
cd5226e0-493b-4a86-b0cc-766b311dcd52.jpeg
Interpret
analyse_media
Reading File
Here is a full interpretation of this Arterial Blood Gas (ABG) report:
ABG Interpretation - Patient: SATALING
Sample: Arterial | GEM 3500 analyzer | 14/07/2026 at 16:46
Step 1: Raw Values vs. Normal Ranges
| Parameter | Result | Normal Range | Status |
|---|---|---|---|
| pH | 7.56 | 7.35 - 7.45 | 🔴 HIGH (Alkalosis) |
| pCO2 | 37 mmHg | 35 - 45 mmHg | ✅ Normal |
| pO2 | 68 mmHg | 80 - 100 mmHg | 🔴 LOW (Hypoxemia) |
| Na+ | 134 mmol/L | 135 - 145 mmol/L | ⚠️ Slightly low |
| K+ | 3.5 mmol/L | 3.5 - 5.0 mmol/L | ✅ Low-normal |
| Ca++ (ionized) | 0.98 mmol/L | 1.12 - 1.32 mmol/L | 🔴 LOW (Hypocalcemia) |
| Ca++ (pH 7.4 corrected) | 1.05 mmol/L | 1.12 - 1.32 mmol/L | 🔴 Still LOW |
| Glucose | 177 mg/dL | 70 - 140 mg/dL | 🔴 HIGH (Hyperglycemia) |
| Lactate | 0.8 mmol/L | 0.5 - 2.0 mmol/L | ✅ Normal |
| Hematocrit | 37% | 36-48% (F), 41-53% (M) | ✅ Normal/low-normal |
| HCO3- | 33.1 mmol/L | 22 - 26 mmol/L | 🔴 HIGH |
| Base Excess (ecf) | +10.9 mmol/L | -2 to +2 mmol/L | 🔴 HIGH |
| SO2c | 96% | ≥95% | ✅ Normal |
| THbc (Hemoglobin) | 11.5 g/dL | 12-17 g/dL | ⚠️ Mild anemia |
Step 2: Primary Disorder
- pH 7.56 → Alkalosis
- pCO2 37 mmHg → Normal (not the primary driver)
- HCO3- 33.1 mmol/L → Elevated (metabolic driver)
Primary Diagnosis: Metabolic Alkalosis
Step 3: Is There Compensation?
For metabolic alkalosis, the expected respiratory compensation is:
Expected pCO2 = 0.7 × (HCO3- - 24) + 40 = 0.7 × (33.1 - 24) + 40 = 0.7 × 9.1 + 40 = 46.4 mmHg
Measured pCO2 = 37 mmHg, which is significantly lower than the expected 46.4 mmHg.
This means the lungs are hyperventilating more than expected - there is a concurrent primary respiratory alkalosis on top of the metabolic alkalosis.
Step 4: Final Acid-Base Diagnosis
Mixed Disorder: Metabolic Alkalosis + Respiratory Alkalosis
This is a double alkalosis - both processes are simultaneously pushing the pH up, explaining the markedly high pH of 7.56.
Step 5: Oxygenation
- pO2 = 68 mmHg → Mild-to-moderate hypoxemia (normal is >80 mmHg on room air)
- SO2 = 96% → Acceptable saturation, but the pO2 is low
- A-a gradient cannot be calculated (FiO2/PAO2 not available), but hypoxemia is present
The hypoxemia could be driving the respiratory alkalosis (hyperventilation in response to low O2).
Step 6: Clinical Correlations
| Finding | Possible Causes |
|---|---|
| Metabolic alkalosis (HCO3- 33.1, BE +10.9) | Vomiting/NG suction, diuretics, Bartter/Gitelman syndrome, excessive alkali intake, mineralocorticoid excess |
| Respiratory alkalosis (pCO2 37 despite high HCO3-) | Hypoxemia-driven hyperventilation, anxiety, pain, sepsis, hepatic encephalopathy, mechanical over-ventilation, pulmonary embolism |
| Hypoxemia (pO2 68) | Pneumonia, PE, pulmonary edema, ARDS, pleural effusion |
| Ionized hypocalcemia (Ca++ 0.98) | Common in alkalosis (alkalosis increases albumin binding of Ca2+), hypomagnesemia, sepsis, pancreatitis |
| Hyperglycemia (177 mg/dL) | Diabetes, stress hyperglycemia, steroid use |
| Mild anemia (Hgb ~11.5 g/dL) | Chronic disease, blood loss |
| Mild hyponatremia (Na+ 134) | Volume depletion, SIADH, pseudohyponatremia from hyperglycemia |
Summary
This patient has a mixed metabolic + respiratory alkalosis with a markedly elevated pH of 7.56. The most likely scenario is a patient who has an underlying metabolic alkalosis (e.g., from vomiting or diuretics) and is hyperventilating on top of that - possibly driven by the documented hypoxemia (pO2 68 mmHg). The ionized hypocalcemia may be partly artifactual from the alkalosis itself but should be confirmed. The hyperglycemia warrants investigation for diabetes or stress response.
