Most common ecg in medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have excellent textbook content to give a thorough, well-structured answer. Here is the comprehensive guide:
Most Common ECGs in Clinical Medicine
ECG interpretation follows a systematic approach: rate → rhythm → axis → intervals → waveform morphology. Below are the most important and commonly encountered ECG patterns, grouped by category.
1. Normal Sinus Rhythm (Baseline Reference)
- Rate: 60-100 bpm
- Regular R-R intervals
- P wave before every QRS, PR interval 120-200 ms, QRS < 120 ms
- The P wave = atrial depolarization; QRS = ventricular depolarization; T wave = ventricular repolarization
How to read rate (quick method): Count large boxes between R waves - divide 300 by that number. Example: 4 large boxes = 75 bpm.
- Medical Physiology, Box 21-2
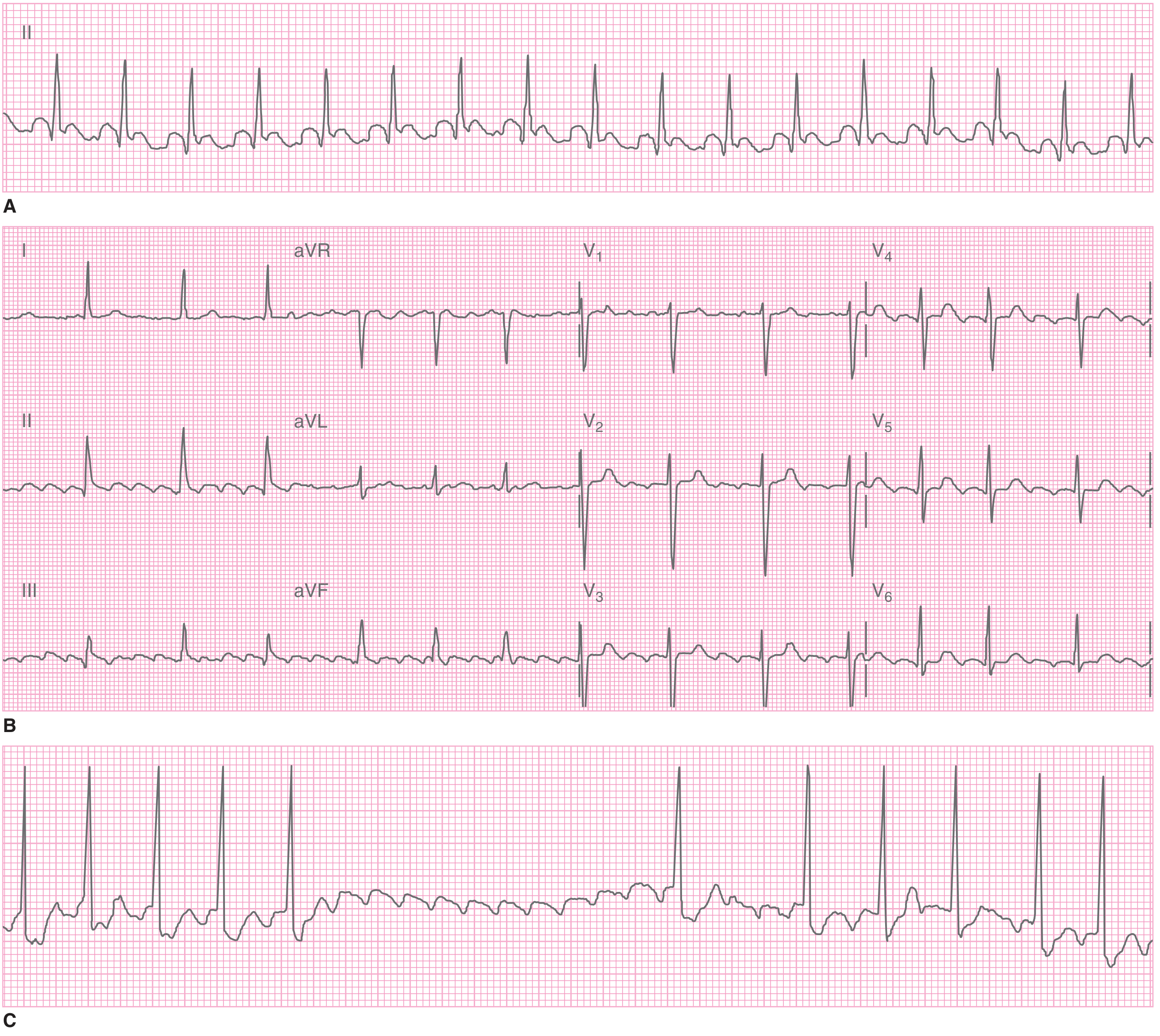
2. Atrial Fibrillation (AF) - Most Common Sustained Arrhythmia
Classic ECG features:
- Absent P waves - flat or chaotic/fibrillatory baseline
- Irregularly irregular ventricular rhythm (no two R-R intervals the same)
- Narrow QRS (unless pre-existing bundle branch block or pre-excitation)
Causes: Ischemic heart disease, valvular disease, cardiomyopathy, thyrotoxicosis, alcohol ("holiday heart"), blunt chest trauma.
Clinical risk: Loss of atrial kick → heart failure. Risk of thromboembolism increases with duration; >48 hours requires anticoagulation before cardioversion.
