In detail about pathological gait for Orthopaedic postgraduate exam in simple words
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have all the content I need from multiple authoritative textbooks. Let me compile the comprehensive answer.
Pathological Gait - Complete Guide for Orthopaedic PG Exams
Part 1: Normal Gait - Quick Review (Foundation)
Before understanding abnormal gaits, you must know the basics.
The Gait Cycle = one complete stride (heel strike of one foot to the next heel strike of the same foot)
| Phase | % of Cycle | What Happens |
|---|---|---|
| Stance phase | 60% | Foot is on the ground (weight-bearing) |
| Swing phase | 40% | Foot is in the air (moving forward) |
| Double limb support | 20-30% | Both feet on ground simultaneously |
Stance Phase Sub-events:
- Initial contact (IC) - heel strikes the ground
- Loading response (LR) - weight shifts to that limb
- Midstance (MSt) - body passes over the foot
- Terminal stance (TSt) - heel rises
- Pre-swing (PSw) - toe-off
Key Muscle Roles (High-Yield):
| Muscle | Phase | Action |
|---|---|---|
| Gluteus medius | Midstance | Prevents pelvis drop (eccentric) |
| Gluteus maximus | Initial contact | Powers hip extension (concentric) |
| Quadriceps | IC and pre-swing | Stabilizes knee (eccentric) |
| Tibialis anterior | Swing | Dorsiflexes ankle (concentric); slows plantar flexion at IC (eccentric) |
| Gastrocnemius-soleus | Stance | Controls dorsiflexion rate (eccentric) |
Normal vertical displacement of center of gravity = 5 cm; lateral displacement = 6 cm
- Miller's Review of Orthopaedics 9th Edition
Part 2: Pathological Gaits - The High-Yield List
The five main causes of pathological gait:
- Muscle weakness / paralysis
- Neurological conditions (spasticity, incoordination)
- Pain
- Limb deformity
- Joint disease (contracture, restricted ROM)
1. Antalgic Gait ("Pain-avoiding gait")
Cause: Pain in one limb - most commonly hip, knee, or foot pathology
What happens:
- The patient shortens the stance phase on the painful side (spends less time on it)
- The swing phase on the other side is also shortened (so they don't stay on the painful side too long)
- The cycle becomes asymmetric - shorter steps on the painful side
Simple image: The patient is trying to "get off" the painful leg as quickly as possible.
Common causes: OA hip/knee, fracture, infection, plantar fasciitis
"Pain in a limb creates an antalgic gait pattern in which the individual shortens the stance phase to lessen the time the painful limb is loaded; the contralateral swing phase is more rapid." - Miller's Review of Orthopaedics 9th Edition
2. Trendelenburg Gait ("Gluteus medius weakness gait")
Cause: Weakness of the hip abductors (gluteus medius/minimus) on the affected side
What happens:
- Normally, gluteus medius keeps the pelvis level when you stand on one leg
- When it is weak: on standing on the affected side, the pelvis drops toward the opposite (unaffected) side
- To compensate, the patient leans the trunk over the weak side - this shifts the body's center of gravity and reduces the demand on the abductors
Uncompensated: Pelvis drops (positive Trendelenburg sign)
Compensated (Trendelenburg Gait): Patient lurches trunk to the weak side to prevent the drop - appears as side-to-side "waddling" of the shoulders while walking
Causes:
- Gluteus medius paralysis (superior gluteal nerve injury)
- Painful hip (hip won't abduct fully - pseudoTrendelenburg)
- DDH (developmental dysplasia of hip)
- Old Perthes disease
- After total hip arthroplasty (abductor damage)
Bilateral involvement (bilateral hip pathology, like bilateral DDH or myopathy) produces the waddling gait - exaggerated side-to-side movement.
