Make a case presentation of anemia patient of age 61 year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive textbook data. Let me compile the full case presentation.
Case Presentation: Iron Deficiency Anemia in a 61-Year-Old Male
I. PATIENT IDENTIFICATION
| Name | Mr. R.K. (identity anonymized) |
| Age | 61 years |
| Sex | Male |
| Occupation | Retired government clerk |
| Residence | Urban |
| Date of Admission | July 7, 2026 |
| Presenting to | Department of Internal Medicine |
II. CHIEF COMPLAINTS
- Fatigue and weakness - 4 months (progressive)
- Shortness of breath on exertion - 2 months
- Pallor noticed by family - 1 month
- Decreased appetite and weight loss (approximately 4 kg) - 2 months
III. HISTORY OF PRESENT ILLNESS
Mr. R.K., a 61-year-old retired male, presents with a 4-month history of gradually worsening fatigue that now significantly limits his daily activities. He reports dyspnea on climbing one flight of stairs and on moderate exertion, which was not present previously. He denies dyspnea at rest or orthopnea. Over the past 6 weeks, he has noticed progressive pallor.
He describes intermittent dull epigastric discomfort for approximately 3 months, especially after meals, with occasional dark, tarry stools on 2-3 occasions over the past month (melena). He has been taking aspirin 75 mg/day for the past 18 months following advice for cardiovascular protection, along with a proton pump inhibitor (omeprazole) which he occasionally skips.
He denies hematemesis, frank rectal bleeding, jaundice, or urinary symptoms. He admits to cold intolerance and occasional restlessness in his legs at night (restless leg syndrome). He denies pica (ice or clay craving) but endorses loss of appetite.
Pertinent negatives: No fever, no lymphadenopathy, no bone pain, no easy bruising or bleeding elsewhere.
IV. PAST MEDICAL HISTORY
| Condition | Duration | Treatment |
|---|---|---|
| Hypertension | 8 years | Amlodipine 5 mg/day |
| Type 2 Diabetes Mellitus | 6 years | Metformin 500 mg BD |
| No prior hospitalization for anemia | - | - |
V. DRUG HISTORY
- Aspirin 75 mg/day (18 months) - risk factor for GI blood loss
- Omeprazole 20 mg/day (irregular use) - PPI reduces ferric-to-ferrous iron conversion, contributing to iron malabsorption
- Amlodipine 5 mg/day
- Metformin 500 mg BD
VI. FAMILY & SOCIAL HISTORY
- Family history: Father had "stomach problem" (unknown diagnosis); no known family history of hematological malignancy or colon cancer
- Diet: Predominantly vegetarian; low meat intake reduces bioavailable heme iron
- Alcohol: Social drinker (1-2 drinks/week)
- Tobacco: Ex-smoker (quit 10 years ago, 15 pack-year history)
VII. REVIEW OF SYSTEMS
| System | Findings |
|---|---|
| General | Fatigue, weight loss (~4 kg/2 months), cold intolerance |
| GI | Epigastric discomfort, intermittent melena, reduced appetite |
| Cardiovascular | Exertional dyspnea, no chest pain at rest |
| Neurological | Restless legs at night |
| Musculoskeletal | Generalized weakness |
| Dermatological | Pallor; no koilonychia yet |
Per Goldman-Cecil Medicine: "Older patients with underlying comorbid conditions typically develop dyspnea and may even develop new onset or worsening angina." The exertional dyspnea in this 61-year-old is consistent with this pattern.
