Anatomy of elbow joint
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from Gray's Anatomy for Students and the Imaging Anatomy Atlas. I have enough to write a thorough, well-illustrated answer.
Anatomy of the Elbow Joint
Overview
The elbow joint is a complex synovial joint involving three separate articulations that share a single common synovial cavity. It functions as both a hinge joint (for flexion/extension) and a pivot joint (for pronation/supination), making it technically a trochoginglymus joint.
Three articulations:
- Humeroulnar joint - trochlear notch of ulna articulates with trochlea of humerus (hinge; primary flexion/extension)
- Humeroradial joint - head of radius articulates with capitulum of humerus (hinge; flexion/extension)
- Proximal radioulnar joint - head of radius articulates with radial notch of ulna (pivot; pronation/supination)
All articular surfaces are covered with hyaline cartilage.
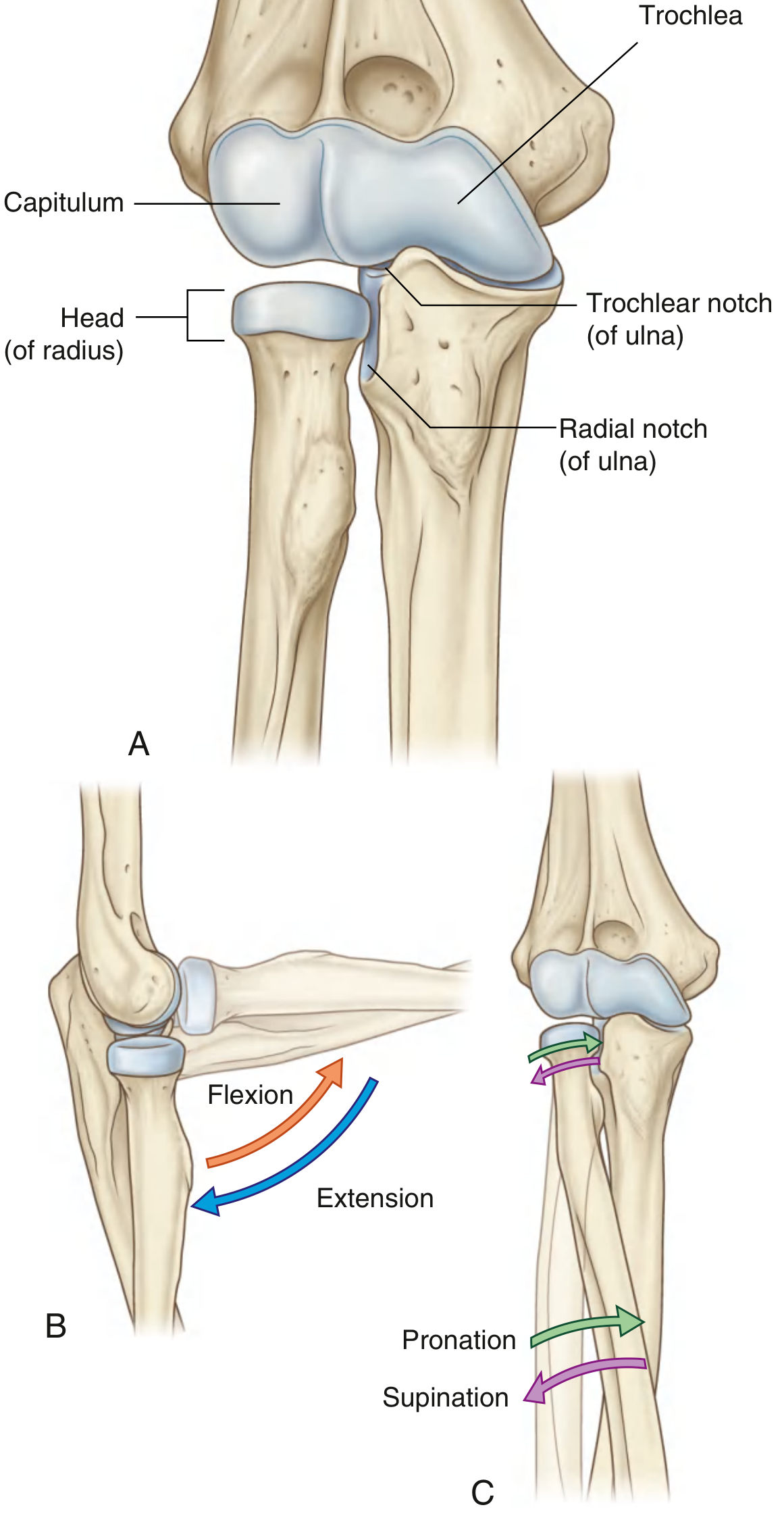
Fig. 7.71 - Elbow joint articulations and movements (Gray's Anatomy for Students)
Bones and Bony Landmarks
Distal Humerus
- Trochlea (medial): pulley-shaped; articulates with the trochlear notch of the ulna; extends anterior to posterior, terminating at the olecranon fossa
- Capitulum (lateral): rounded surface; articulates with the head of the radius
- Medial epicondyle: origin of common flexor muscles; ulnar nerve passes posterior to it
- Lateral epicondyle: origin of common extensor muscles (common extensor tendon)
- Olecranon fossa (posterior): receives olecranon in full extension
- Coronoid fossa (anterior): receives coronoid process in full flexion
- Radial fossa (anterolateral): receives head of radius in full flexion
Proximal Ulna
- Olecranon process: projects posteriorly; inserts triceps tendon; received in olecranon fossa during extension
- Coronoid process: received in coronoid fossa during flexion
