Management of refeeding syndrome
Reading File
Finding Sources
Searching PubMed
"refeeding syndrome" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a detailed, well-organized answer:
Management of Refeeding Syndrome
Definition & Background
Refeeding syndrome was first described after WWII when severely malnourished prisoners were refed and experienced fatal electrolyte crises. It is a potentially life-threatening metabolic complication occurring within 72 hours of reintroducing nutrition (enteral or parenteral) after a period of starvation (>5 days), and is magnified in those with prolonged malnutrition. - Current Surgical Therapy 14e
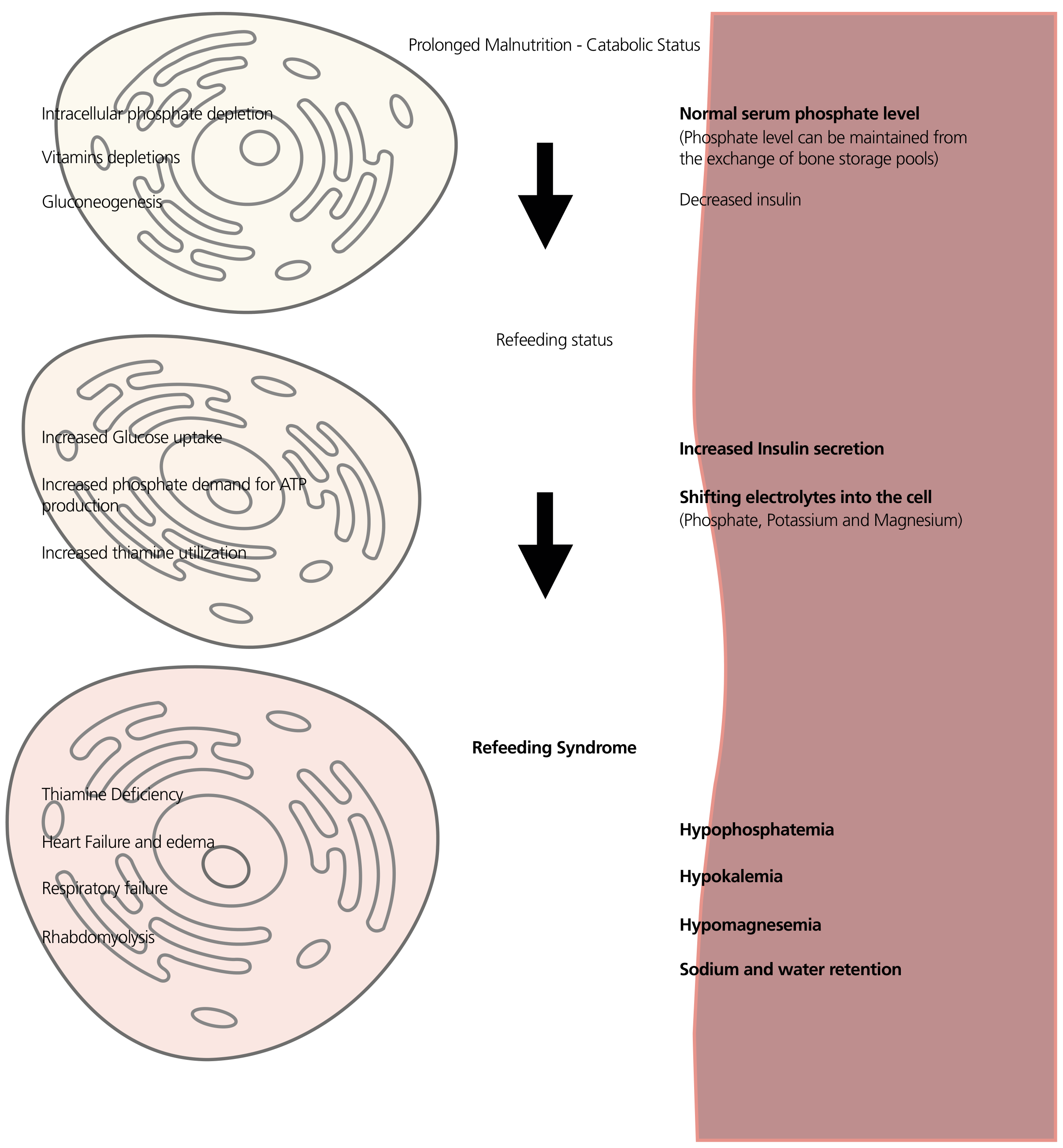
Pathophysiology
During starvation, the body shifts to fat and amino acid metabolism. Intracellular minerals (phosphate, potassium, magnesium) are depleted, but serum levels often remain falsely normal due to exchange from bone storage pools.
