Urticaria
Reading File
Finding Sources
Searching PubMed
urticaria management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
I now have a thorough set of data. Let me compile a comprehensive response on urticaria.
Urticaria (Hives)
Definition
Urticaria (hives) is one of the most common cutaneous reaction patterns, characterized by well-circumscribed, raised wheals with erythematous serpiginous borders and blanched centers. Individual lesions last <24 hours, are intensely pruritic, migrate around the body, and leave no bruising or scarring. Angioedema, which involves deeper dermis and subcutaneous tissues, co-exists in roughly 40% of cases. - Harrison's Principles of Internal Medicine 22E, p. 2849
Classification
| Category | Subtypes | Key Features |
|---|---|---|
| Acute urticaria | Allergic, infection-triggered, drug-induced | Duration <6 weeks; >2/3 of new cases |
| Chronic spontaneous urticaria (CSU) | Autoimmune (~45%), idiopathic | Duration ≥6 weeks, no identifiable trigger; peaks 3rd-4th decade |
| Chronic inducible urticaria | Physical subtypes (below) | Triggered by a specific physical stimulus |
Inducible (Physical) Subtypes
| Subtype | Trigger | Clinical Clue |
|---|---|---|
| Dermatographism | Firm stroking of skin | Linear wheals; 2-5% prevalence |
| Cold urticaria | Cold contact/temperature drop | Ice cube test positive; risk of anaphylaxis on swimming |
| Pressure urticaria | Sustained pressure (belts, straps) | Often accompanies CSU |
| Cholinergic urticaria | Sweating, exercise, hot bath | Tiny 1-4 mm wheals with wide flare; common in young |
| Solar urticaria | UV/visible radiation | Minutes after sun exposure |
| Aquagenic urticaria | Water (any temperature) | Distinguished from cold/heat urticaria by temperature independence |
| Vibratory urticaria | Vibratory stimuli | ADGRE2 mutation in familial form |
| Contact urticaria | Skin contact with substance | IgE-mediated or non-immunologic |
- Fitzpatrick's Dermatology, pp. 714-732
Epidemiology
- Lifetime prevalence ~8-20% of the general population
- CSU: prevalence ~0.8% in any given year; women affected ~2x more than men
- Peak age for CSU: 20-40 years (bimodal in children and adults)
- 50% of CSU patients have disease for ≥5 years
Pathophysiology
Urticaria arises from mast cell degranulation in the superficial dermis, releasing histamine, slow-reacting substance of anaphylaxis (leukotrienes), bradykinin, kallikrein, and other mediators. This causes localized vasodilation and increased vascular permeability.
Mechanisms:
- IgE-mediated (immunologic): Classic type I hypersensitivity - food allergens, drugs, insect stings
- Autoimmune: Up to 45% of CSU - IgG autoantibodies against IgE or the α-chain of FcεRI on mast cells; positive autologous serum skin test (ASST)
- Immune complex-mediated: Complement activation, as in urticarial vasculitis and serum sickness