"Weakness of the hip adductors results in dipping of the pelvis to the other side when bearing weight on the affected limb... This Trendelenburg gait is apparent as side-to-side movement of the shoulders when walking." - Rheumatology, 2-Volume Set (Elsevier 2022)
3. Steppage Gait (High-stepping gait / Foot-drop gait / Equine gait)
Cause: Weakness of ankle dorsiflexors (tibialis anterior) causing foot drop
Pathology: Cannot dorsiflex the foot during swing phase, so the foot hangs down with toes pointing toward the ground
Compensation: The patient lifts the knee excessively high during swing phase to stop the toes from catching on the ground
What you hear: A characteristic foot "slap" as the foot hits the ground (because controlled plantar flexion is lost at initial contact)
Associated with: NOT troubled by imbalance - patients typically fall by tripping on carpet edges and curbstones
Unilateral vs Bilateral:
- Unilateral: Common peroneal nerve palsy, L4-L5 root lesion, sciatic nerve injury
- Bilateral: Charcot-Marie-Tooth disease, bilateral L5 lesions, Guillain-Barre, certain muscular dystrophies
Key nerve: Common peroneal (fibular) nerve at the fibular neck is the most common site
"This gait pattern is caused by paralysis of the pretibial and peroneal muscles... Walking is accomplished by excessive flexion at the hip, the leg being lifted abnormally high in order for the foot to clear the ground. There is a slapping noise as the foot strikes the floor." - Adams and Victor's Principles of Neurology 12th Ed
4. Hemiplegic Gait (Circumduction gait)
Cause: Unilateral UMN (upper motor neuron) lesion - spasticity + weakness of one side (e.g. stroke, head injury, hemiplegia)
What happens:
- The affected leg is stiff - does not flex normally at hip, knee, and ankle
- During swing phase, the leg is swung outward in a semicircle (circumduction) - away from the body and then back
- The foot scrapes the floor, typically at the toe and outer heel
- The arm on the same side is held flexed and adducted, and does not swing
What you hear: Slow, rhythmic scuffing sound; medial toe of the shoe shows wear
Causes: Stroke (CVA), traumatic brain injury, any unilateral corticospinal tract lesion
5. Scissor Gait (Spastic paraplegic gait)
Cause: Bilateral UMN lesion causing spastic paraplegia - essentially a "double hemiplegic gait"
What happens:
- Both legs are stiff with adductor spasticity
- The thighs are strongly adducted and almost cross each other as the patient walks (like scissors cutting)
- Steps are short and slow; the patient moves with great effort
Classic description: "Wading waist-deep in water"
Causes:
- Cerebral diplegia (Little's disease) - most classic cause for PG exams
- Spinal cord lesions: Multiple sclerosis, cord compression, syringomyelia
- Bilateral corticospinal tract damage
"The legs are extended or slightly bent at the knees, and the thighs may be strongly adducted, causing the legs almost to cross as the patient walks (scissor-like gait)." - Adams and Victor's Principles of Neurology 12th Ed
6. Waddling Gait (Myopathic gait / Bilateral Trendelenburg)
Cause: Bilateral proximal weakness - mainly hip abductors and extensors
What happens:
- Same as Trendelenburg, but bilateral
- The body rocks from side to side with each step (trunk lurches left then right)
- Often combined with hyperlordosis of the lumbar spine (to compensate for weak hip extensors)
- Toe walking may occur in early Duchenne
Causes:
- Duchenne muscular dystrophy (classic PG exam favorite)
- Limb-girdle muscular dystrophy
- Polymyositis
- Bilateral hip OA / bilateral DDH
High-yield point: Gowers' sign is associated with this gait pattern in Duchenne MD.
7. Parkinsonian (Festinating) Gait
Cause: Basal ganglia dysfunction - Parkinson's disease (hypokinetic-rigid syndrome)
Features (the "FROST" mnemonic is useful):
- F - Festination (steps get faster and faster, can't stop)
- R - Reduced arm swing (arms held slightly flexed, not swinging)
- O - Overall forward bent posture (stooped, flexed neck, knees, elbows)
- S - Short shuffling steps (feet barely clear the ground)
- T - Trouble initiating (freezing at doorways, turns en bloc)
What happens: Body's center of gravity moves ahead of the feet; patient tries to "catch up" with their own center of gravity, resulting in progressively quickening small steps (festination - from Latin "festinare" = to hasten)
Retropulsion: If pushed from the front, the patient takes small backward steps (retropulsive festination).