When carbohydrates are reintroduced:
- Insulin surge - stimulates Na/K-ATPase, driving potassium out of serum into cells
- Phosphate consumption - massively consumed by glycolysis for ATP synthesis → severe hypophosphatemia
- Magnesium shifts intracellularly (mechanism not fully elucidated); exacerbates hypokalemia
- Thiamine is a cofactor for pyruvate dehydrogenase; without it, pyruvate cannot enter the Krebs cycle - requirements spike dramatically during refeeding
- Sodium and water retention occur, worsening fluid overload
- Yamada's Textbook of Gastroenterology, 7th ed.
At-Risk Patients (NICE Criteria)
Significant risk - ONE criterion needed:
- BMI <16 kg/m²
- Unintentional weight loss >15% in last 3-6 months
- Little or no intake for >10 days
- Low K⁺, PO₄³⁻, or Mg²⁺ prior to feeding
Moderate risk - TWO criteria needed:
- BMI <18.5 kg/m²
- Unintentional weight loss >10% in 3-6 months
- Little or no intake for >5 days
- History of alcohol abuse, or use of insulin, chemotherapy, antacids, or diuretics
Other high-risk groups: anorexia nervosa, chronic alcoholism, cancer, AIDS, post-bariatric surgery, delayed nutritional support, massive obesity with recent extreme weight loss. - Bailey and Love's Short Practice of Surgery 28th ed.; Tietz Textbook of Laboratory Medicine 7th ed.
Clinical Features
| System | Manifestation |
|---|---|
| Cardiac | Arrhythmias, cardiac failure, cardiac arrest (from hypophosphatemia) |
| Neurological | Confusion, lethargy, seizures |
| Respiratory | Respiratory failure/muscle weakness |
| Metabolic | Lactic acidosis, hyperglycemia |
| Musculoskeletal | Muscle weakness, rhabdomyolysis |
| Fluid | Oedema, heart failure from Na/water retention |
| Nutritional | Wernicke's encephalopathy (thiamine deficiency) |
Management
1. Pre-feeding: Identify and correct deficits FIRST
- Check and correct electrolyte imbalances (K⁺, PO₄³⁻, Mg²⁺, Ca²⁺) before starting nutrition
- Correct volume deficits
- Administer thiamine 100 mg IV/IM before initiating feeding or any glucose-containing fluids - especially critical in alcoholics and severely starved patients; continue 100 mg/day for 5-7 days in high-risk patients
- Give supplementary B vitamins and multivitamins
2. Start nutrition slowly
| Risk Level | Starting Rate |
|---|---|
| Standard at-risk | 50% of estimated energy requirements on day 1 |
| Highest risk (prolonged starvation, chronic electrolyte losses) | ≤10 kcal/kg/day |
| Both | Gradually increase to full requirements over 4-7 days |
For parenteral nutrition: start with only 50% of the dextrose on day 1 as an added safety measure. - Yamada's Textbook of Gastroenterology; Bailey and Love's 28th ed.; Sabiston Textbook of Surgery
3. Electrolyte monitoring and repletion
Monitor phosphate, potassium, magnesium, and calcium closely and replace aggressively as levels fall:
| Electrolyte | Management |
|---|---|
| Phosphate (severe, <1.0 mg/dL) | IV phosphate up to 45 mmol (rate up to 20 mmol/h); choose sodium phosphate vs. potassium phosphate based on K⁺ level; avoid too-rapid infusion (risk of Ca²⁺ precipitation) |
| Phosphate (moderate) | Oral supplementation in divided doses (up to 3x normal intake) |
| Potassium | IV or oral replacement; frequency of checks increased in refeeding syndrome |
| Magnesium | IV or oral replacement |
| Calcium | Monitor; correct as needed |
Frequency: electrolyte checks at minimum daily during the initiation phase - more frequently in severe cases. - Sabiston Textbook of Surgery
4. Vitamins and micronutrients
- Thiamine (as above - mandatory before feeding)
- Vitamin B complex
- Daily multivitamins
- Trace elements
5. Ongoing monitoring
- Vital signs and fluid balance daily
- Blood glucose: hyperglycemia is common (especially in elderly, critically ill, or diabetics) - treat with IV insulin if needed; avoid abrupt cessation of PN (risk of rebound hypoglycaemia)
- Daily electrolytes until stable
- Adjust feed rate if electrolytes drop sharply
Summary Algorithm
Identify at-risk patient
↓
Correct electrolyte deficits (K⁺, PO₄³⁻, Mg²⁺, Ca²⁺)
↓
Thiamine 100 mg BEFORE feeding starts
↓
Start feeding at ≤10 kcal/kg/day (or 50% energy requirements)
↓
Increase gradually over 4–7 days to full requirements
↓
Monitor electrolytes, blood glucose, fluid balance daily
↓
Aggressively replete electrolyte deficits as they emerge
Sources: Bailey and Love's Short Practice of Surgery 28th ed. | Current Surgical Therapy 14e | Yamada's Textbook of Gastroenterology 7th ed. | Sabiston Textbook of Surgery | Schwartz's Principles of Surgery 11th ed. | Tietz Textbook of Laboratory Medicine 7th ed.
