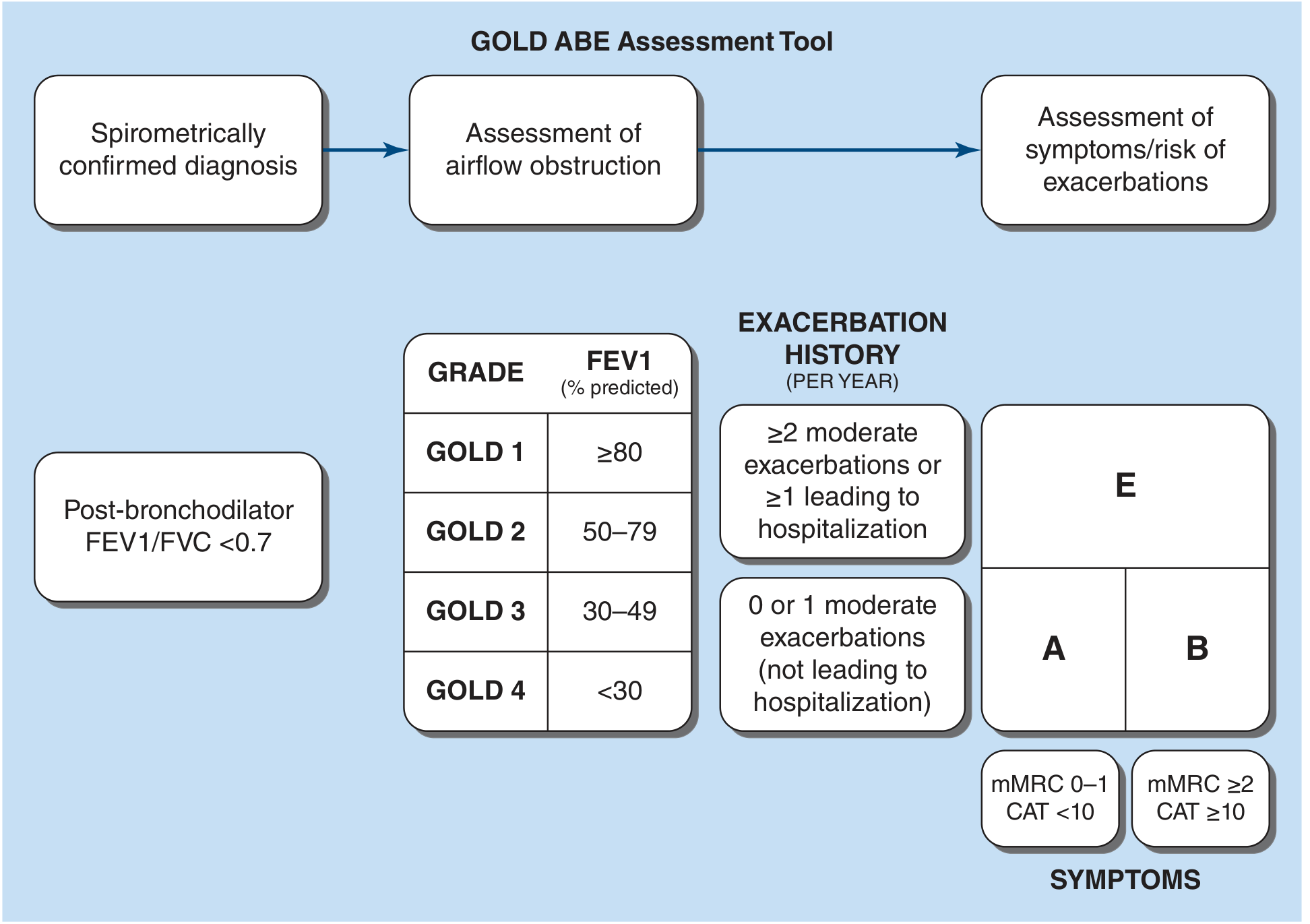
| Group | Symptoms | Exacerbation history |
|---|---|---|
| A | Few symptoms (mMRC 0-1, CAT < 10) | 0 or 1 moderate (no hospitalization) |
| B | More symptoms (mMRC ≥ 2, CAT ≥ 10) | 0 or 1 moderate (no hospitalization) |
| E | Any symptom level | ≥ 2 moderate OR ≥ 1 leading to hospitalization |
Other PFT Findings
- Increased TLC, FRC, RV (air trapping and hyperinflation)
- Reduced DLCO (diffusing capacity) - hallmark of emphysema (alveolar destruction reduces gas exchange surface)
- RV/TLC ratio elevated (air trapping)
- Unlike asthma: < 12% reversibility after bronchodilator (not fully reversible)
Chest X-Ray
- Hyperinflation: flat hemidiaphragms, increased retrosternal air space, barrel-shaped thorax
- Increased AP diameter
- Bullae (emphysema - large lucent areas with thin walls)
- Attenuated vascular markings (emphysema)
- "Dirty chest" appearance (chronic bronchitis - increased bronchovascular markings)
- Enlarged pulmonary arteries (cor pulmonale)
HRCT Chest
- Most sensitive for emphysema detection
- Centrilobular emphysema: scattered lucencies, upper-lobe predominant
- Panacinar emphysema: uniform low attenuation, lower-lobe predominant (AAT deficiency)
- Air trapping on expiratory scans
- Airway wall thickening (chronic bronchitis)
- Mucus plugging (associated with increased mortality)
ABG
- Mild-Moderate: Normal or mild hypoxemia
- Severe: Type 2 respiratory failure (hypoxemia + hypercapnia - PaCO2 > 45 mmHg)
- Chronic hypercapnia: compensated respiratory acidosis (normal pH, elevated HCO3-)
Other Tests
- Alpha-1 antitrypsin level - screen if: early-onset (< 45 yrs), lower-lobe emphysema, non-smoker/minimal smoker, family history
- ECG / Echo - right heart strain, cor pulmonale
- CBC - polycythemia (secondary to chronic hypoxia), eosinophil count (guides ICS use)
- CRP, procalcitonin - during exacerbations
BODE Index (Predicts Mortality Better than FEV1 Alone)
| Variable | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| BMI | > 21 | ≤ 21 | - | - |
| Obstruction (FEV1 % pred) | ≥ 65% | 50-64% | 36-49% | ≤ 35% |
| Dyspnea (mMRC) | 0-1 | 2 | 3 | 4 |
| Exercise (6MWT, meters) | ≥ 350 | 250-349 | 150-249 | ≤ 149 |
- Higher score = worse prognosis
- BODE score ≥ 7 = candidates for lung transplantation evaluation
Management
Three Interventions Proven to Improve Survival
- Smoking cessation (most important)
- Long-term oxygen therapy (LTOT) in chronically hypoxemic patients
- Lung volume reduction surgery (LVRS) in selected emphysema patients
(Triple inhaled therapy - ICS/LABA/LAMA - also reduces mortality in selected patients)
Stable COPD Pharmacotherapy
Group A
- Short-acting bronchodilator as needed (SABA or SAMA)
Group B
- Long-acting bronchodilator (LAMA preferred) - start with single LABA or LAMA