Urgent considerations:
- Identify and treat the cause of hypoxemia (chest X-ray, consider PE workup)
- Correct the metabolic alkalosis (stop precipitating factors, fluid/KCl repletion if volume-depleted)
- Monitor ionized calcium - symptomatic hypocalcemia (tetany, cramps) can occur with alkalosis
- Check serum Mg2+ (hypomagnesemia perpetuates metabolic alkalosis)
cd5226e0-493b-4a86-b0cc-766b311dcd52.jpeg
How should i treat
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a structured, evidence-based treatment plan for this patient's mixed metabolic + respiratory alkalosis with hypoxemia.
Treatment Plan
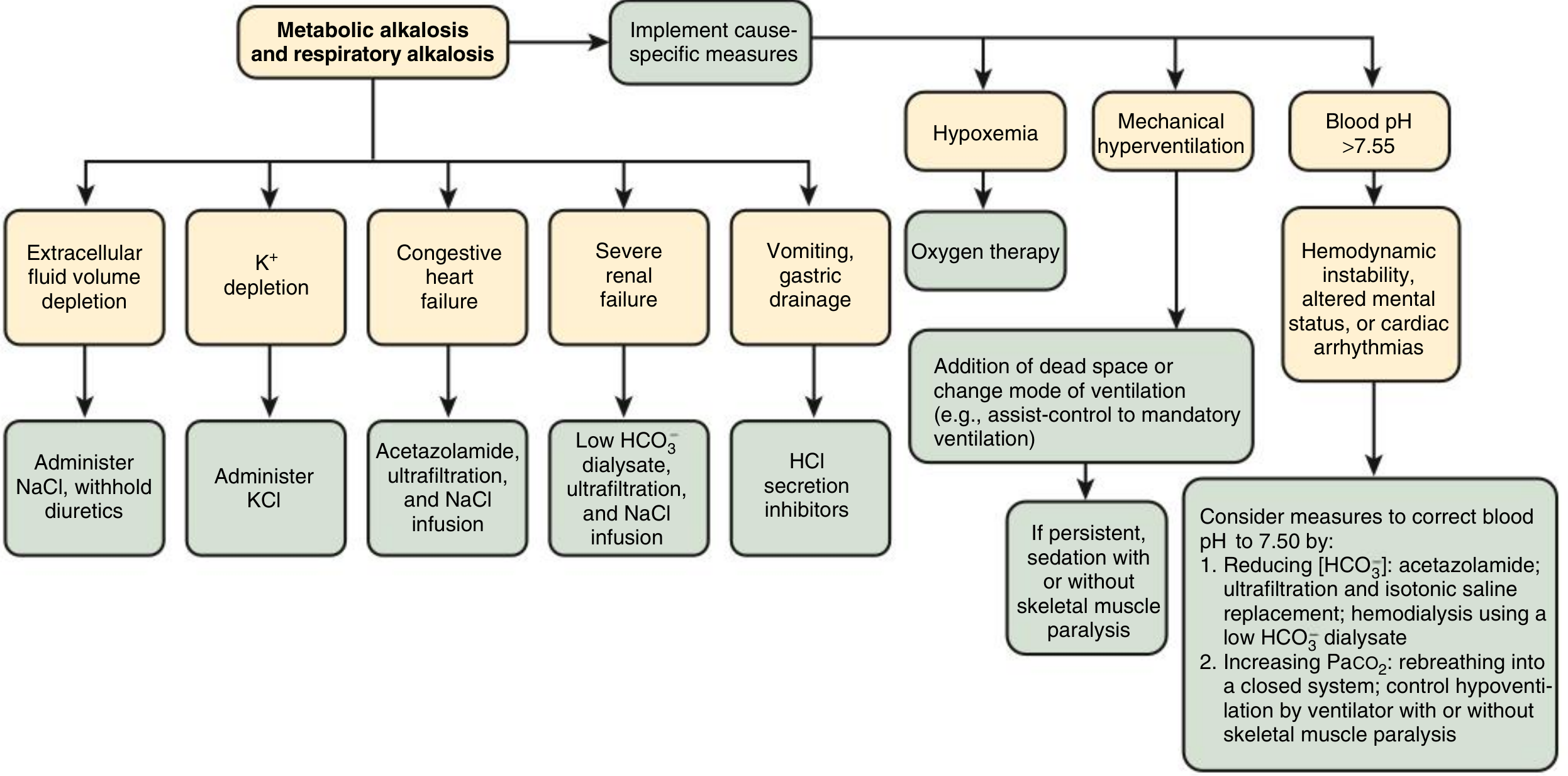
This textbook flowchart directly applies to this patient (Mixed Metabolic + Respiratory Alkalosis):
Priority 1: Treat the Hypoxemia FIRST
pO2 = 68 mmHg - this is the most urgent issue and is likely driving the respiratory alkalosis.