- Trochlear notch (semilunar notch): articulates with trochlea of humerus
- Radial notch: articulates with head of radius (proximal radioulnar joint)
- Ulnar tuberosity: attachment for brachialis muscle
Proximal Radius
- Head of radius: disc-shaped; articulates above with capitulum and medially with radial notch of ulna
- Radial tuberosity: attachment for biceps brachii tendon
Bony landmarks: When the elbow is extended, the medial epicondyle, lateral epicondyle, and olecranon tip are in a straight horizontal line (Hueter's line). When the elbow is flexed to 90°, these three points form an equilateral triangle. This relationship is disrupted in fractures and dislocations.
Joint Capsule
The joint is enclosed by a fibrous capsule with two layers:
Fibrous Membrane
- Anteriorly: attaches to the margins of the coronoid and radial fossae on the humerus, and to the coronoid process and neck of the radius
- Posteriorly: attaches to the margins of the olecranon fossa and olecranon
- Medially and laterally: blends with and is reinforced by the collateral ligaments
- On the lateral side, the free inferior margin passes around the neck of the radius (anterior to posterior), allowing rotation
Synovial Membrane
- Lines the deep surface of the fibrous capsule
- Lines the radial fossa, coronoid fossa, olecranon fossa, and the medial surface of the trochlea
- Separated from the fibrous capsule by fat pads overlying the three fossae (coronoid, olecranon, radial)
- These fat pads are displaced by the brachialis and triceps when the fossae receive bony processes during movement
- The sacciform recess is a pocket of synovial membrane that protrudes inferiorly from the free margin of the capsule - it accommodates radial head rotation during pronation/supination
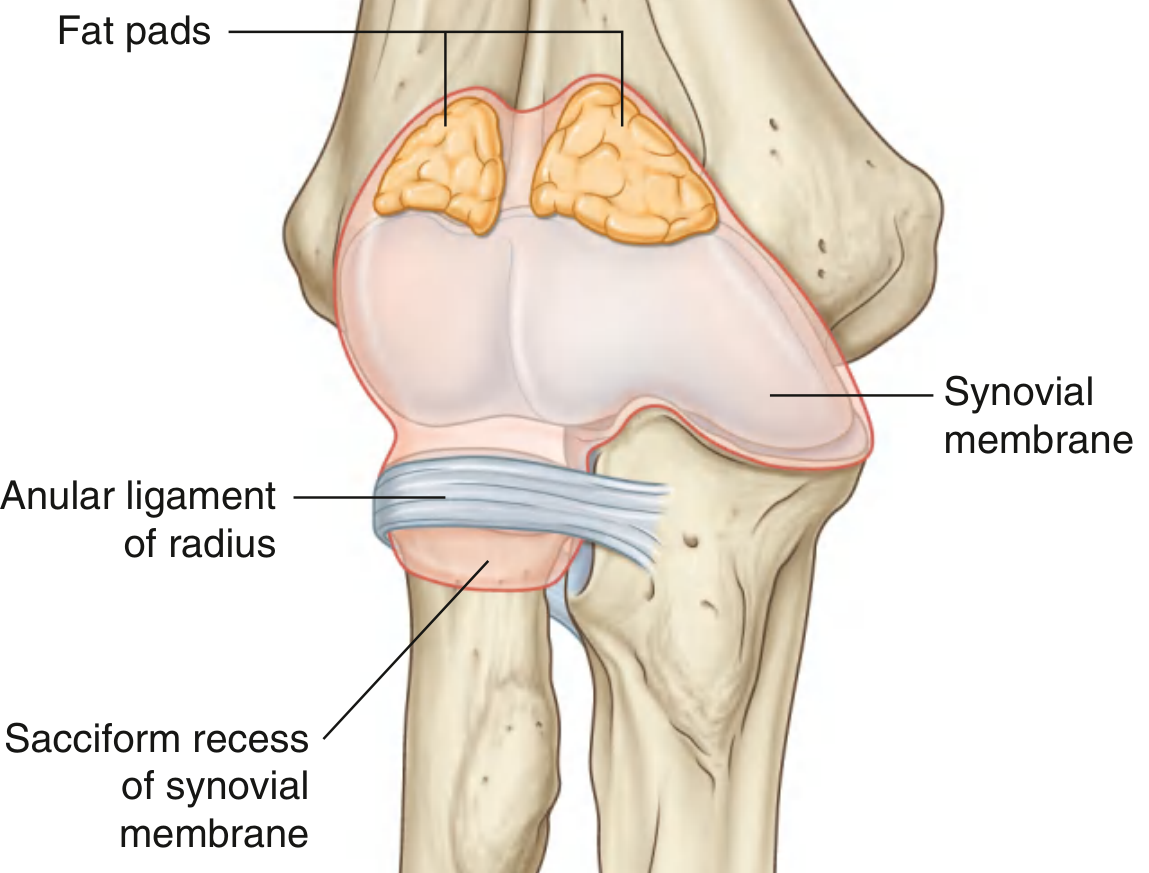
Fig. 7.72 - Synovial membrane of the elbow joint (Gray's Anatomy for Students)