- If symptoms persist: LABA + LAMA
Group E (High exacerbation risk)
- LABA + LAMA as initial treatment
- If blood eosinophils ≥ 300/μL: consider LABA + LAMA + ICS (triple therapy)
- Eosinophil count guides ICS use:
- < 100/μL: ICS unlikely to benefit (do NOT add ICS)
- 100-299/μL: consider ICS if exacerbations on LABA/LAMA
- ≥ 300/μL: strong indication for triple therapy
Drug Classes in COPD
| Drug | Class | Notes |
|---|---|---|
| Salbutamol / terbutaline | SABA | Reliever; as-needed |
| Ipratropium | SAMA | Adds to SABA; used in acute exacerbations |
| Tiotropium | LAMA (24h) | First-line LAMA; reduces exacerbations > LABA |
| Glycopyrronium, aclidinium, umeclidinium | LAMA | Alternatives |
| Salmeterol, formoterol, indacaterol, olodaterol, vilanterol | LABA | Symptomatic; not monotherapy |
| Budesonide, fluticasone, beclomethasone | ICS | Only add in specific indications (eosinophils, exacerbations on LABA+LAMA) |
| Roflumilast | PDE-4 inhibitor | Severe COPD (FEV1 < 50%), chronic bronchitis phenotype, ≥ 1 exacerbation/yr; reduces exacerbations |
| Azithromycin (long-term) | Macrolide | Reduces exacerbations in former smokers; check QT interval, hearing |
| Theophylline | Methylxanthine | Modest bronchodilation; narrow therapeutic index; less used |
| N-acetylcysteine | Mucolytic | Antioxidant; modest reduction in exacerbations |
Non-Pharmacological Management
| Intervention | Details |
|---|---|
| Smoking cessation | Nicotine replacement, varenicline, bupropion; counseling |
| Pulmonary rehabilitation | Most effective non-drug intervention for dyspnea and exercise tolerance; reduces hospitalizations; 6-8 weeks minimum |
| Long-term oxygen therapy (LTOT) | Indication: PaO2 ≤ 55 mmHg; or PaO2 56-59 mmHg with cor pulmonale, polycythemia (Hct > 55%), or edema; ≥ 15 h/day; improves survival |
| Influenza vaccine | Annually - reduces exacerbations |
| Pneumococcal vaccine | All COPD patients |
| COVID-19 + RSV vaccines | Recommended |
| Lung Volume Reduction Surgery (LVRS) | For severe upper-lobe emphysema + low exercise capacity; improves survival + function |
| Bronchoscopic procedures | Endobronchial valves (Zephyr valves), coils for suitable emphysema patients |
| Lung transplantation | End-stage COPD; BODE score ≥ 7; improves quality of life |
COPD Exacerbations
Definition
An acute exacerbation = acute worsening of respiratory symptoms beyond normal day-to-day variation that leads to a change in medication.
Cardinal features (Anthonisen criteria):
- Increased dyspnea
- Increased sputum volume
- Increased sputum purulence
Type 1 (severe): all 3 features
Type 2 (moderate): any 2 features
Type 3 (mild): 1 feature + URTI/fever/wheeze
Precipitating Causes
- Viral infections > 50% (rhinovirus, influenza, parainfluenza, RSV)