- Non-immunologic direct mast cell release: Opioids, vancomycin, NSAIDs, contrast media, certain foods (strawberries, lobster - histamine release)
- Bradykinin-mediated: ACE inhibitor-induced angioedema, hereditary angioedema (HAE)
- Goldman-Cecil Medicine, p. 4301; Harrison's 22E, p. 2850
Common Triggers / Etiology
Acute urticaria:
- Drugs: Penicillin (most common antibiotic trigger), NSAIDs/aspirin (probably non-immunologic), opioids, ACE inhibitors
- Foods: Seafood, tree nuts, eggs, peanuts; strawberries/lobster (non-immunologic histamine release)
- Infections: Rhinovirus, rotavirus, hepatitis viruses, EBV/mono, coxsackievirus; also candida, dermatophytes, parasites
- Contact: Animal dander/saliva, latex, cosmetics, plants
Chronic urticaria:
-
Autoimmune (most common identifiable cause in CSU)
-
Thyroid disease (anti-thyroid peroxidase / anti-thyroglobulin antibodies, even when euthyroid)
-
Occult infection (H. pylori, dental abscess)
-
Stress and psychological factors (aggravating, not causal)
-
Malignancy (rare; hematologic malignancies have weak association)
-
Rosen's Emergency Medicine, p. 2413; Fitzpatrick's Dermatology, p. 5845
Clinical Features
Wheals (urticaria):
- Pink-to-red, raised, blanching plaques with surrounding erythema ("wheal and flare")
- Any body surface, intensely pruritic (stinging in cholinergic type)
- Individual lesions last <24 h; inducible urticarias <2 h
- Crops of new lesions appear as old ones fade
Angioedema:
- Deeper, asymmetric, non-pitting swelling; more painful than pruritic
- Favors periorbital and perioral regions, tongue, larynx, GI tract
- Laryngeal angioedema is life-threatening
- Takes hours-to-days to resolve
This is what dermatographism looks like on provocation:

Investigations
For acute urticaria, extensive workup is rarely needed. For chronic urticaria, guided investigation is appropriate:
| Test | Indication |
|---|---|
| CBC, ESR/CRP | Baseline; eosinophilia, infection screen |
| Anti-thyroid antibodies (anti-TPO, anti-TG) | Autoimmune thyroid disease association |
| ASST (autologous serum skin test) | Screen for functional IgG autoantibodies (sensitivity ~60-70%) |
| Basophil histamine release assay | More specific for anti-FcεRI/anti-IgE autoantibodies |
| Skin biopsy + DIF | Rule out urticarial vasculitis (if lesions last >24h, leave bruising, or systemic features) |
| C3, C4, CH50 | Suspected urticarial vasculitis or HAE |
| Serum IgE, specific IgE RAST | If allergic trigger suspected |
| Provocation tests | For each inducible subtype (ice cube test, dermographometer, etc.) |
- Fitzpatrick's Dermatology, p. 5996
Differential Diagnosis
- Urticarial vasculitis (lesions last >24h, leave purpura/bruise)
- Bullous pemphigoid (urticarial phase)
- Erythema multiforme
- Contact dermatitis
