Define total TIVA . Mention varies agents used in clinical practise for MD anaesthesia exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a thorough MD exam answer. Here is the full response:
Total Intravenous Anaesthesia (TIVA) - MD Anaesthesia Examination Answer
Definition
Total Intravenous Anaesthesia (TIVA) is a technique of general anaesthesia in which all anaesthetic agents - hypnotics, analgesics, and muscle relaxants - are administered exclusively by the intravenous route, with no use of any inhalational agent (including nitrous oxide) for induction or maintenance.
The three essential components of anaesthesia (the anaesthetic "triad") are all delivered IV:
- Hypnosis/Unconsciousness - e.g., propofol
- Analgesia - e.g., remifentanil, fentanyl
- Muscle relaxation - e.g., rocuronium, vecuronium
TIVA differs from partial IV anaesthesia (PIVA) where IV agents are combined with volatiles. In "pure TIVA," no volatile agent is used at any stage.
Pharmacokinetic Basis of TIVA
Three-Compartment Model
IV anaesthetics follow a three-compartment model:
- Central compartment (plasma/blood) - rapid initial distribution
- Peripheral compartment 1 (rapidly equilibrating tissues)
- Peripheral compartment 2 (slowly equilibrating tissues - fat, muscle)
On stopping infusion, drug returns from peripheral compartments back to the central compartment, prolonging the time to awakening.
Context-Sensitive Half-Time (CSHT)
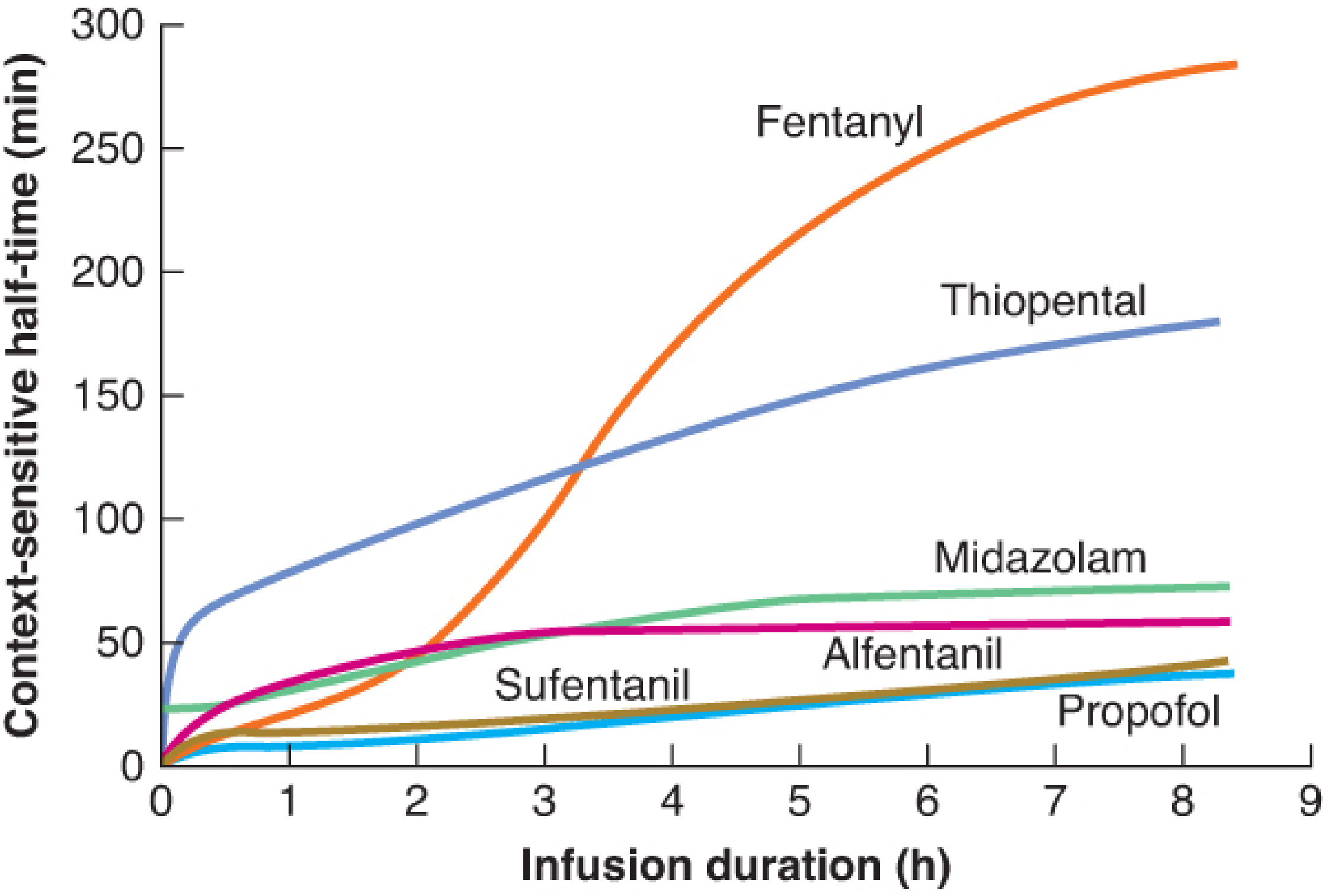
This is the key concept in TIVA pharmacokinetics. CSHT is defined as the time required for plasma concentration to decrease by 50% after stopping a continuous infusion of a specific duration. The "context" refers to the duration of infusion.
Key clinical implications:
- Propofol - CSHT remains low (~30-40 min) even after prolonged infusions. Rapid hepatic clearance prevents peripheral drug from re-accumulating in plasma.
- Remifentanil - CSHT is ~3-4 min regardless of infusion duration (metabolized by non-specific plasma esterases; essentially a flat line).
- Fentanyl - CSHT rises steeply after >2 hours; becomes unpractical for pure TIVA.
- Thiopental - CSHT rises rapidly; NOT suitable for maintenance infusions.
Target Controlled Infusion (TCI)
TCI is the delivery method that makes TIVA clinically practical. A computer-controlled syringe pump uses population pharmacokinetic models to calculate infusion rates that achieve and maintain a target plasma (Cp) or effect-site (Ce) concentration.
- Propofol uses the Marsh model (plasma target) or Schneider model (effect-site target)
- Remifentanil uses the Minto model (accounts for age, weight, and height)
Advantages of TIVA
| Advantage | Mechanism |
|---|---|
| Reduced PONV | Propofol has antiemetic properties |