"Once walking has started, the upper part of the body advances ahead of the lower part, and the patient is impelled to take increasingly short and rapid steps as though trying to catch up to their center of gravity." - Adams and Victor's Principles of Neurology 12th Ed
8. Cerebellar Ataxic Gait (Drunken gait)
Cause: Cerebellar damage (cerebellum coordinates balance and movement)
Features:
- Wide-based gait (feet far apart for stability)
- Irregular, lurching steps - veering to one or both sides
- Cannot walk heel-to-toe (tandem walking fails)
- NOT worsened by closing eyes (unlike sensory ataxia)
- Unsteadiness is present even with eyes open
Causes: Alcohol, MS, cerebellar tumors, spinocerebellar ataxias (Friedreich's ataxia)
9. Sensory Ataxic Gait (Tabetic gait / Stamping gait)
Cause: Loss of proprioception (dorsal columns, large fiber neuropathy, posterior roots)
Features:
- Wide-based stamping gait - feet are thrown out and forcibly brought down ("stamp and stick")
- Patient watches the ground carefully (using vision to substitute for lost proprioception)
- Romberg sign positive - markedly worse with eyes closed (hallmark)
- Patient is aware that the problem is in the legs, not the head (no dizziness)
Causes: Tabes dorsalis (syphilis - classic), vitamin B12 deficiency (subacute combined degeneration), Friedreich's ataxia, large-fiber polyneuropathies
"Stamp and stick" - Ramsay Hunt's classic description of sensory ataxic gait, from Adams and Victor's Principles of Neurology 12th Ed
10. Leg Length Discrepancy Gait
Cause: Unequal leg lengths (LLD)
Two patterns:
- Equinus pattern: The longer limb is used as-is; the patient tilts the pelvis - appears as Trendelenburg-type sway
- Bending pattern: The longer limb's knee is flexed during swing to clear the ground - body dips up and down as it walks
If LLD > 2-3 cm, it is usually noticeable clinically.
Quick Comparison Table (Exam Favorite)
| Gait Type | Cause | Key Feature | Lesion |
|---|---|---|---|
| Antalgic | Pain | Short stance on painful side | Any painful condition |
| Trendelenburg | Weak gluteus medius | Trunk lurches to weak side | Superior gluteal nerve / hip |
| Steppage | Foot drop | High knee lift, foot slap | Common peroneal nerve, L4-5 |