- Bacterial infections: Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Chlamydia pneumoniae
- Air pollution, allergens
- Pulmonary embolism (always consider - incidence increased in COPD)
- Medication non-adherence
- No identifiable cause in a significant minority
Assessment of Severity
- Degree of dyspnea and change from baseline
- RR, HR, SpO2
- ABG: PaCO2 > 45 mmHg + pH ≤ 7.35 = respiratory acidosis → NIPPV
- CXR: rule out pneumonia, pneumothorax, cardiac failure (abnormal in ~25%)
Indications for Hospitalization:
- Respiratory acidosis (PaCO2 > 45 mmHg, pH ≤ 7.35)
- New or worsening hypoxemia
- Severe underlying COPD
- Significant comorbidities (heart failure)
- Inadequate home support
Treatment of Acute Exacerbation
1. Oxygen therapy
- Target SpO2 88-92% (avoid over-oxygenation)
- High-flow O2 causes modest rise in PaCO2 (V/Q mismatch) - do not withhold O2 for hypoxemia
2. Bronchodilators
- Nebulized SABA (salbutamol 2.5-5 mg) + SAMA (ipratropium 500 mcg)
- Convert to MDI with spacer when improving
3. Systemic Corticosteroids
- Prednisolone 40 mg oral for 5 days (equivalent to IV hydrocortisone 100 mg 8-hourly)
- Reduces length of stay, hastens recovery, reduces relapse
- Hyperglycemia is most common complication (especially in diabetics)
4. Antibiotics
- Duration: 5-7 days (moderate-severe exacerbations)
- Choices: amoxicillin-clavulanate, doxycycline, azithromycin, or respiratory fluoroquinolone (levofloxacin)
- Based on local resistance patterns
5. Noninvasive Positive Pressure Ventilation (NIPPV/NIV)
- Indication: PaCO2 > 45 mmHg AND pH ≤ 7.35 (respiratory acidosis)
- Reduces mortality, need for intubation, hospital stay
- Contraindications: hemodynamic instability, altered consciousness, inability to cooperate, copious secretions, craniofacial abnormalities
6. Invasive Mechanical Ventilation
- Indications: failed NIPPV, respiratory arrest, severe hypoxemia, hemodynamic instability, altered mental status
- Mortality 17-49% for that hospitalization
- Consider auto-PEEP (dynamic hyperinflation) - ensure adequate expiratory time
Post-Exacerbation Prognosis
- ~20% rehospitalized in 30 days; ~45% in 1 year
- ~20% mortality in the year following hospital discharge
Cor Pulmonale
- Right heart failure due to COPD (pulmonary hypertension from hypoxic vasoconstriction)
- Signs: elevated JVP, right ventricular heave, loud P2, pansystolic murmur (TR), peripheral edema
- ECG: right axis deviation, P pulmonale (tall P in II > 2.5 mm), RV hypertrophy (R > S in V1)
- Echo: dilated RV, TR, raised RVSP
- Treatment: LTOT (most effective), diuretics for edema, vasodilators not generally effective
Key Exam Points
| Point | Fact |
|---|---|
| Diagnostic criterion | Post-bronchodilator FEV1/FVC < 0.70 |
| Most important cause | Cigarette smoking (80-90%) |