- Tintinalli's Emergency Medicine, Table 18-8
3. STEMI (ST-Elevation Myocardial Infarction)
Per the Fourth Universal Definition of MI, diagnostic STEMI criteria:
| Lead | Threshold |
|---|---|
| All leads except V2-V3 | New ST elevation ≥ 1 mm in ≥2 contiguous leads |
| V2-V3, females (any age) | ≥ 1.5 mm |
| V2-V3, males < 40 years | ≥ 2.5 mm |
| V2-V3, males ≥ 40 years | ≥ 2.0 mm |
Evolutionary sequence:
- Hyperacute T waves - tall, broad-based, peaked (within minutes of occlusion; transient)
- ST elevation - "tombstoning" pattern
- Q wave formation - pathological Q waves develop (>40 ms wide or >25% of R wave height)
- T wave inversion - during and after infarction
- ST normalization - hours to days later
Localization by leads:
- Inferior MI (RCA): II, III, aVF - reciprocal changes in I, aVL
- Anterior MI (LAD): V1-V4
- Lateral MI (LCx): I, aVL, V5-V6
- Posterior MI (RCA/LCx): ST depression V1-V3 + tall R waves (mirror image)
Important: ST elevation establishes candidacy for emergent reperfusion (PCI or fibrinolysis). A single normal ECG does not rule out AMI - serial ECGs are required.
- Rosen's Emergency Medicine, Chapter 64
4. NSTEMI / Unstable Angina ECG Findings
- ST depression (horizontal or downsloping ≥ 0.5 mm)
- T-wave inversions (deep symmetric inversions = Wellens pattern in LAD disease)
- May have a normal ECG (up to 6% of MIs)
- Troponin distinguishes NSTEMI from unstable angina
5. Left Bundle Branch Block (LBBB)
- QRS ≥ 120 ms (broad)
- Broad notched R in I, aVL, V5, V6 ("M" shape or plateau)
- Deep S or QS in V1 (rS or QS pattern)
- ST and T wave changes discordant (opposite) to the main QRS deflection
- New LBBB + chest pain = treat as STEMI equivalent (Sgarbossa criteria)
6. Right Bundle Branch Block (RBBB)
- QRS ≥ 120 ms
- RSR' pattern ("rabbit ears") in V1-V2
- Wide S wave in I, V5, V6
- Common in pulmonary embolism, right heart strain, congenital disease, or incidental finding
7. Left Ventricular Hypertrophy (LVH)
Sokolow-Lyon criteria (most used):
- S in V1 + R in V5 or V6 ≥ 35 mm
- R in aVL ≥ 11 mm
Associated findings:
- "Strain pattern" - ST depression + asymmetric T-wave inversion in lateral leads (I, aVL, V5, V6)
- Left axis deviation
- Increased QRS duration
Common in hypertension, aortic stenosis, hypertrophic cardiomyopathy.
8. AV Blocks
| Type | PR interval | Dropped beats | QRS |
|---|---|---|---|
| 1st degree | >200 ms, constant | None | Normal |
| 2nd degree Mobitz I (Wenckebach) | Progressively lengthens | Yes, then resets | Normal |
| 2nd degree Mobitz II | Fixed PR interval | Sudden drop (no warning) | Often wide |
| 3rd degree (complete) | No relationship (AV dissociation) | All P waves blocked | Wide escape |
- Mobitz II and 3rd degree = serious, often require pacing
- Symptom to Diagnosis, Chapter on Bradycardia
9. Ventricular Tachycardia (VT) vs. SVT with Aberrancy
VT features:
- Wide QRS (≥ 120 ms), rate 100-250 bpm
- AV dissociation (P waves independent of QRS) - pathognomonic
- Fusion beats and capture beats (pathognomonic)
- Brugada algorithm helps differentiate from SVT with aberrancy
VF: Completely chaotic, no discernible QRS - cardiac emergency.
10. Other High-Yield Patterns
| Pattern | Key ECG Finding | Cause |
|---|---|---|
| Hyperkalemia | Peaked T waves → wide QRS → sine wave | Renal failure, ACE inhibitors |
| Hypokalemia | Flattened T waves, prominent U waves, QU prolongation | GI losses, diuretics |
| Pulmonary embolism | S1Q3T3 (S wave in I, Q wave + T inversion in III), sinus tachycardia, new RBBB | Large/submassive PE |
| Pericarditis | Diffuse saddle-shaped ST elevation, PR depression (all leads except aVR/V1) | Viral, autoimmune |
| Brugada syndrome | Coved-type ST elevation in V1-V2, RBBB morphology | Channelopathy, sudden death risk |
| Wolff-Parkinson-White (WPW) | Short PR, delta wave, wide QRS | Accessory pathway |
| Long QT | QTc > 450 ms (males), > 470 ms (females) | Drugs (amiodarone, antipsychotics), electrolyte abnormalities, congenital |
| Early repolarization | ST elevation with J-point notching in young athletes | Usually benign variant |
| Digoxin toxicity | "Reverse tick" ST scooping (Salvador Dali mustache), PVCs, bidirectional VT | Digoxin excess |
Quick Systematic ECG Reading Approach
- Rate - 300 / (number of large boxes between R-R)
- Rhythm - regular? P before every QRS?
- Axis - I and aVF both positive = normal axis
- Intervals - PR (120-200 ms), QRS (<120 ms), QTc (<450 ms males / <470 ms females)
- P wave - present, morphology, relationship to QRS
- QRS - width, morphology, Q waves
- ST segment - elevation or depression
- T waves - inversion, hyperacuity
- U waves - if present, think hypokalemia
- Medical Physiology, Box 21-2 & Table 21-5
- Rosen's Emergency Medicine
- Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.