- Start supplemental oxygen to target pO2 >80 mmHg (SpO2 94-98%)
- Investigate the cause of hypoxemia urgently:
- Chest X-ray (pneumonia, pulmonary edema, pleural effusion)
- Consider CT pulmonary angiography if PE is suspected
- ECG, D-dimer, troponin as clinically indicated
- Correcting hypoxemia will reduce the hyperventilation drive, allowing pCO2 to rise and pH to normalize partially
Priority 2: Identify the Cause of Metabolic Alkalosis
Check urine chloride (spot Cl-) - this is the key diagnostic step:
| Urine Cl- | Interpretation | Treatment |
|---|---|---|
| < 25 mmol/L (Chloride-responsive) | Vomiting, NG suction, diuretics, post-hypercapnia | IV Normal Saline (0.9% NaCl) + KCl |
| > 40 mmol/L (Chloride-resistant) | Hyperaldosteronism, Bartter/Gitelman, Cushing's | Treat underlying cause; spironolactone |
Most likely this patient has chloride-responsive alkalosis (most common) - treat accordingly:
Priority 3: Correct the Metabolic Alkalosis
A. Chloride-Responsive (most likely)
- IV isotonic saline (0.9% NaCl) - restores ECV and allows kidneys to excrete excess HCO3-
- Potassium chloride (KCl) - K+ is 3.5 mmol/L (low-normal); replete aggressively as hypokalemia perpetuates metabolic alkalosis. Target K+ > 4.0 mmol/L
- Stop any diuretics if in use
- Proton pump inhibitor (PPI) or H2 blocker if vomiting/NG suction is the cause (to reduce ongoing H+ loss)
B. If patient cannot tolerate saline (e.g., heart failure, fluid overload)
- Acetazolamide 250-500 mg IV - carbonic anhydrase inhibitor, forces kidneys to excrete HCO3-
- Caution: can worsen hypokalemia - always co-administer KCl
- Ultrafiltration if in renal failure
C. If pH > 7.60 with hemodynamic instability or arrhythmias
- Consider dilute HCl (0.1N) infused via central line - reserved for extreme cases only
- Or ammonium chloride (NH4Cl) orally - avoid in liver disease
- Target: bring pH down to ~7.50, not full correction
Priority 4: Treat the Respiratory Alkalosis
- Respiratory alkalosis itself is rarely life-threatening - treating hypoxemia and the metabolic alkalosis is the primary focus
- Do NOT use paper bag rebreathing - dangerous if there is underlying respiratory disease (can worsen hypoxemia)
- If anxiety/pain is contributing: reassurance, anxiolytics (short-acting benzodiazepine), pain control
- If on a ventilator: reduce tidal volume and/or respiratory rate to allow pCO2 to normalize gradually
Priority 5: Correct Associated Abnormalities
| Problem | Action |
|---|---|
| Ionized Ca++ 0.98 (low) | Mostly due to alkalosis binding Ca2+ to albumin - will improve as pH corrects. If symptomatic (tetany, seizures): IV calcium gluconate |
| Glucose 177 mg/dL | Monitor closely; insulin if diabetic or if rising |
| Na+ 134 mmol/L | Mild hyponatremia - will correct with NaCl infusion |
| Hemoglobin ~11.5 g/dL | Mild anemia - investigate cause; transfuse only if symptomatic |
Monitoring
- Repeat ABG in 2-4 hours after initiating treatment
- Urine output and urine electrolytes
- Serum electrolytes (Na, K, Cl, Mg) - check magnesium as hypomagnesemia perpetuates metabolic alkalosis
- Cardiac monitoring (alkalosis increases risk of arrhythmias, especially with hypokalemia)
- Caution: Do not correct pH too rapidly - overshoot into acidosis is dangerous
Bottom line: Start O2, get a chest X-ray and urine chloride, give IV normal saline + KCl, and identify/stop the precipitating cause. The respiratory alkalosis will self-correct once hypoxemia is treated.(Sources: Comprehensive Clinical Nephrology 7e; National Kidney Foundation Primer on Kidney Diseases 8e)
This is a shared conversation. Sign in to Orris to start your own chat.