| No atmospheric pollution | No volatile agent scavenging needed |
| Better haemodynamic stability | Titratable depth |
| Useful in MH-susceptible patients | No trigger agents |
| Improved intraoperative conditions | Especially in ENT/airway/laser surgery |
| Rapid predictable recovery | Low CSHT of propofol + remifentanil |
| Reduces coughing on emergence | Propofol blunts airway reflexes |
| Suitable during TIVA for nerve monitoring | No neuromuscular blocking needed with remifentanil |
Indications for TIVA
- Neurosurgery (reduces ICP, CMRO2)
- Airway laser surgery (no inflammable vapours)
- During cardiopulmonary bypass
- Day case/ambulatory anaesthesia
- ENT, head & neck, microlaryngoscopy
- Patients prone to PONV (bariatric, GI surgery)
- Malignant hyperthermia susceptible patients
- Robotic and laparoscopic surgery
- Total ear surgery (nerve monitoring)
Disadvantages / Risks
- Small but real risk of awareness (no end-tidal agent monitor as backup - depth must be monitored with BIS/entropy)
- Pain on IV injection (propofol)
- Propofol infusion syndrome (prolonged high doses in ICU/children)
- IV access dependency - pump failure or disconnection = awareness
- No muscle relaxation reversal provided by the hypnotic
Agents Used in Clinical Practice for TIVA
A. HYPNOTIC AGENTS
1. Propofol (2,6-di-isopropyl phenol) - THE CORNERSTONE OF TIVA
Mechanism: Potentiation of GABA-A receptor chloride channels
Pharmacokinetics:
- Onset: 30-60 seconds
- Large volume of distribution (Vd)
- Hepatic clearance: ~1.5-2.0 L/min (exceeds hepatic blood flow - extrahepatic clearance also occurs)
- Context-sensitive half-time: low and flat - ideal for infusion
- Recovery is rapid even after prolonged infusions due to rapid redistribution
Doses:
| Use | Dose |
|---|---|
| Induction (adult) | 1-2.5 mg/kg IV |
| Maintenance infusion | 4-12 mg/kg/hr (66-200 mcg/kg/min) |
| TCI target (plasma) | 3-6 mcg/mL |
| Sedation infusion | 1-4 mg/kg/hr |
Advantages:
- Anti-emetic (reduces PONV)
- Smooth, rapid induction
- Blunts laryngeal reflexes - useful in airway procedures
- Low CSHT - predictable recovery
- Reduces ICP, CMRO2
Disadvantages:
- Pain on injection (mitigated by IV lidocaine or opioid pre-treatment, large vein)
- Hypotension (vasodilation + myocardial depression), especially with hypovolaemia/elderly
- Apnoea
- Propofol Infusion Syndrome (PRIS): metabolic acidosis, rhabdomyolysis, cardiac dysrhythmias - with prolonged doses >4 mg/kg/hr
Bailey & Love 28e; Barash 9e; Scott-Brown Vol 1
2. Ketamine (phencyclidine derivative)
Mechanism: Non-competitive NMDA receptor antagonist. Also acts on opioid receptors, muscarinic receptors, and sodium/calcium channels.