| Genetic cause | Alpha-1 antitrypsin deficiency (panacinar, lower lobe) |
| Reid index (chronic bronchitis) | Mucus gland/bronchial wall > 0.5 (normal < 0.4) |
| Emphysema type in smokers | Centrilobular (upper lobes) |
| Emphysema type in AAT deficiency | Panacinar (lower lobes) |
| Reduced DLCO | Hallmark of emphysema |
| Clubbing in COPD | NOT a feature - investigate for lung cancer |
| O2 target in COPD | SpO2 88-92% (not > 94%) |
| NIPPV indication | PaCO2 > 45 mmHg + pH ≤ 7.35 |
| Survival-improving interventions | Smoking cessation > LTOT > LVRS; triple therapy |
| LTOT indication | PaO2 ≤ 55 mmHg; ≥ 15h/day |
| PDE-4 inhibitor | Roflumilast (severe COPD + chronic bronchitis phenotype) |
| Antibiotic for exacerbation | 5-7 days; amox-clav / doxycycline / levofloxacin |
| Steroids for exacerbation | Prednisolone 40 mg × 5 days |
| BODE index | BMI + Obstruction + Dyspnea + Exercise; predicts mortality |
Sources
- Harrison's Principles of Internal Medicine, 22E (2025) - pp. 2293-2302
- Murray & Nadel's Textbook of Respiratory Medicine
- Fishman's Pulmonary Diseases and Disorders
Brochiectasis
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full exam-style answer.
BRONCHIECTASIS
(Archith Boloor exam-style format - Harrison's 22E, Fishman's, Murray & Nadel)
Definition
Bronchiectasis is a permanent, irreversible abnormal dilation of the bronchi and bronchioles resulting from destruction of the elastic and muscular components of the bronchial wall, usually due to infection and inflammation.
Harrison's 22E, p. 2286
Morphological Types (Reid's Classification)
| Type | Description | Notes |
|---|---|---|
| Cylindrical (Tubular) | Uniform dilation of bronchi with straight, regular outline | Most common type |
| Varicose (Fusiform) | Irregular dilation resembling varicose veins; alternating constrictions and dilations | Intermediate severity |
| Cystic (Saccular) | Progressive dilation ending in cyst/sac formation (cul-de-sacs) | Most severe; associated with severe infection |
Etiology
By Pattern of Lung Involvement
FOCAL Bronchiectasis (localized area):
- Airway obstruction - extrinsic (lymphadenopathy, tumor mass) or intrinsic (foreign body, tumor, scar/stenosis)
- Congenital bronchial atresia
DIFFUSE Bronchiectasis (widespread):
1. Infectious Causes (most common overall)
- Post-infectious (historically most common): whooping cough (Bordetella pertussis), measles (rubeola), influenza, adenovirus, Klebsiella, S. aureus
- Tuberculosis - most common cause in developing countries (cavitary disease + parenchymal destruction)
- Non-tuberculous mycobacteria (NTM) - especially MAC (M. avium-intracellulare complex)
- Granulomatous fungi: Histoplasma capsulatum
- Lung abscess, pneumonia
2. Congenital / Genetic Causes
- Cystic fibrosis (CF) - most common cause in young adults in developed countries; upper-lobe predominant