Ligaments
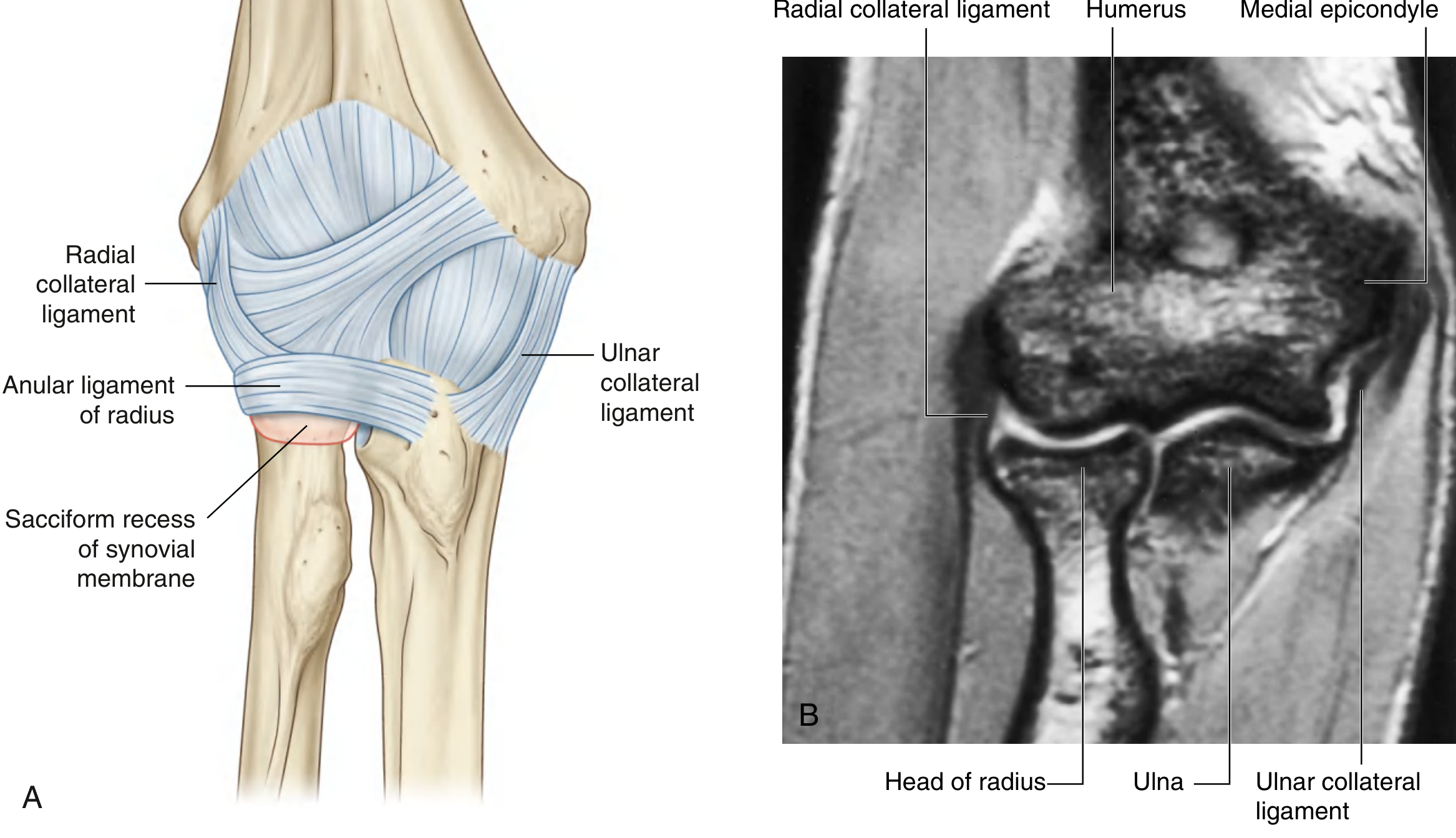
Fig. 7.73 - Elbow joint capsule and ligaments with coronal MRI (Gray's Anatomy for Students)
Medial (Ulnar) Collateral Ligament Complex (UCL)
Comprises three bundles:
- Anterior bundle (most important): arises from the inferior margin of the medial epicondyle, inserts at the sublime tubercle of the ulnar coronoid process. It is the primary static stabilizer against valgus stress and internal rotation. Has an anterior band (taut during extension) and a posterior band (taut during flexion)
- Posterior bundle (Bardinet's ligament): from the posterior aspect of the medial epicondyle to the medial olecranon; forms the floor of the cubital tunnel; provides secondary valgus stability at extremes of flexion
- Transverse bundle (Cooper's ligament): connects olecranon to coronoid; minimal stabilizing function
Lateral Collateral Ligament Complex (LCL)
- Radial collateral ligament (RCL): from the lateral epicondyle, blends into the annular ligament anteriorly
- Annular ligament of the radius: strong ring-shaped ligament encircling the radial head; holds the head of radius against the radial notch of the ulna; blends with the fibrous joint capsule (except posteriorly); the deep surface is lined by cartilage for smooth rotation
- Accessory collateral ligament: assists the annular ligament
- Lateral ulnar collateral ligament (LUCL): lateral epicondyle to the supinator crest of the ulna; primary restraint to posterolateral rotatory instability
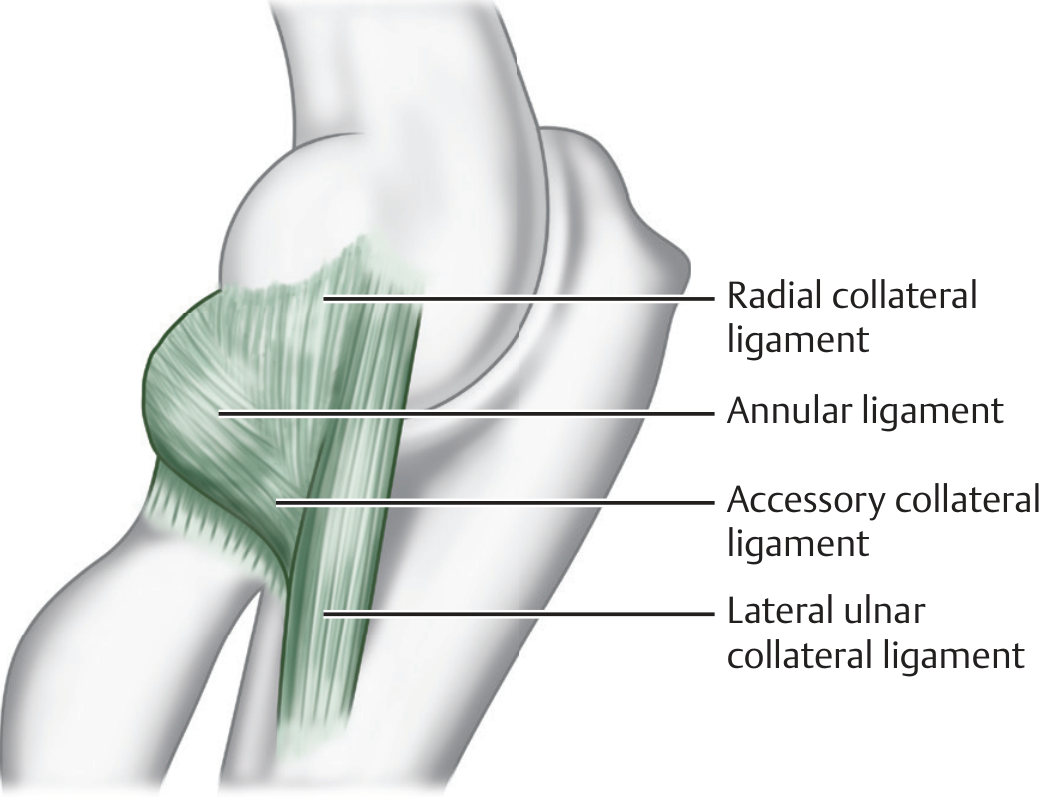
Fig. 16.10 - Lateral collateral ligament complex (Imaging Anatomy: Bones, Joints, Vessels and Nerves)
Muscles Acting on the Elbow Joint
| Movement | Primary Muscles |
|---|---|
| Flexion | Brachialis (primary flexor), Biceps brachii (primary supinator; secondary flexor), Brachioradialis |