VIII. PHYSICAL EXAMINATION
General
- Conscious, oriented, cooperative; appears tired and pale
- Vital signs: BP 130/82 mmHg | HR 96 bpm (regular) | RR 18/min | Temperature 37.1°C | SpO2 97% on room air
- Weight 72 kg | Height 168 cm | BMI 25.5
Specific Systems
| System | Finding |
|---|---|
| Skin/Nails | Pallor of skin and conjunctivae +++ ; no koilonychia, no glossitis, no angular stomatitis at this stage |
| Eyes | Pale conjunctivae bilaterally |
| Oral | Mild pallor of oral mucosa; tongue appears slightly smooth |
| Cardiovascular | Tachycardia (HR 96); soft systolic flow murmur grade 2/6 at left sternal border (high-output state); no signs of cardiac failure |
| Respiratory | Clear to auscultation bilaterally; no wheeze or crepitations |
| Abdomen | Mild epigastric tenderness on deep palpation; liver and spleen not palpably enlarged; no mass palpable; bowel sounds normal |
| Rectal exam | Guaiac (fecal occult blood) positive; no external hemorrhoids; no palpable rectal mass |
| Lymph nodes | No peripheral lymphadenopathy |
| CNS | Normal |
IX. INVESTIGATIONS
A. Complete Blood Count (CBC)
| Parameter | Patient's Value | Normal Range |
|---|---|---|
| Hemoglobin | 7.8 g/dL | 13.5 - 17.5 g/dL (male) |
| Hematocrit | 25% | 41-53% |
| MCV | 68 fL | 80-100 fL |
| MCH | 22 pg | 27-33 pg |
| MCHC | 28 g/dL | 32-36 g/dL |
| RBC count | 3.2 x 10^12/L | 4.5-5.5 x 10^12/L |
| RDW | 17.5% (elevated) | 11.5-14.5% |
| WBC | 7.2 x 10^9/L | 4.0-11.0 x 10^9/L |
| Platelets | 420 x 10^9/L (reactive thrombocytosis) | 150-400 x 10^9/L |
| Reticulocytes | 0.8% (low - not reticulocytosis) | 0.5-2.5% |
Impression: Microcytic hypochromic anemia with elevated RDW and reactive thrombocytosis - classic iron deficiency pattern.
B. Peripheral Blood Smear
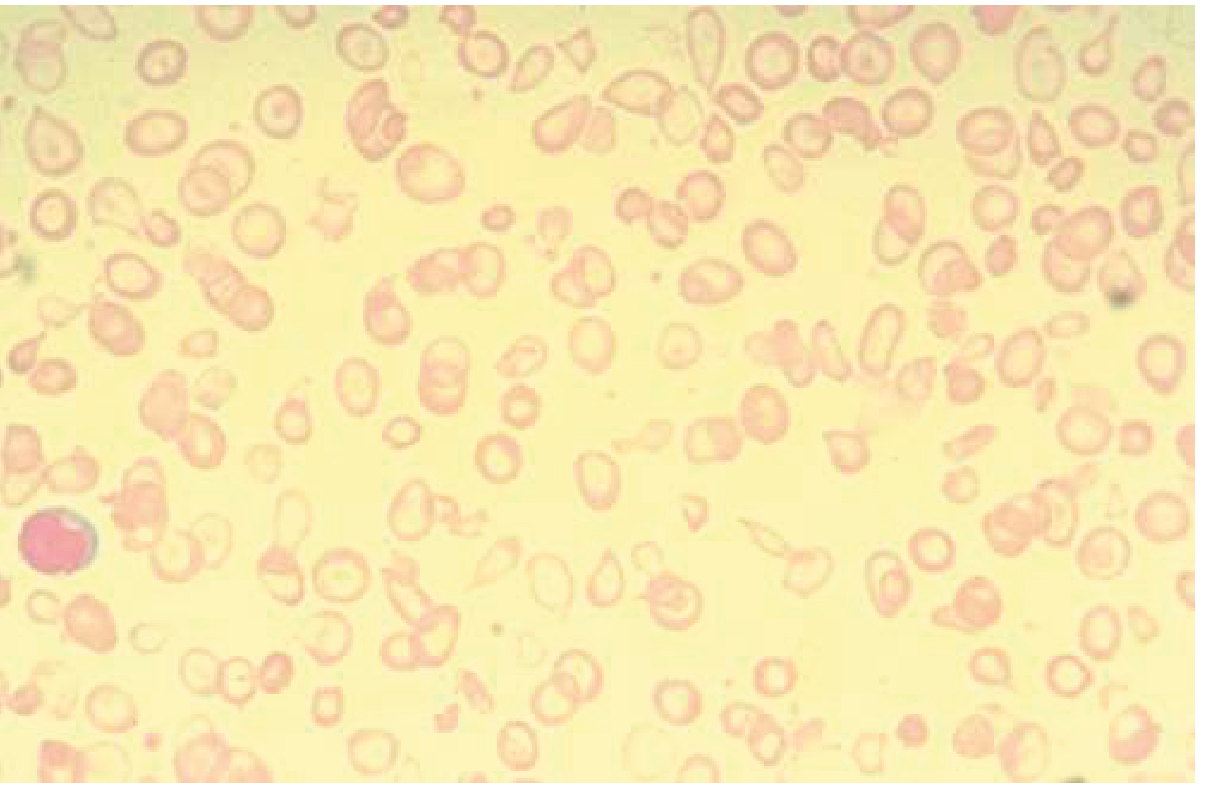
Peripheral blood smear (Goldman-Cecil Medicine, Fig. 145-2): Microcytic, hypochromic red blood cells with prominent central pallor and poikilocytosis - typical of iron deficiency anemia.