- Primary Ciliary Dyskinesia (PCD / Kartagener's syndrome) - autosomal recessive; defective dynein arms → immotile cilia → poor mucociliary clearance; Kartagener's triad = bronchiectasis + sinusitis + situs inversus
- Alpha-1 antitrypsin deficiency
- Hypogammaglobulinemia (primary immunodeficiencies: common variable immunodeficiency - CVID, X-linked agammaglobulinemia)
- Cartilage defects: Mounier-Kuhn syndrome (tracheobronchomegaly), Williams-Campbell syndrome (central airway bronchiectasis)
- Congenital cystic disease
3. Immunodeficiency
- Primary (hypogammaglobulinemia, CVID)
- Secondary (HIV, post-transplant bronchiolitis obliterans syndrome - BOS)
4. Autoimmune / Rheumatologic
- Rheumatoid arthritis
- Sjogren's syndrome
- Inflammatory bowel disease (IBD)
- SLE
5. Allergic / Immune-mediated
- Allergic Bronchopulmonary Aspergillosis (ABPA) - immune reaction to Aspergillus; central airway bronchiectasis; associated with refractory asthma; high IgE, eosinophilia, Aspergillus precipitins
6. Chronic Aspiration
- Esophageal motility disorders (scleroderma, achalasia)
- Gastro-oesophageal reflux
- Neuromuscular disorders
- Lower-lobe predominant
7. Miscellaneous
- Yellow nail syndrome (bronchiectasis + pleural effusion + yellow discoloured nails + lymphoedema)
- Traction bronchiectasis (from lung fibrosis - IPF, post-radiation)
- Sarcoidosis, PMF/silicosis
- Young's syndrome (obstructive azoospermia + sinusitis + bronchiectasis)
8. Idiopathic
- 25-50% of cases after workup
Anatomic Distribution - Clue to Etiology
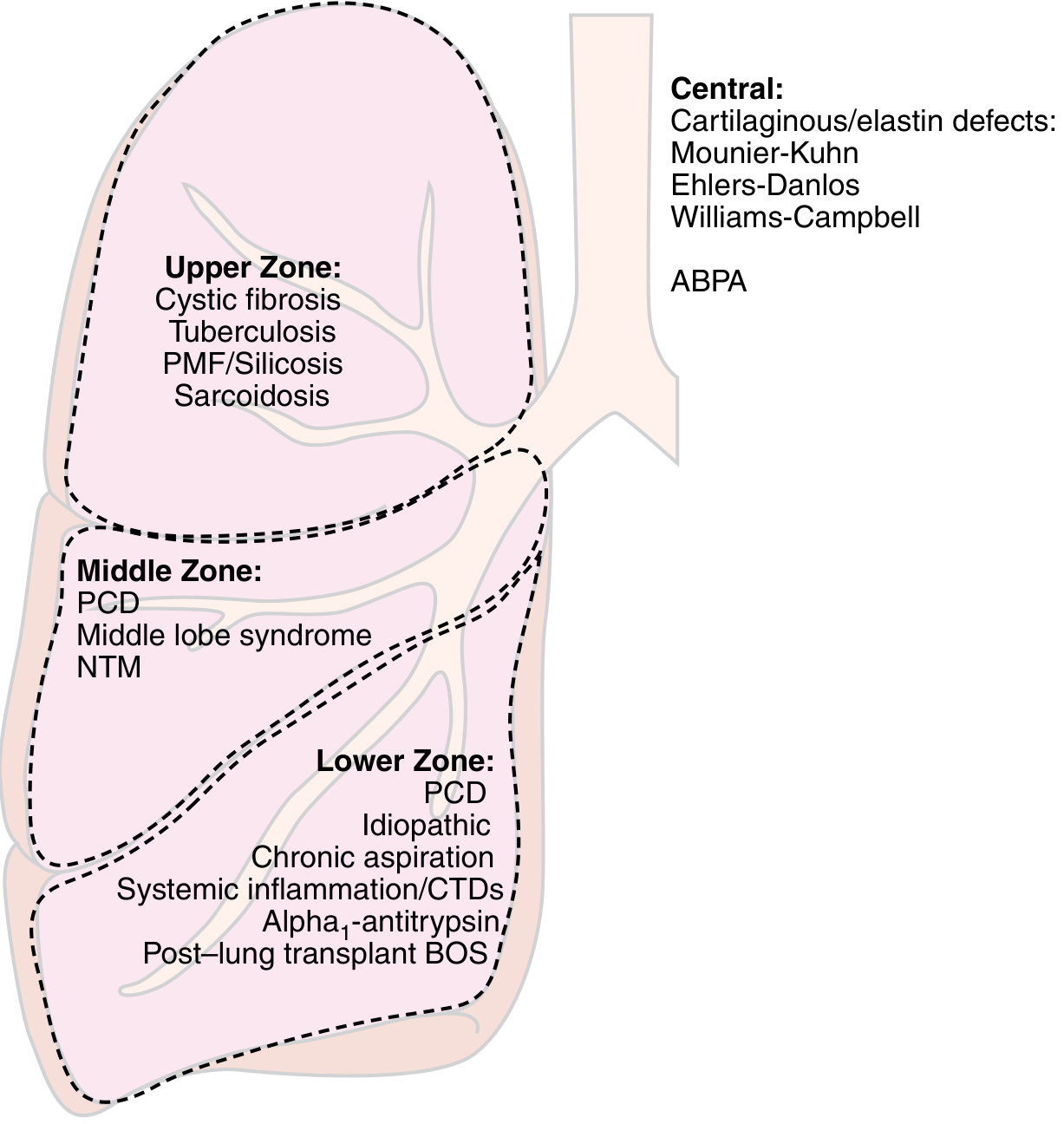
| Zone | Etiology |
|---|---|
| Upper zone | Cystic fibrosis, Tuberculosis, Sarcoidosis, PMF/Silicosis, Post-radiation |
| Middle zone | PCD (Primary Ciliary Dyskinesia), NTM (MAC), Middle lobe syndrome |
| Lower zone | PCD, Idiopathic, Chronic aspiration, CTDs (RA, Sjogren's), Alpha-1-antitrypsin, Post-transplant BOS |
| Central airways | ABPA, Mounier-Kuhn syndrome, Williams-Campbell syndrome, Ehlers-Danlos |
Pathogenesis - "Vicious Cycle Hypothesis"
The central mechanism of infectious bronchiectasis:
Susceptibility to infection + Poor mucociliary clearance
↓
Microbial colonization of bronchial tree
↓ (organisms like Pseudomonas aeruginosa evade host defenses)
Chronic airway inflammation (neutrophil-dominant)
↓ (release of elastase, MMP, reactive oxygen species, proinflammatory cytokines)
Airway wall destruction (loss of elastin, smooth muscle, cartilage)
↓
Further bronchial dilation and impaired clearance
↓
Ongoing infection and inflammation → cycle repeats and worsens
Additional mechanism: Inflammatory cells in small airways damage larger airway walls via proteases and cytokines → airflow obstruction.
