hi
Hi! How can I help you today?
enteric fever
Reading File
Finding Sources
Searching PubMed
"enteric fever" AND "typhoid"
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information. Let me compile a complete response.
Enteric Fever (Typhoid Fever)
Definition
Enteric fever is a systemic illness caused by dissemination of Salmonella enterica serovar Typhi (typhoid fever) or Paratyphi A, B, or C (paratyphoid fever). The term "enteric fever" was proposed in 1869 to distinguish it from typhus, based on its anatomical association with Peyer's patches and mesenteric lymph nodes.
Etiology & Pathogenesis
- Causative organisms: S. Typhi and S. Paratyphi — humans are the only known reservoir
- Transmission: fecal-oral via contaminated food/water; rarely from chronic carriers, healthcare settings, or sexual contact
- Organism invades gut epithelium → penetrates Peyer's patches → lymphatic spread → systemic dissemination via mononuclear phagocytes
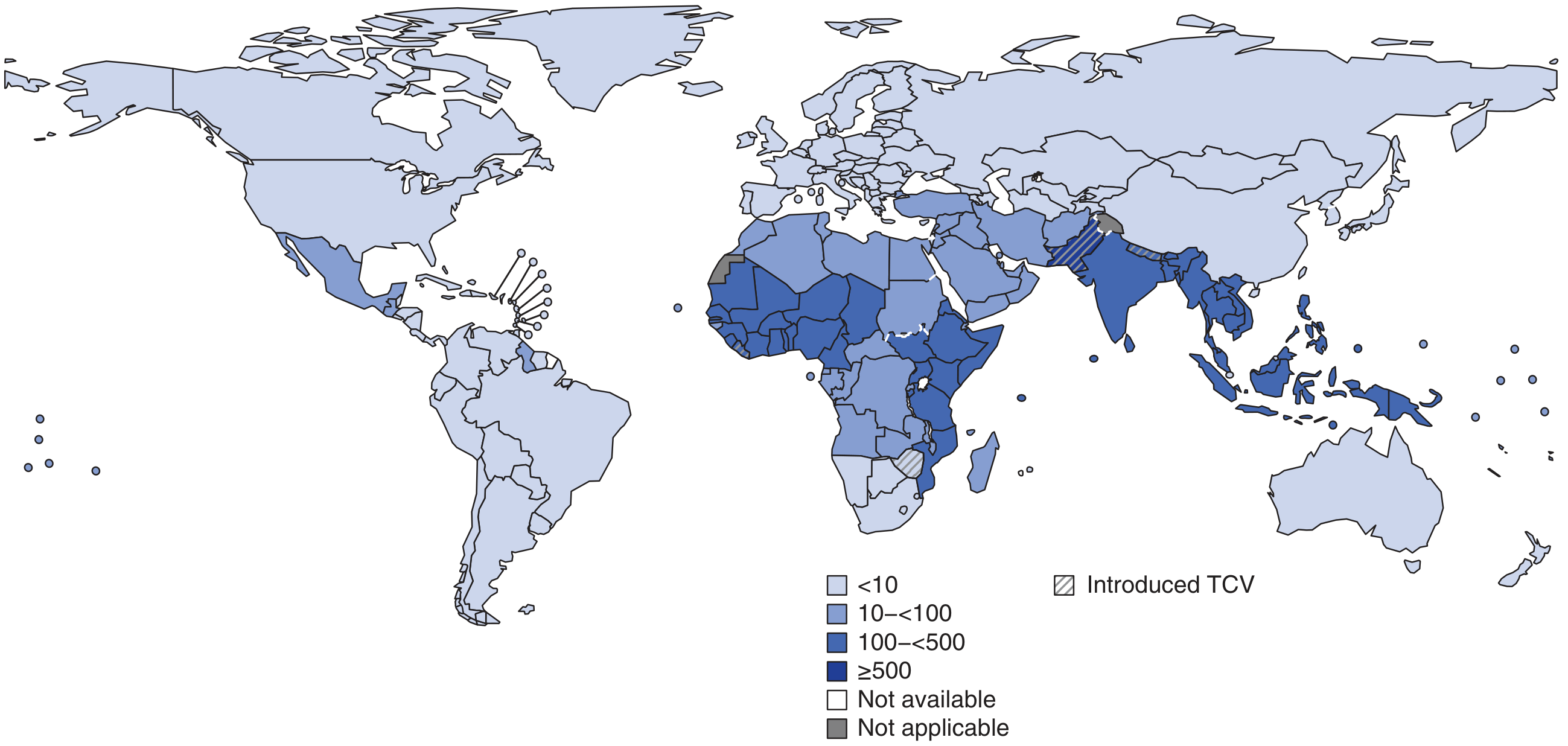
Epidemiology
- 9.2–21 million typhoid cases/year; 5 million paratyphoid cases; 110,000–280,000 deaths annually
- Highest burden: Indian subcontinent (India, Pakistan, Bangladesh, Nepal), Eastern Mediterranean, Africa — can exceed 1,000 cases/100,000 children in some urban areas
- Correlates with mixing of drinking water and sewage; more common in urban poor areas and young children/adolescents
- In developed nations, most cases are travel-associated (78%), particularly from Indian subcontinent
Drug Resistance (Critical)
| Resistance Type | Details |
|---|---|
| MDR (multidrug-resistant) | Plasmid-encoded resistance to chloramphenicol, ampicillin, TMP-SMX; emerged 1980s |
| DSC (decreased susceptibility to ciprofloxacin) | MIC ≥0.125 μg/mL; MIC ≥1 μg/mL = full resistance; associated with clone H58 |
| XDR (extensively drug-resistant) | Emerged 2016 in Sindh, Pakistan; additional resistance to fluoroquinolones + 3rd-gen cephalosporins |
Clinical Course
Incubation: 5–21 days (mean 10–14 days) — depends on inoculum size, vaccination status
Week-by-Week Progression
| Week | Features |
|---|---|
| Week 1 | Stepwise rising fever (38.8–40.5°C), headache (80%), chills (35–45%), cough (30%), anorexia (55%), relative bradycardia (~50%), rose spots appear |
| Week 2 | Sustained high fever, abdominal distension/pain, hepatosplenomegaly, rose spots prominent, potential diarrhea or constipation |
| Weeks 3–4 | Risk of serious complications — GI bleeding (6%), intestinal perforation (1%), neuropsychiatric symptoms |
Key Physical Signs
- Rose spots: Faint salmon-colored, blanching maculopapular rash on trunk/chest; seen in ~30% (difficult to detect in dark-skinned patients)
- Relative bradycardia (pulse-temperature dissociation): up to 50%