Produces "dissociative anaesthesia" - a cataleptic state with profound analgesia, amnesia, and unconsciousness while maintaining most reflexes.
Pharmacokinetics:
- Onset (IV): 30-60 seconds
- Duration: 10-15 minutes (bolus)
- Hepatic metabolism (CYP3A4) to active metabolite norketamine
- Redistribution governs offset after single dose
Doses:
| Use | Dose |
|---|---|
| IV induction | 1-2 mg/kg |
| IM induction | 4-8 mg/kg |
| Oral premedication (paed) | 3-6 mg/kg |
| Intranasal (paed) | 3-6 mg/kg |
| Subanesthetic IV infusion | 0.2-0.5 mg/kg/hr |
Advantages:
- Preserves airway reflexes and respiratory drive
- Bronchodilator - ideal in asthma, reactive airway
- Maintains blood pressure - ideal in haemodynamically compromised patients and field anaesthesia
- Excellent analgesia (opioid-sparing)
- Multiple routes of administration
Disadvantages:
- Emergence delirium/hallucinations (mitigated by concurrent benzodiazepine)
- Increases secretions (sialorrhoea) - give anticholinergic pre-treatment
- Raises ICP, IOP - use caution in head injury, glaucoma
- Dysphoria, unpleasant dreams
Bailey & Love 28e; Cummings Otolaryngology
3. Etomidate (imidazole / steroid derivative)
Mechanism: GABA-A receptor agonist
Key feature: Minimal cardiovascular depression - agent of choice in haemodynamically unstable patients
Pharmacokinetics:
- Onset: 30-60 seconds
- Duration: 3-5 minutes
- Metabolism: ester hydrolysis (plasma + hepatic esterases)
- Rapid, predictable offset
Doses:
| Use | Dose |
|---|---|
| IV induction (adult) | 0.2-0.3 mg/kg |
| Paediatric induction | 0.2-0.3 mg/kg |
Advantages:
- Excellent haemodynamic stability (no change in CO, HR, BP)
- Reduces CMRO2, ICP - useful in neuroanaesthesia
- Brief duration
Disadvantages:
- Adrenocortical suppression - inhibits 11-beta-hydroxylase. Even a single induction dose suppresses cortisol for 6-8 hours; avoid in septic shock, repeated doses, ICU infusions
- Pain on injection
- Myoclonus
- PONV
- NOT used for maintenance infusion in clinical practice (adrenal suppression)
Bailey & Love 28e; Cummings Otolaryngology
4. Thiopentone / Thiopental (barbiturate)
Mechanism: GABA-A receptor potentiation + AMPA/kainate receptor inhibition
Doses:
| Use | Dose |
|---|---|
| IV induction (adult) | 3-5 mg/kg |
| Neonate | 3-4 mg/kg |
Advantages:
- Rapid, smooth induction
- Reduces CMRO2 and ICP (historic use in neuroanaesthesia)
- Anticonvulsant
Disadvantages:
- Significant myocardial depression, vasodilation - hypotension
- High CSHT after prolonged infusions (NOT suitable for TIVA maintenance)
- Porphyria precipitant (absolute contraindication)
- No analgesic properties
- Accumulates in fat with prolonged dosing - "hung-over" recovery
Largely replaced by propofol. Thiopentone is unsuitable as a TIVA maintenance agent due to its high and rising CSHT.