Alpha-1 antitrypsin neutralizes neutrophil elastase - its deficiency therefore predisposes to both bronchiectasis and emphysema.
Clinical Features
Symptoms
- Chronic productive cough - most common symptom; persistent; thick, tenacious, mucopurulent sputum
- Sputum classically described as three-layered on standing (frothy top + mucopurulent middle + thick sediment bottom) - Reid's 3-layer sign
- Haemoptysis - common; can be massive (bronchial arteries dilated and tortuous)
- Breathlessness / exertional dyspnea
- Recurrent chest infections / pneumonia (same lobe)
- Pleuritic chest pain
- Systemic features: fever, weight loss, fatigue (during exacerbations)
Signs
- Coarse crackles (crepitations) - most consistent sign; inspiratory, basal or localised
- Wheeze (bronchospasm)
- Clubbing of fingers (common in bronchiectasis - unlike COPD where clubbing should trigger cancer workup)
- Cyanosis (advanced disease)
- Signs of cor pulmonale (late)
- Signs of underlying disease (joint deformity in RA, nasal polyps in CF/ABPA, situs inversus in Kartagener's)
Investigations
Imaging
Chest X-Ray (CXR)
- Often normal in early disease (insensitive)
- Tram-track shadows - dilated bronchi seen end-on as parallel lines ("tram tracks")
- Ring shadows / cystic spaces (cystic bronchiectasis)
- Peribronchial thickening (honeycombing appearance)
- Crowding of lung markings (from volume loss)
- CXR may show causal lesion (old TB, pleural scarring, lymphadenopathy)
HRCT Chest (Gold Standard / Investigation of Choice)
CT Diagnostic Criteria (International consensus - any ONE of):
- Inner or outer airway-artery diameter ratio ≥ 1.5 (signet ring sign - bronchus bigger than accompanying vessel)
- Lack of airway tapering (airways fail to narrow as they proceed distally)
- Visibility of airways within 1 cm of the pleural surface (normal airways not visible this peripherally)
- Bronchial wall thickening in dilated airways
- Tree-in-bud pattern (mucus-filled bronchioles)
- Cysts emanating from bronchial walls (cystic bronchiectasis)
Signet ring sign = cross-sectional bronchial diameter ≥ 1.5x the adjacent pulmonary artery (most characteristic CT finding)
Clinical diagnosis requires CT criteria + at least TWO of:
- Cough most days of the week
- Sputum production most days of the week
- History of exacerbations
Pulmonary Function Tests
- Obstructive pattern most common (FEV1/FVC < 0.70)
- Sometimes mixed obstructive + restrictive
- FVC and FEV1 both reduced in severe disease
- Not fully reversible (unlike asthma)
Sputum
- Gram stain and culture (most important): common organisms:
- Haemophilus influenzae (most common)
- Pseudomonas aeruginosa (poor prognosis; in advanced/CF-related disease)
- S. pneumoniae, Moraxella catarrhalis, S. aureus
- NTM (MAC) - consider in nonsmoking women > 50 with mid-zone disease
- AFB stain + culture (TB / NTM)