| Extension | Triceps brachii (3 heads: long, lateral, medial), Anconeus |
| Supination | Biceps brachii, Supinator |
| Pronation | Pronator teres, Pronator quadratus |
Key muscle details:
- Brachialis: originates from the anterior distal half of the humerus, inserts onto the coronoid process and ulnar tuberosity - it is the elbow's sole dedicated flexor
- Biceps brachii: long head from supraglenoid tubercle, short head from coracoid process; inserts at radial tuberosity and bicipital aponeurosis; primary supinator
- Triceps brachii: three heads converge on the olecranon; primary extensor
- Anconeus: blends with triceps distally; origin at lateral epicondyle, inserts on lateral olecranon and posterior ulna; secondary extensor and stabilizer against varus forces
Carrying Angle
The carrying angle is the angle between the long axis of the arm and the forearm when the elbow is fully extended and supinated.
- Normal: 5-10° in males, 10-15° (up to 20°) in females (valgus)
- Disappears when the forearm is flexed or pronated
- Cubitus valgus: carrying angle increased (>15°); may cause tardy ulnar nerve palsy
- Cubitus varus (gunstock deformity): common sequel to malunited supracondylar fracture in children
Movements and Range
| Movement | Normal Range |
|---|---|
| Flexion | 0° to 145° |
| Extension | 0° (or up to 5-10° hyperextension) |
| Supination (forearm) | 0° to 90° |
| Pronation (forearm) | 0° to 85° |
The ulnohumeral joint provides the majority of elbow stability, accounting for 55-75% of joint restriction during flexion and extension.
Nerve Supply
- Predominantly: branches of the radial nerve and musculocutaneous nerve
- Additional contributions from branches of the ulnar nerve and median nerve
- The ulnar nerve passes posterior to the medial epicondyle in the cubital tunnel (posterior bundle of UCL forms the floor); it is vulnerable here in fractures and cubitus valgus
Blood Supply