- Hepatosplenomegaly: ~50% of patients
- Coated tongue: 51–56%

Complications (~27% of hospitalized patients)
- GI bleeding (6%) and intestinal perforation (1%) — from necrosis of ileocecal Peyer's patches; life-threatening, require surgery
- Neurologic: meningitis, Guillain-Barré, neuritis, "muttering delirium" / coma vigil (2–40%)
- Hemophagocytic syndrome, DIC, pancreatitis, hepatitis, myocarditis, endocarditis, orchitis, pneumonia
- Relapse: 10% within 2–3 weeks of fever resolution
- Chronic carriage: 2–5% shed S. Typhi >1 year (more common in women, biliary disease); associated with increased gallbladder cancer risk
Diagnosis
- Gold standard: Culture isolation of S. Typhi / Paratyphi
- Blood culture: positive in 40–80% (best in first 2 weeks)
- Bone marrow culture: most sensitive (~90%), even after antibiotics started
- Stool/urine culture: positive mainly in week 2–3
- Rose spot biopsy culture also possible
- CBC: Leukopenia/neutropenia in 15–25%; leukocytosis may occur in children or with perforation
- Liver enzymes: Moderately elevated
- Widal test: Agglutination titers to O and H antigens — low specificity, poor positive predictive value; not recommended as sole test
- Rapid antigen tests: Various formats available, but none yet replace culture
Treatment
| Antibiotic | Use |
|---|---|
| Azithromycin | Oral; preferred for uncomplicated typhoid, especially DSC strains |
| Ceftriaxone / 3rd-gen cephalosporins | IV; drug of choice for severe/MDR enteric fever |
| Fluoroquinolones (ciprofloxacin) | Avoid where DSC/XDR prevalent (Indian subcontinent); unreliable |
| Chloramphenicol, ampicillin, TMP-SMX | Avoid if MDR suspected |
| Carbapenems | For XDR strains |
- Steroids (dexamethasone) + antibiotics for severe disease with altered consciousness/shock
- Surgical intervention for perforation
Prevention
- Safe water, sanitation, hand hygiene
- Vaccines:
- Vi polysaccharide vaccine (ViCPS): IM, >2 years, ~55–72% effective
- Ty21a (oral live attenuated): >6 years, 4-dose series
- Typhoid Conjugate Vaccine (TCV): Vi antigen conjugated to tetanus toxoid; superior immunogenicity, approved from 6 months; 2025 Cochrane review confirms TCVs are highly effective and recommended for endemic regions (PMID: 40326553)
- Vaccines do not protect against S. Paratyphi
Chronic Carrier State
- 2–5% become chronic carriers (>1 year shedding)
- Organisms survive in gallbladder biofilms on gallstones
- Treatment: Prolonged antibiotic course (ciprofloxacin or ampicillin × 4–6 weeks); cholecystectomy may be needed
- Carriers are notifiable in most jurisdictions and excluded from food handling
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Medical Microbiology 9e
This is a shared conversation. Sign in to Orris to start your own chat.