C. Iron Studies
| Test | Patient's Value | Normal Range | Interpretation |
|---|---|---|---|
| Serum Iron | 28 mcg/dL | 60-170 mcg/dL | Decreased |
| TIBC | 490 mcg/dL | 250-370 mcg/dL | Increased (specific for IDA) |
| Transferrin Saturation | 5.7% | 20-50% | Decreased (<16% = IDA) |
| Serum Ferritin | 8 ng/mL | 20-300 ng/mL | Severely decreased (<15 ng/mL = IDA) |
Per Goldman-Cecil Medicine: "A ferritin level of less than 15 ng/mL is very specific for iron deficiency." The TIBC is elevated, which is specific for iron deficiency (as opposed to anemia of chronic inflammation, where TIBC is decreased).
D. Additional Workup
| Test | Result | Significance |
|---|---|---|
| Fecal occult blood test (FOBT) | Positive | GI blood loss confirmed |
| Serum B12 | 320 pg/mL (normal) | Rules out B12 deficiency |
| Serum Folate | 8.2 ng/mL (normal) | Rules out folate deficiency |
| HbA1c | 7.1% | Suboptimal DM control |
| RBS | 148 mg/dL | Mildly elevated |
| Renal function (urea/creatinine) | Normal | No CKD-related anemia |
| LFTs | Normal | No liver disease |
| Serum CRP | 8 mg/L (mildly elevated) | Mild background inflammation (aspirin use / chronic GI irritation) |
| TSH | 2.8 mIU/L | Normal (rules out hypothyroid contribution) |
| Peripheral smear | Microcytic hypochromic cells, anisocytosis, pencil cells | Consistent with IDA |
| Hemoglobin electrophoresis | Normal HbA, no HbS, HbA2 <3.5% | Excludes thalassemia |
X. DIAGNOSIS
Confirmed Primary Diagnosis:
Iron Deficiency Anemia (IDA) - severe (Hb 7.8 g/dL), microcytic hypochromic
Underlying Cause (most likely):
Chronic occult gastrointestinal blood loss - in a 61-year-old male with FOBT positive, epigastric discomfort, intermittent melena, and long-term aspirin use
Differential Diagnoses Considered and Excluded:
| Differential | Reason Excluded |
|---|---|
| Anemia of Chronic Inflammation | Ferritin would be high (>200 ng/mL), TIBC decreased - not our pattern |
| Thalassemia minor | HbA2 normal on electrophoresis; RDW is elevated in IDA but normal/low in thalassemia |
| Sideroblastic anemia | Ferritin and serum iron are not elevated; no ringed sideroblasts |
| B12/Folate deficiency | Normal B12 and folate; anemia is microcytic, not macrocytic |
| Anemia of CKD | Renal function normal |
Per Goldman-Cecil Medicine: "Iron deficiency anemia must be distinguished from α- or β-thalassemia, in which serum iron and serum ferritin levels are normal or high. A low serum iron level with a high ferritin level is typical of the anemia of chronic inflammation."