- Fungal culture (ABPA)
Blood Tests
- CBC: eosinophilia (ABPA, parasites), neutrophilia (bacterial infection)
- Immunoglobulins (IgG, IgA, IgM) - screen for hypogammaglobulinemia
- Serum IgE (total and Aspergillus-specific), Aspergillus precipitins, skin prick test - for ABPA
- Sweat chloride test - screen for CF (Cl- > 60 mEq/L = positive)
- Alpha-1 antitrypsin levels
- Rheumatoid factor, ANA, ANCA - connective tissue diseases
- HIV testing
- Nasal nitric oxide (nNO) - reduced (< 77 nL/min) in Primary Ciliary Dyskinesia
Bronchoscopy
- Mandatory in focal bronchiectasis - exclude airway obstruction by mass or foreign body
- BAL for culture (including NTM, fungi)
- Biopsy for cilia ultrastructure (electron microscopy for PCD - absent dynein arms)
Special Conditions
Kartagener's Syndrome (Primary Ciliary Dyskinesia)
- Autosomal recessive
- Triad: Bronchiectasis + Chronic sinusitis + Situs inversus (dextrocardia)
- Due to absent/abnormal dynein arms on cilia → immotile cilia
- Males: infertility (immotile sperm)
- Diagnosis: nasal NO < 77 nL/min + electron microscopy of cilia (absent dynein arms) + genetic testing
ABPA (Allergic Bronchopulmonary Aspergillosis)
- Hypersensitivity to Aspergillus fumigatus in asthmatics
- Central proximal bronchiectasis (pathognomonic)
- Criteria: refractory asthma + elevated total IgE > 1000 IU/mL + elevated Aspergillus-specific IgE + Aspergillus precipitins + eosinophilia
- CXR/CT: central bronchiectasis, "finger-in-glove" opacities (mucus plugging), consolidation (often fleeting)
- Treatment: oral corticosteroids + itraconazole/voriconazole
Young's Syndrome
- Males: obstructive azoospermia + chronic sinusitis + bronchiectasis
- Normal cilia ultrastructure (unlike PCD)
- Mechanism: abnormal mucus / epididymal obstruction
Management
Goals
- Control active infection - reduce microbial load
- Improve secretion clearance (bronchial hygiene)
- Treat underlying cause
- Manage complications (haemoptysis, cor pulmonale)
Airway Clearance Techniques (Bronchial Hygiene) - Cornerstone
- Postural drainage - positioning to drain affected segments by gravity (historically: head-down position)
- Chest physiotherapy - manual percussion (hand clapping) or mechanical
- Oscillatory PEP devices (Flutter valve, Acapella) - positive expiratory pressure + oscillation loosens mucus
- High-frequency chest wall oscillation vest
- Huffing technique
- Hypertonic saline nebulisation - increases mucociliary clearance (reduces exacerbations)
- Nebulized bronchodilators (pre-clearance)
- Pulmonary rehabilitation + regular exercise - improves secretion clearance + exercise capacity
DNase (Dornase alfa): Recommended in CF-related bronchiectasis ONLY. NOT recommended in non-CF bronchiectasis (may cause harm - increased exacerbations in non-CF).