Recent evidence note (PubMed, 2024-2026): A 2025 systematic review (PMID 39187889) identified prolonged starvation, low BMI, and pre-existing electrolyte abnormalities as the most consistent risk factors. A 2026 systematic review on critically ill adults (PMID 41793849) highlighted that no single validated risk prediction model has yet been universally adopted - clinical judgment using NICE criteria remains the standard. These findings are consistent with textbook guidance above.
What fluid required
Finding Sources
Finding Sources
Reading File
Reading File
Excellent - comprehensive data from Harrison's and Tietz. Here is the focused answer:
Fluid Requirements in Refeeding Syndrome
Why Fluid is a Problem
Fluid management in refeeding syndrome is particularly hazardous because insulin - released when carbohydrates are reintroduced - has a potent anti-natriuretic effect: it causes renal sodium (and therefore water) retention. The malnourished heart is also atrophied and cannot handle sudden volume loading. Excess fluid and sodium intake can rapidly cause volume expansion, manifesting as:
- Peripheral oedema ("refeeding oedema")
- Pulmonary oedema
- Acute left heart failure (due to three concurrent mechanisms)
As Harrison's 22e explains, left heart failure in refeeding has three simultaneous causes:
- Abrupt increase in intravascular volume from administered fluids + insulin-mediated renal sodium retention
- Increased cardiac demand placed on an already atrophic left ventricle (insulin raises resting energy expenditure)
- Myocardial deficiencies of potassium, phosphorus, and magnesium
- Harrison's Principles of Internal Medicine 22E
Fluid Type
| Scenario | Fluid of Choice |
|---|---|
| Hypovolaemia / pre-refeeding volume deficit | Isotonic saline (0.9% NaCl) - volume repletion before feeding begins |
| Hypovolaemic hyponatraemia (e.g. eating disorders) | Isotonic saline (normal saline is treatment of choice) |
| Electrolyte repletion (phosphate, K⁺, Mg²⁺) | IV phosphate/potassium/magnesium solutions added separately |
| Maintenance during feeding | Restrict sodium-containing fluids - use the minimum needed |
- Frameworks for Internal Medicine; Bailey and Love's 28th ed.
Critically: avoid glucose-containing fluids (e.g. 5% dextrose) as a sole maintenance fluid - they worsen the insulin surge and accelerate phosphate/potassium shift. If glucose fluids are unavoidable (e.g. PN), start at only 50% of dextrose on day 1.
Sodium and Water Restriction - The Key Principle
Sodium should be severely restricted in the refeeding phase:
- Excess sodium directly drives fluid retention via insulin's anti-natriuretic action
- "Refeeding oedema can be minimized by severely limiting sodium provision and increasing carbohydrate provision slowly" - Harrison's 22E
- For parenteral nutrition: keep sodium content of bags to the minimum needed (do not give routine maintenance sodium volumes)
Fluid Volume - Practical Guidance
There is no single "fixed" daily fluid prescription, but the following principles apply from the textbook evidence:
| Parameter | Guidance |
|---|---|
| Pre-feeding | Correct dehydration/volume deficit first with isotonic saline, before any calories are started |
| During refeeding | Restrict sodium to avoid oedema; match fluid input to output + insensible losses |
| Rate of rehydration | Slow and measured - avoid bolus sodium loads |
| In PN patients | Limiting total fluid volume is part of the strategy alongside limiting dextrose |
| Monitoring | Daily fluid balance charts; watch for weight gain >0.5 kg/day (indicates fluid accumulation) |
Diagnostic Severity Grading (Tietz / Recent Consensus)
Recent consensus defines refeeding syndrome severity by electrolyte falls and organ dysfunction:
| Grade | Definition |
|---|---|
| Mild | ≥10-20% drop in PO₄³⁻, K⁺, or Mg²⁺ |
| Moderate | 20-30% drop |
| Severe | >30% drop and/or organ dysfunction (cardiac failure, respiratory failure) or thiamine deficiency |
In severe cases (organ dysfunction), aggressive IV electrolyte replacement is needed, but fluid volumes should still be carefully controlled to avoid worsening heart failure.
Summary of Key Fluid Rules
- Correct volume deficits with isotonic saline before feeding starts
- Severely restrict sodium once feeding begins - it is the main driver of refeeding oedema
- Avoid glucose-containing IV fluids unless part of a controlled feeding regimen (start at ≤50% dose)
- Monitor daily fluid balance - weight, urine output, clinical signs of overload
- Slow down or pause feeding if oedema or heart failure develops
- Electrolyte replacement fluids (phosphate, Mg²⁺, K⁺) are given in addition - choose sodium phosphate vs potassium phosphate based on the patient's K⁺ level
Sources: Harrison's Principles of Internal Medicine 22E | Tietz Textbook of Laboratory Medicine 7th ed. | Bailey and Love's Short Practice of Surgery 28th ed. | Schwartz's Principles of Surgery 11th ed. | Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.