XI. DIAGNOSTIC SUMMARY TABLE
| Feature | Our Patient | IDA Pattern |
|---|---|---|
| MCV | 68 fL (low) | Microcytic |
| Ferritin | 8 ng/mL (low) | <15 ng/mL |
| TIBC | 490 mcg/dL (high) | Increased |
| Transferrin saturation | 5.7% | <16% |
| Blood smear | Microcytic, hypochromic | Classic |
| Reticulocytes | Low/normal | Not elevated |
XII. MANAGEMENT
Step 1: Treat the Underlying Cause
- Upper GI endoscopy (OGD) urgently - to identify and treat the bleeding source (peptic ulcer, gastritis, gastric cancer given age >60 and weight loss)
- Colonoscopy - mandatory in any iron-deficient man >40 years to exclude colonic malignancy
- Helicobacter pylori testing - serology or rapid urease test; treat if positive (eradication reduces ulcer recurrence and associated blood loss)
- Reassess aspirin - discuss risk-benefit; consider switching to clopidogrel or adding misoprostol; ensure consistent PPI use
Per Goldman-Cecil Medicine: "Any man with unexplained iron deficiency or any iron-deficient woman over age 40 years should undergo both upper and lower gastrointestinal endoscopy to evaluate for occult blood loss."
Step 2: Iron Replacement Therapy
Oral Iron (First-line if tolerated)
- Ferrous sulfate 325 mg once daily (65 mg elemental iron) - taken on empty stomach or with meat protein to maximize absorption
- Alternative: Ferrous gluconate 325 mg if GI side effects occur (contains 35 mg elemental iron per tablet)
- Vitamin C co-administration enhances absorption
- Avoid with tea, coffee, calcium, antacids
- Monitor: Reticulocyte count rises within 1 week; Hb should increase by ~1 g/dL every 2 weeks
- Continue iron for 3-6 months after Hb normalizes to replenish stores
Intravenous Iron (if oral fails or not tolerated)
- Ferric carboxymaltose 750-1000 mg IV as a single dose
- Indicated if: oral iron not tolerated, ongoing GI blood loss too great for oral replacement, or Hb not rising within 2 weeks of oral therapy
- Options: ferumoxytol, low-molecular-weight iron dextran, ferric derisomaltose
Blood Transfusion
- Consider if Hb <7 g/dL with symptomatic cardiovascular compromise (angina, heart failure, hemodynamic instability), or pre-operative
- This patient (Hb 7.8 g/dL, hemodynamically stable) does not currently require transfusion
Step 3: Dietary Advice
- Increase dietary iron: lean red meat (richest in heme iron), liver, legumes, dark green vegetables
- Avoid iron antagonists at meal time: tea, coffee, high-fiber cereals, calcium-rich foods
- Cooking in cast iron cookware can modestly increase dietary iron
Step 4: Monitor and Follow Up
| Timepoint | What to Monitor |
|---|---|
| 1 week | Reticulocyte count (should rise) |
| 4 weeks | Hemoglobin (should increase ~2 g/dL) |
| 3 months | Repeat CBC, iron studies, ferritin |
| 6 months | Confirm iron stores repleted (ferritin >50 ng/mL) |
| Ongoing | Results of GI endoscopy; treat underlying cause |
XIII. PROBLEM LIST SUMMARY
- Severe iron deficiency anemia (Hb 7.8 g/dL, MCV 68 fL, ferritin 8 ng/mL)
- Occult GI blood loss (melena history, FOBT positive, aspirin use) - requires urgent endoscopy to exclude malignancy
- Hypertension - continue amlodipine; reassess aspirin use
- Type 2 Diabetes - suboptimal control; continue metformin, review HbA1c
- Restless leg syndrome - likely iron-related; will improve with iron repletion
XIV. PROGNOSIS
The prognosis is good for the anemia itself with appropriate iron replacement. The key determinant of long-term outcome is the underlying cause of GI blood loss. If endoscopy identifies a benign peptic ulcer, full recovery is expected. If a GI malignancy is found, management and prognosis will depend on stage. Given his age (61), weight loss, and melena, malignancy must be actively excluded before attributing blood loss solely to aspirin-related gastritis.
References:
- Goldman-Cecil Medicine, 26e - Chapter 145: Iron Deficiency Anemia (pp. 1680-1682)
- Harrison's Principles of Internal Medicine, 22e - Chapter 102: Iron Deficiency and Iron-Deficiency Anemia (p. 806)
This is a shared conversation. Sign in to Orris to start your own chat.