Antibiotic Therapy
Acute Exacerbations:
- Duration: 7-14 days (minimum 7-10 days)
- Common pathogens: H. influenzae, Pseudomonas aeruginosa
- Oral: amoxicillin-clavulanate, ciprofloxacin (if Pseudomonas suspected)
- IV: for severe exacerbations, Pseudomonas-directed (piperacillin-tazobactam, ceftazidime, meropenem)
- Pseudomonas eradication protocol in newly colonized patients (intensive courses)
Long-term / Prophylactic Antibiotics (to reduce exacerbation frequency):
- Azithromycin 250 mg three times/week or 500 mg daily 3 days/week - reduces exacerbations; anti-inflammatory + antimicrobial properties; check QT interval and audiology
- Nebulized colistin or tobramycin - for chronic Pseudomonas colonization
NTM / MAC Infection:
- Macrolide (azithromycin/clarithromycin) + rifampicin + ethambutol - triple therapy
- Prolonged treatment (12-18 months or 12 months after negative culture)
- Check macrolide susceptibility
Anti-Inflammatory Therapy
- Inhaled corticosteroids (ICS): may reduce dyspnea and sputum; no significant effect on exacerbation rate or lung function; risk of immunosuppression in infected airways
- Oral corticosteroids: important for ABPA-associated bronchiectasis; not routine
- Statins: anti-inflammatory benefit under investigation
- Oral neutrophil elastase inhibitor (brensocatib): phase 2 trial showed reduced exacerbations (awaiting phase 3 confirmation)
Surgery
- Indications: focal bronchiectasis causing recurrent infections refractory to medical therapy; massive haemoptysis (segmentectomy/lobectomy)
- Not suitable for diffuse disease
- Bronchial artery embolization for massive haemoptysis (bridge to surgery or definitive in diffuse disease)
Lung Transplantation
- For end-stage bilateral diffuse bronchiectasis (especially CF)
Complications
- Massive haemoptysis (life-threatening; from dilated bronchial arteries)
- Recurrent pneumonia / lung abscess
- Empyema
- Cor pulmonale (pulmonary hypertension → right heart failure)
- Amyloidosis (AA type - rare complication of chronic infection)
- Respiratory failure (hypoxaemia + hypercapnia)
- Pneumothorax (uncommon)
- Brain abscess (haematogenous spread in severe infection)
Key Exam Points
| Point | Fact |
|---|---|
| Definition | Permanent, irreversible bronchial dilation |
| Most common morphological type | Cylindrical/tubular |
| Most severe type | Cystic/saccular |
| Most common cause in developing countries | Pulmonary tuberculosis |
| Most common cause in young adults (developed world) | Cystic fibrosis |
| Most common organism | Haemophilus influenzae (mild-moderate); Pseudomonas (advanced) |
| Most consistent clinical sign | Coarse crackles (crepitations) |
| Clubbing | PRESENT in bronchiectasis (unlike COPD where it needs investigation) |
| Imaging of choice | HRCT chest |
| Classic CT sign | Signet ring sign (bronchus ≥ 1.5x adjacent artery) + tram-track sign |
| Kartagener's triad | Bronchiectasis + sinusitis + situs inversus |
| ABPA = | Central bronchiectasis + asthma + elevated IgE + eosinophilia |
| DNase | Only in CF bronchiectasis (NOT non-CF) |
| Airway clearance device | Flutter valve / OPEP device |
| Long-term antibiotic | Azithromycin (3x/week) |
| Surgery indication | Focal bronchiectasis refractory to medical treatment |
| Massive haemoptysis management | Bronchial artery embolization |
| 3-layer sputum | Frothy (top) + mucopurulent (middle) + sediment (bottom) |
Sources
- Harrison's Principles of Internal Medicine, 22E (2025) - pp. 2286-2287
- Fishman's Pulmonary Diseases and Disorders - pp. 1579-1584
- Murray & Nadel's Textbook of Respiratory Medicine
Lobar pneumonia
Finding Sources
Finding Sources
Lobar pleumonia
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.