A rich periarticular anastomotic network around the elbow is formed by:
- Collateral branches: anterior and posterior branches of the profunda brachii artery; superior and inferior ulnar collateral arteries
- Recurrent branches: radial recurrent artery (from radial artery), anterior and posterior interosseous recurrent arteries (from ulnar artery), anterior ulnar recurrent and posterior ulnar recurrent arteries
- This network ensures collateral circulation even with arterial injury at the elbow
Elbow Position in Effusion
When joint effusion is present, the elbow is held in semi-flexion (~45°) - the position of greatest joint capacity and least intra-articular pressure. On imaging, the fat pad sign (displaced fat pads) is a radiographic indicator of joint effusion or hemarthrosis.
Clinical Correlations
| Condition | Anatomy |
|---|---|
| Supracondylar fracture (children) | Distal fragment displaced posteriorly by triceps; brachial artery can be bowstrung over fracture fragment causing forearm ischemia (Volkmann's contracture) |
| Pulled elbow / Nursemaid's elbow | Sudden traction on extended, pronated forearm causes radial head to slip through/under annular ligament |
| Tennis elbow (lateral epicondylitis) | Degeneration at the origin of common extensors (ECRB) from lateral epicondyle |
| Golfer's elbow (medial epicondylitis) | Degeneration at the origin of common flexors from the medial epicondyle |
| Cubital tunnel syndrome | Ulnar nerve compression in the cubital tunnel (floor = posterior UCL bundle) |
| Posterolateral rotatory instability | Disruption of the LUCL |
Sources: Gray's Anatomy for Students (9780323934237, pp. 884-885); Imaging Anatomy: Bones, Joints, Vessels and Nerves (9781626239845, Chapter 16); S. Das Manual on Clinical Surgery 13th Edition (9788190568104, p. 233)
This is a shared conversation. Sign in to Orris to start your own chat.