| Hemiplegic | Unilateral UMN | Circumduction, flexed arm | Stroke / corticospinal tract |
| Scissor | Bilateral UMN spasticity | Crossing legs (scissors) | Cerebral diplegia, spinal cord |
| Waddling | Bilateral proximal weakness | Side-to-side lurch + lordosis | Duchenne / myopathy |
| Parkinsonian | Basal ganglia | Shuffling, festination, freezing | Parkinson's disease |
| Cerebellar | Cerebellar lesion | Wide base, no Romberg | Cerebellum |
| Sensory ataxic | Proprioception loss | Stamping, Romberg +ve | Dorsal columns / large fibers |
(From Adams and Victor's Principles of Neurology 12th Ed - Table 6-1)
Gait Pattern Illustrations
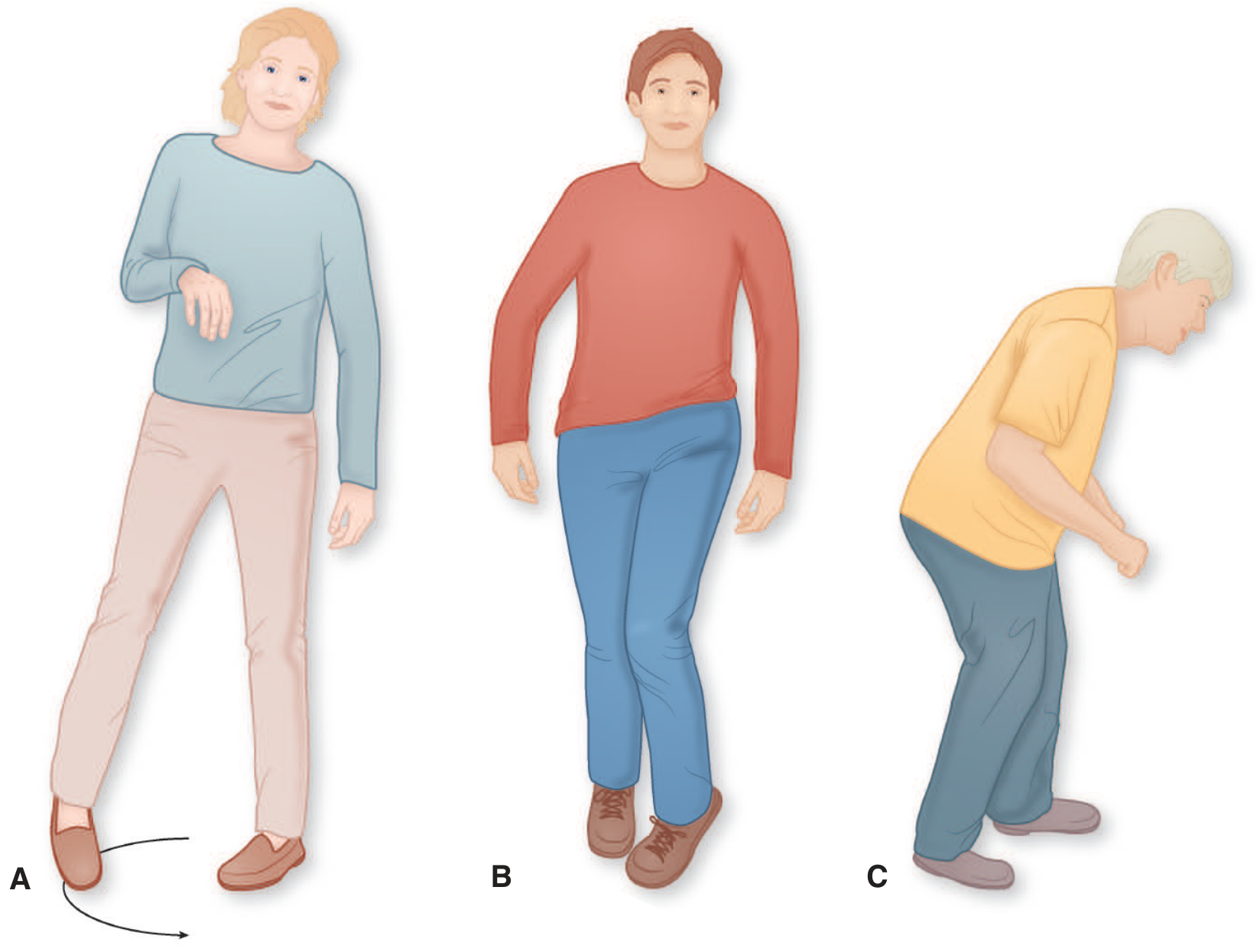
A = Hemiplegic gait (circumduction) | B = Scissor gait (spastic paraplegia) | C = Parkinsonian gait (stooped, shuffling)
Part 3: PG Exam High-Yield Points
1. Trendelenburg test:
- Positive Trendelenburg sign = pelvis drops on the LIFTED side when standing on the affected limb
- Causes: gluteus medius weakness, hip pain (any cause), DDH, Perthes
2. Foot drop nerve:
- Common peroneal (fibular) nerve at the fibular neck = most common cause of unilateral steppage gait
- Root level: L4, L5
3. Scissor gait = cerebral diplegia (Little's disease):
- Commonest cause is perinatal hypoxic brain injury
- Also seen in spinal cord disorders (MS, cord compression)
4. Duchenne muscular dystrophy:
- Classic waddling gait + toe walking + Gowers' sign + pseudohypertrophy of calves + hyperlordosis
5. Festination:
- Latin: "to hasten" - the involuntary acceleration in Parkinson's gait
- Distinguish from marche à petit pas (senile gait) - also small steps but NO festination, NO tremor
6. "Stamp and stick" = sensory ataxic (tabetic) gait - patient uses a stick and stamps the feet
7. Cerebellar vs sensory ataxia:
- Cerebellar: Romberg negative (still unsteady with eyes open)
- Sensory: Romberg positive (much worse when eyes closed)
8. Antalgic vs Trendelenburg:
- Antalgic: Short STANCE phase on affected side
- Trendelenburg: Trunk LURCH to affected side during stance phase
Sources: Miller's Review of Orthopaedics 9th Ed; Adams and Victor's Principles of Neurology 12th Ed; Campbell's Operative Orthopaedics 15th Ed 2026; Rheumatology 2-Volume Set (Elsevier 2022)
This is a shared conversation. Sign in to Orris to start your own chat.