5. Midazolam (benzodiazepine)
Mechanism: GABA-A receptor positive allosteric modulator
Role in TIVA: Used as an adjunct/co-induction agent; not a sole hypnotic for TIVA but reduces propofol requirements and provides amnesia.
Doses:
| Use | Dose |
|---|---|
| Premedication (oral) | 0.3-0.5 mg/kg (paed) |
| IV co-induction | 0.03-0.05 mg/kg |
| Sedation infusion | 0.02-0.1 mg/kg/hr |
Notes: Rising CSHT with prolonged infusion (see graph above). Active metabolite 1-OH-midazolam accumulates in renal failure.
6. Dexmedetomidine (alpha-2 agonist)
Mechanism: Highly selective alpha-2 adrenoceptor agonist (8x more selective than clonidine). Acts at locus coeruleus to produce "rousable sedation"
Key property: Sedation with cooperative, rousable patient - does not cause respiratory depression
Doses:
| Use | Dose |
|---|---|
| Loading dose | 0.5-1 mcg/kg over 10-20 min |
| Maintenance infusion | 0.2-0.7 mcg/kg/hr |
Indications in TIVA context:
- Awake fibre-optic intubation
- ICU sedation
- Adjunct in TIVA - reduces propofol and opioid requirements
- Procedural sedation
Advantages:
- No respiratory depression
- Analgesic and sympatholytic
- Reduces emergence delirium (especially in children)
- Prevents opioid-induced hyperalgesia
Disadvantages:
- Bradycardia, hypotension (especially loading dose)
- Not approved for prolonged use in children
B. OPIOID ANALGESIC AGENTS IN TIVA
1. Remifentanil - THE IDEAL TIVA OPIOID
Mechanism: Mu-opioid receptor agonist
Unique pharmacokinetics:
- Metabolized by non-specific tissue and plasma esterases (ester linkage in its structure)
- Elimination half-time: ~6 minutes
- Context-sensitive half-time: 3-4 minutes - independent of infusion duration (flat line on CSHT graph)
- Not dependent on hepatic/renal function
Doses:
| Use | Dose |
|---|---|
| TCI (plasma target) | 2-8 ng/mL |
| Infusion (maintenance) | 0.05-2 mcg/kg/min |
| Awake fibre-optic intubation | 0.025-0.1 mcg/kg/min |
Advantages:
- Predictable rapid offset regardless of infusion length
- No active metabolites
- Deep intraoperative analgesia achievable with rapid reversal
- Eliminates need for NMBDs in some cases (useful for nerve monitoring)
- Improves intraoperative cardiovascular stability
Disadvantages:
- Very short duration - post-operative analgesia MUST be planned and given before emergence (switch to longer acting opioid or regional technique)
- Bradycardia, chest wall rigidity at high doses
- Muscle rigidity with rapid injection
- Opioid-induced hyperalgesia with prolonged infusion
- Cost
Scott-Brown Vol 1; Bailey & Love 28e
2. Fentanyl
Mechanism: Mu-opioid receptor agonist (synthetic)
- Highly lipophilic; rapid onset
- CSHT rises dramatically after >2 hours of infusion (see graph)
- Used as bolus dosing during TIVA rather than continuous infusion for cases >2 hours
Doses:
| Use | Dose |
|---|---|
| Intraoperative bolus | 1-3 mcg/kg |
| Infusion | 1-3 mcg/kg/hr |
3. Alfentanil
- Shorter-acting than fentanyl; lower CSHT than fentanyl
- Less lipophilic than fentanyl - smaller Vd
- Useful for short procedures as bolus or brief infusion