- Mastocytosis / urticaria pigmentosa
- Angioedema from ACE inhibitors / HAE (bradykinin-mediated - does NOT respond to antihistamines)
- Adult-onset Still disease
- Schnitzler syndrome
- Polymorphic eruption of pregnancy
Treatment
General Principles
- Identify and eliminate triggers
- Avoid NSAIDs and aspirin (can worsen most urticaria types)
- Note: bradykinin-mediated angioedema (HAE, ACE inhibitor) does NOT respond to antihistamines or steroids - requires specific therapy (C1-INH, icatibant, ecallantide)
EAACI/AAAAI Stepwise Algorithm for Chronic Urticaria
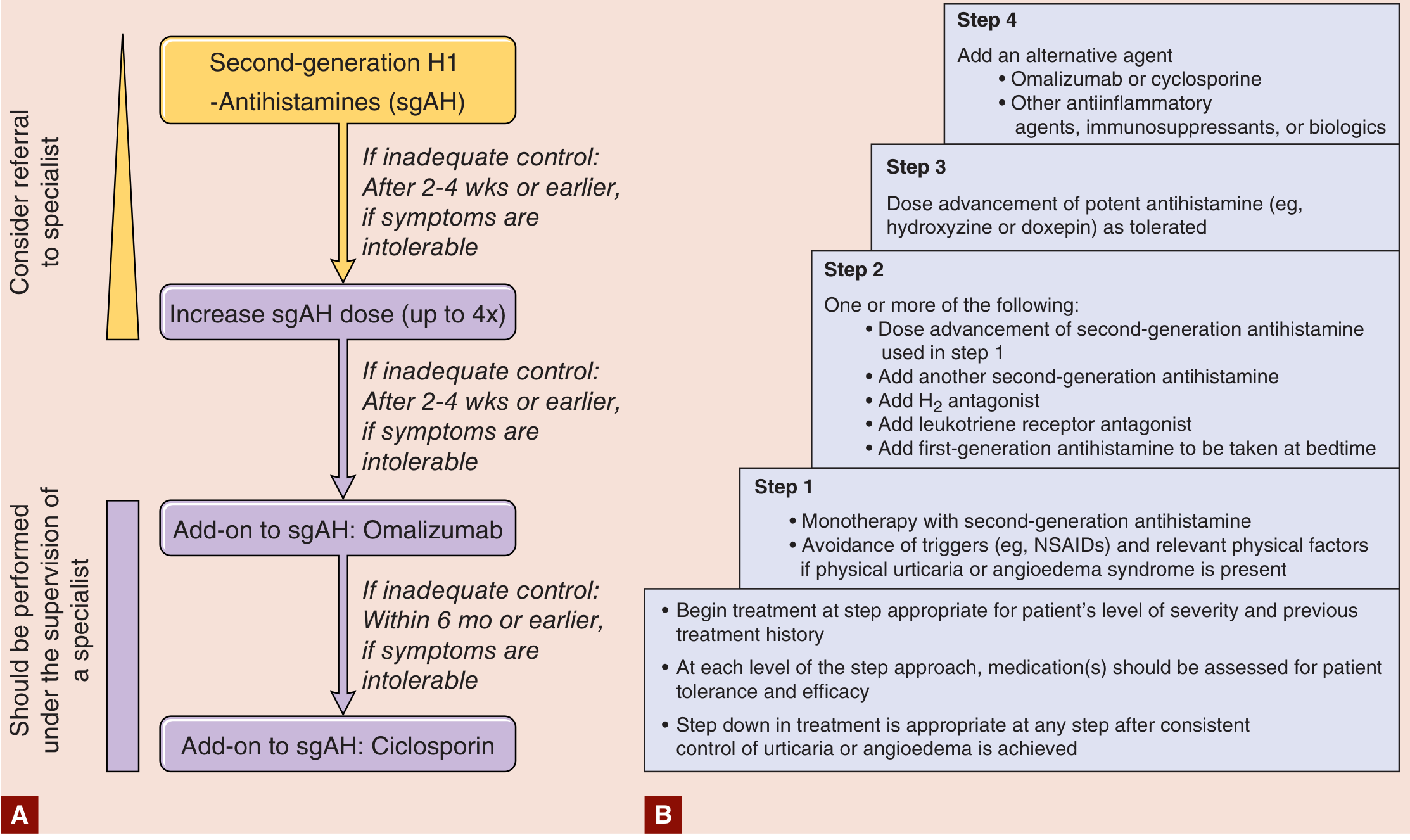
| Step | Treatment |
|---|---|
| Step 1 | Second-generation H1-antihistamine (sgAH) monotherapy (cetirizine, loratadine, fexofenadine, bilastine) + trigger avoidance |
| Step 2 (if inadequate at 2-4 weeks) | Up-dose sgAH up to 4x standard dose; add H2 antagonist; add leukotriene receptor antagonist; add first-generation AH at bedtime |
| Step 3 | Add potent antihistamine (hydroxyzine or doxepin) as tolerated |
| Step 4 | Add omalizumab (anti-IgE biologic, 300 mg SC monthly) or cyclosporin |
Omalizumab is highly effective for antihistamine-refractory CSU. A 2025 systematic review and meta-analysis confirms its safety and efficacy in pediatric CSU as well (PMID 40545961).
A 2024 systematic review (PMID 38420865) of acute urticaria treatment confirms the priority of antihistamines with epinephrine reserved for anaphylactic presentations.
Systemic corticosteroids: Generally avoided long-term for idiopathic urticaria due to toxicity. Indicated short-term for severe exacerbations, pressure urticaria, urticarial vasculitis, or debilitating disease refractory to antihistamines.
Refractory/specialty cases:
-
Urticarial vasculitis: hydroxychloroquine, dapsone, colchicine ± steroids
-
HAE: acute attacks - icatibant (bradykinin-2 receptor antagonist), ecallantide (kallikrein inhibitor), purified C1-INH or fresh frozen plasma; prophylaxis - lanadelumab, C1-INH, attenuated androgens
-
Other refractory options: methotrexate, tacrolimus, IV immunoglobulin, plasmapheresis, narrow-band UVB
-
Fitzpatrick's Dermatology, p. 732; Harrison's 22E, pp. 2851-2854; Goldman-Cecil Medicine, p. 4302
Key Points to Remember
- Urticaria = superficial dermis; angioedema = deep dermis/subcutaneous; ~40% have both
- Chronic = ≥6 weeks; CSU is most common chronic form and is often autoimmune
- Individual wheals lasting >24h, with bruising or systemic signs → biopsy to rule out urticarial vasculitis
- ACE inhibitor / HAE angioedema is bradykinin-mediated → antihistamines and epinephrine are ineffective → needs C1-INH or icatibant
- Stepwise treatment: sgAH → up-dose → add omalizumab → add cyclosporin
- NSAIDs worsen urticaria in most patients and should be avoided
This is a shared conversation. Sign in to Orris to start your own chat.