Tilt table test
Reading File
Finding Sources
Searching the Web
tilt table test syncope diagnosis protocol interpretation
Searching PubMed
"tilt table test" AND syncope
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive information from multiple authoritative textbooks and the image. Let me compile the full answer.
Tilt Table Test (Head-Up Tilt Table Testing / HUTT)
Definition and Principle
The tilt table test is a diagnostic procedure for evaluating patients with suspected neurally mediated syncope (NMS), also called neurocardiogenic or vasovagal syncope. It exploits the principle that orthostatic stress - prolonged upright posture - causes venous pooling in susceptible individuals, forcing the autonomic nervous system to work without assistance from the skeletal muscle pump. This may provoke the heart rate and blood pressure patterns that trigger syncope.
- Braunwald's Heart Disease, p. 689
- Fuster and Hurst's The Heart, 15th Ed., p. 1260
Protocol
| Phase | Details |
|---|---|
| Pre-tilt stabilization | Patient supine for 20-45 minutes |
| Tilt angle | 60-80 degrees (70 degrees most common) |
| Duration of tilt | 30-45 minutes with continuous HR and BP monitoring |
| Pharmacologic provocation | Isoproterenol (1-3 µg/min, titrated to increase HR ≥25% above baseline) or sublingual nitroglycerin (300-400 µg spray after 20-minute unmedicated upright phase) |
The two provocative agents are equivalent in diagnostic accuracy. Provocation increases sensitivity but reduces specificity.
Indications
Standard indications (Fuster & Hurst, Table 39-5):
- Unexplained recurrent syncope, or single syncopal episode associated with injury (or significant risk of injury), in the absence of organic heart disease
- Same criteria in the setting of organic heart disease, after cardiac causes have been excluded
- When the cause of syncope is known (e.g., asystole) but confirming NMS susceptibility would alter treatment
Additional uses where it may be helpful:
- Differentiating convulsive syncope from epilepsy
- Evaluation of recurrent near-syncope or dizziness
- Autonomic failure syndromes
- Exercise- or post-exercise-induced syncope (when stress testing cannot reproduce the episode)
- Recurrent unexplained falls
- Diagnosing psychogenic pseudosyncope (loss of consciousness with normal HR, BP, EEG, and transcranial Doppler)
- Patient education and teaching counterpressure maneuvers
The 2017 ACC/AHA/HRS syncope guidelines give tilt-table testing a Class IIa, LOE B-NR recommendation for suspected vasovagal syncope when the diagnosis remains unclear after initial evaluation.
Positive Test Criteria
A positive test = reproduction of the patient's presyncopal or syncopal symptoms accompanied by hypotension, bradycardia, or both.
A negative test is characterized by a moderate increase in HR and maintenance of systolic BP above 90 mmHg without symptoms throughout the planned study duration.
Induction of reflex hypotension/bradycardia without reproduction of syncope points toward NMS but is a less specific response.
Five Patterns of Abnormal Response
(From Fuster & Hurst, based on the VASIS classification):
| # | Pattern | Hemodynamic Features |
|---|---|---|
| 1 | Classic neurocardiogenic (vasovagal) | Abrupt BP drop + significant HR drop |
| 1b | Vasodepressor | Abrupt BP drop WITHOUT significant HR change |
| 2 | Dysautonomic (delayed orthostatic) | Gradual progressive BP fall, little HR change; seen in autonomic failure syndromes |
| 3 | Postural tachycardic (POTS) | HR increase >30 bpm or HR >120 bpm within the first 10 minutes of tilt |
| 4 | Cerebral syncope | Loss of consciousness without systemic hypotension; intense cerebral vasoconstriction on transcranial Doppler + cerebral hypoxia on EEG |
| 5 | Psychogenic | Loss of consciousness without systemic hypotension, normal EEG, normal transcranial Doppler |
The mixed pattern (combined BP drop + bradycardia/asystole) is the most common form of neurally mediated syncope.