- Used before intubation, laryngoscopy: 10-20 mcg/kg
4. Sufentanil
- 5-10x more potent than fentanyl
- Moderate CSHT - less accumulation than fentanyl for infusions up to ~8 hours
- Used in cardiac anaesthesia
5. Morphine
- Used as part of multi-modal analgesia alongside TIVA
- Long CSHT, active metabolite (M6G) accumulates in renal failure
- Not ideal for continuous infusion as primary TIVA opioid
C. MUSCLE RELAXANTS (as part of total IV technique)
Though not strictly "hypnotics," muscle relaxants complete the TIVA triad:
| Agent | Class | Onset | Duration | Notes |
|---|---|---|---|---|
| Suxamethonium | Depolarizing | 60 sec | 5-10 min | RSI; metabolized by plasma cholinesterase |
| Rocuronium | Non-depolarizing | 90 sec | 30-45 min | Reversible with sugammadex; can be used in RSI at 1.2 mg/kg |
| Vecuronium | Non-depolarizing | 2-3 min | 25-40 min | Standard relaxant |
| Atracurium | Non-depolarizing | 2-3 min | 25-35 min | Hofmann elimination - useful in renal/hepatic failure |
| Cisatracurium | Non-depolarizing | 3-5 min | 40-60 min | Fewer histamine release; preferred in ICU |
| Mivacurium | Non-depolarizing | 2-3 min | 12-20 min | Shortest non-depolarizing; metabolized by plasma ChE |
Summary Table - Key Agents in TIVA
| Agent | Class | Primary Role | Key Feature |
|---|---|---|---|
| Propofol | Alkylphenol | Induction + Maintenance | Low CSHT; anti-emetic; cornerstone of TIVA |
| Remifentanil | Opioid | Analgesia (infusion) | Flat CSHT; esterase metabolism |
| Ketamine | NMDA antagonist | Dissociative hypnotic/analgesic | Haemodynamic preservation; bronchodilator |
| Etomidate | Imidazole | Induction only | Cardiac stability; adrenal suppression |
| Midazolam | Benzodiazepine | Adjunct/co-induction | Amnesia; rising CSHT |
| Dexmedetomidine | Alpha-2 agonist | Sedation adjunct | No respiratory depression; rousable |
| Fentanyl | Opioid | Short-term analgesia | Rising CSHT after 2h |
| Alfentanil | Opioid | Short procedures | Lower CSHT than fentanyl |
| Thiopentone | Barbiturate | Induction only | RSI; neuroanaesthesia; porphyria CI |
TCI Models (Exam Favourite)
| Drug | PK Model | Target |
|---|---|---|
| Propofol | Marsh / Schneider | Plasma Cp or Effect-site Ce |
| Remifentanil | Minto | Effect-site Ce |
| Alfentanil | Maitre | Plasma Cp |
Clinical Settings Where TIVA is the Preferred Choice
- Neurosurgery - reduces ICP + CMRO2
- Laser airway surgery - no fire risk from volatiles
- Cardiopulmonary bypass - prevents volatile delivery interruption
- ENT/microscopic ear surgery - facial nerve monitoring (remifentanil avoids NMBDs)
- Day case surgery - rapid, clear-headed recovery
- Malignant hyperthermia susceptibility - no triggers
- PONV-prone patients (bariatric, gynaecology)
- Thyroid + parathyroid surgery - reduced coughing on emergence
Sources: Bailey & Love's Short Practice of Surgery 28e | Barash, Cullen & Stoelting's Clinical Anesthesia 9e | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1 | Cummings Otolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.