The three main neurally mediated patterns are shown below (cardiovagal, vasodepressor, and mixed):
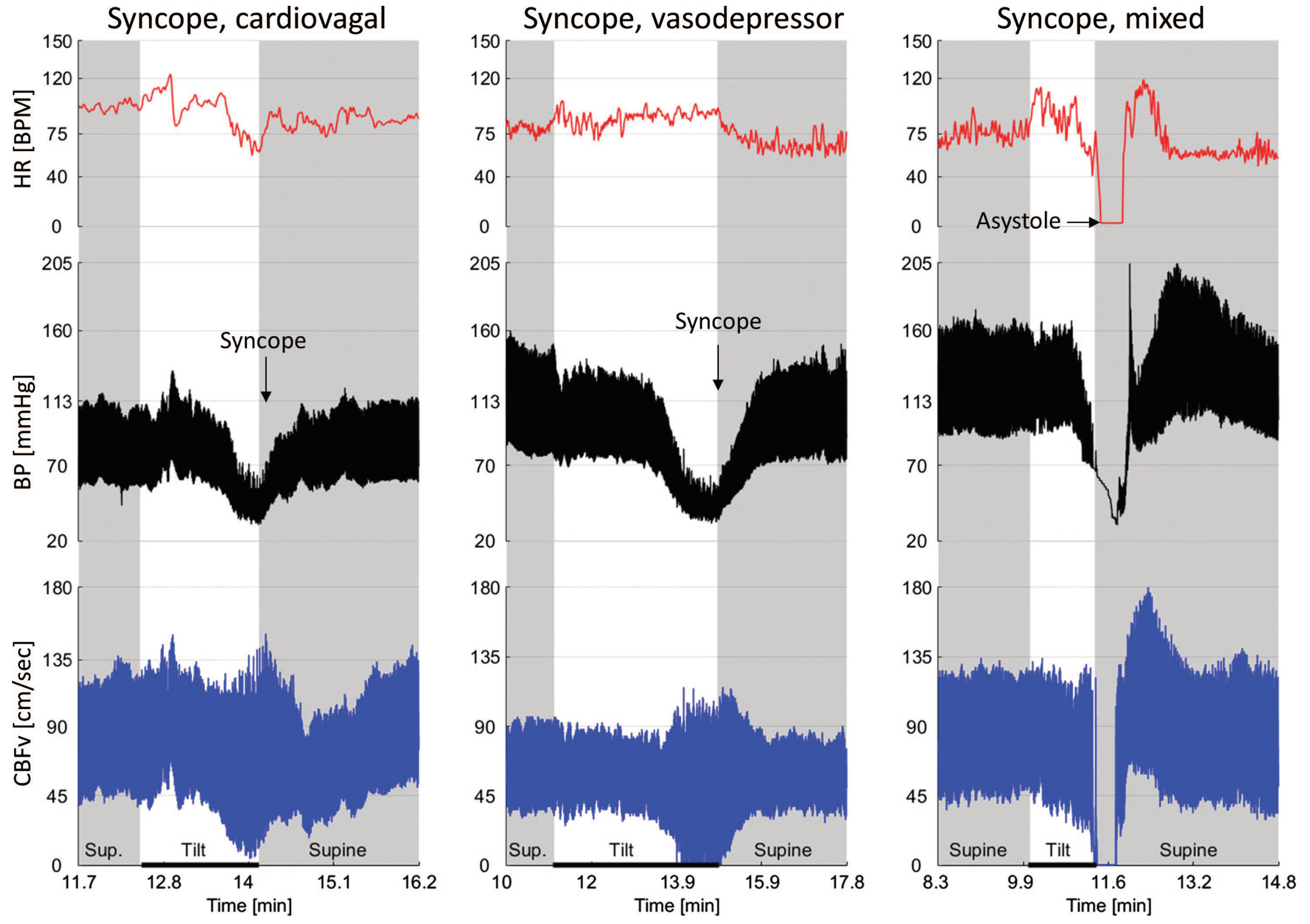
Figure: Adams & Victor's Principles of Neurology - cardiovagal syncope shows isolated HR drop, vasodepressor shows isolated BP drop, mixed (most common) shows asystole with BP collapse.
Diagnostic Performance
| Parameter | Value |
|---|---|
| Specificity (without provocation) | ~90% |
| Specificity (with provocation) | Significantly lower |
| Sensitivity | 20-74% (highly variable) |
| Reproducibility (initially positive test) | 80-90% |
| Reproducibility (initially negative test) | 30-90% |
Important caveats:
-
Sensitivity is only 26-56% even by the best criteria
-
A positive result is not specific for vasovagal syncope - it can be positive in patients without any syncope history, and can trigger vagal reflexes in patients with syncope due to structural heart disease or arrhythmias, potentially leading to misdiagnosis
-
The ISSUE trial showed spontaneous syncopal episodes are more often associated with significant bradycardia than tilt-induced episodes
-
Tilt testing is not useful for assessing treatment efficacy in NMS
-
Symptom to Diagnosis, 4th Ed., p. 7382-7395
-
Braunwald's Heart Disease, p. 689
When NOT to Test
- When the diagnosis of vasovagal syncope can already be established confidently from history and physical examination alone
- When a cardiac cause has not yet been excluded in a patient with structural heart disease
- Routine tilt testing without specific indication
Contraindications / Cautions
- Active or recent MI, significant left ventricular outflow obstruction, critical coronary artery disease (isoproterenol provocation particularly risky)
- Severe aortic stenosis or HOCM
Recent Evidence
Three recent high-level publications are relevant:
- Head-up tilt testing in older syncope patients (Systematic Review, 2025) - PMID 40207380 - examines performance specifically in older patients
- HUTT in hypertrophic cardiomyopathy and unexplained syncope (Meta-Analysis, 2025) - PMID 39017965 - limited diagnostic yield in HCM
- HUTT in suspected vasovagal syncope: meta-regression modelling (Meta-Analysis, 2026) - PMID 40976356 - latest evidence on test characteristics
These recent meta-analyses continue to affirm the limited sensitivity of the test and the importance of careful patient selection.
This is a shared conversation. Sign in to Orris to start your own chat.