Applied anatomy of bronchial Tree and root of lung according standard book
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive information from Gray's Anatomy for Students and Fischer's Mastery of Surgery. Let me compile the complete, well-illustrated answer.
Applied Anatomy of the Bronchial Tree and Root of the Lung
Sources: Gray's Anatomy for Students (Gray's AFS) | Fischer's Mastery of Surgery, 8th ed.
1. The Bronchial Tree
Trachea - The Beginning
The trachea is a flexible tube (~11 cm long, 2-2.5 cm wide) extending from vertebral level C6 in the lower neck to T4/T5 in the mediastinum, where it bifurcates into the right and left main bronchi. It is held open by C-shaped hyaline cartilage rings with the open part facing posteriorly (the posterior wall is smooth muscle). The lowest ring bears the carina - a hook-shaped projection in the midline between the two main bronchi that is normally vertical, sharp, and narrow.
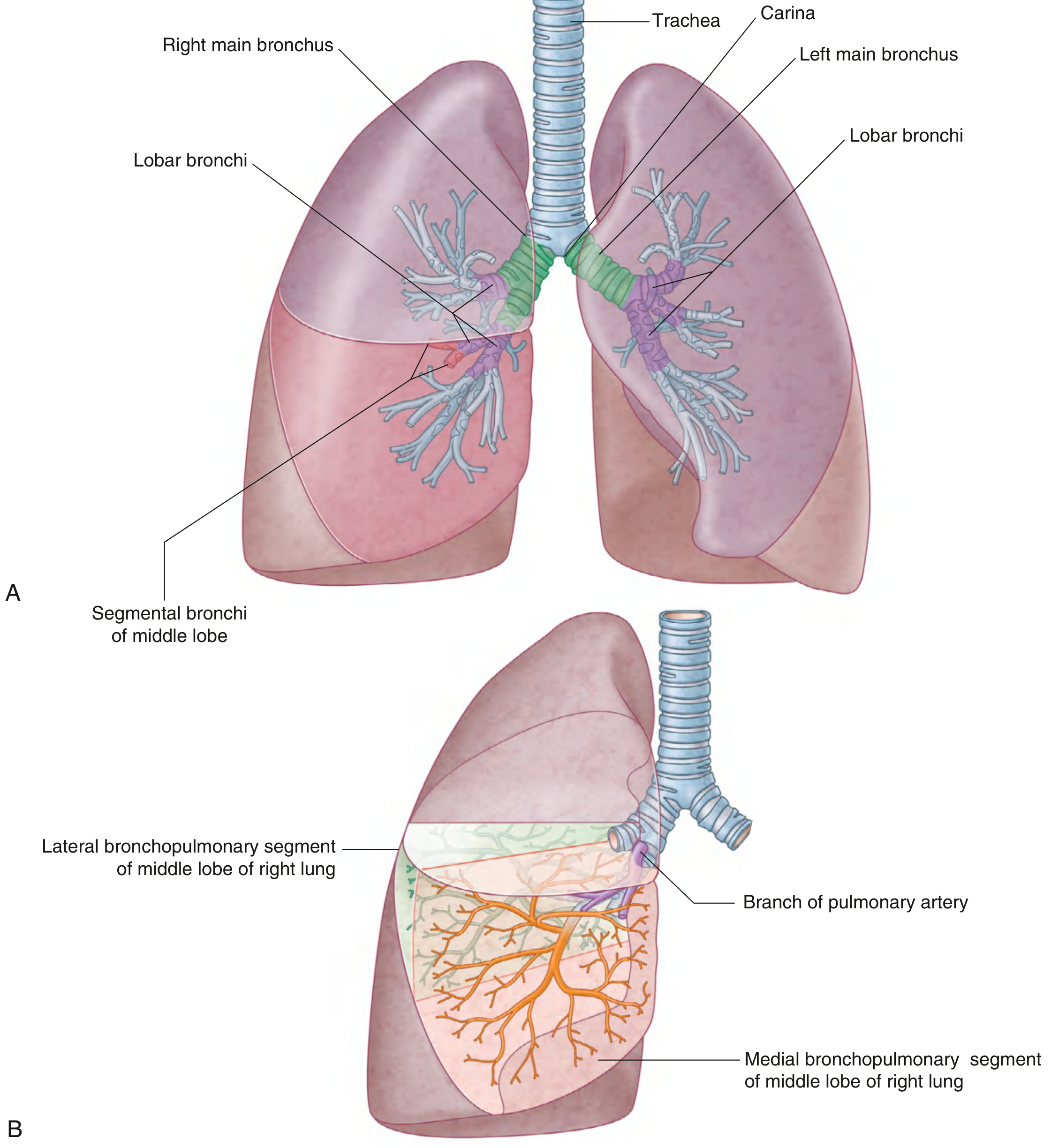
Main Bronchi - Key Differences (High-Yield Applied Point)
| Feature | Right Main Bronchus | Left Main Bronchus |
|---|---|---|
| Width | Wider | Narrower |
| Direction | More vertical | More horizontal |
| Length (before 1st lobar branch) | Shorter (~2-3 cm) | Longer |
| Superior lobar bronchus origin | Within the root of the lung | Within the lung |
| Foreign body tendency | More common (due to vertical course) | Less common |
| Endotracheal tube | Preferentially enters here if passed too deeply | Not preferred |
The right main bronchus is shorter and takes a more direct course from the trachea - bronchoscopically, the superior lobe orifice lies 2-3 cm from the carina, usually in a very lateral location. - Fischer's Mastery of Surgery, p.2056
Lobar Bronchi (Secondary Bronchi)
- Right lung - 3 lobar bronchi: upper, middle, lower
- Left lung - 2 lobar bronchi: upper, lower
The right upper lobe bronchus arises within the root of the lung (before entering the hilum proper). The remainder arise after passing through the hilum.
Segmental Bronchi (Tertiary Bronchi) and Bronchopulmonary Segments
Lobar bronchi divide into segmental bronchi, each supplying one bronchopulmonary segment. There are 10 segments in each lung (some fuse in the left lung).
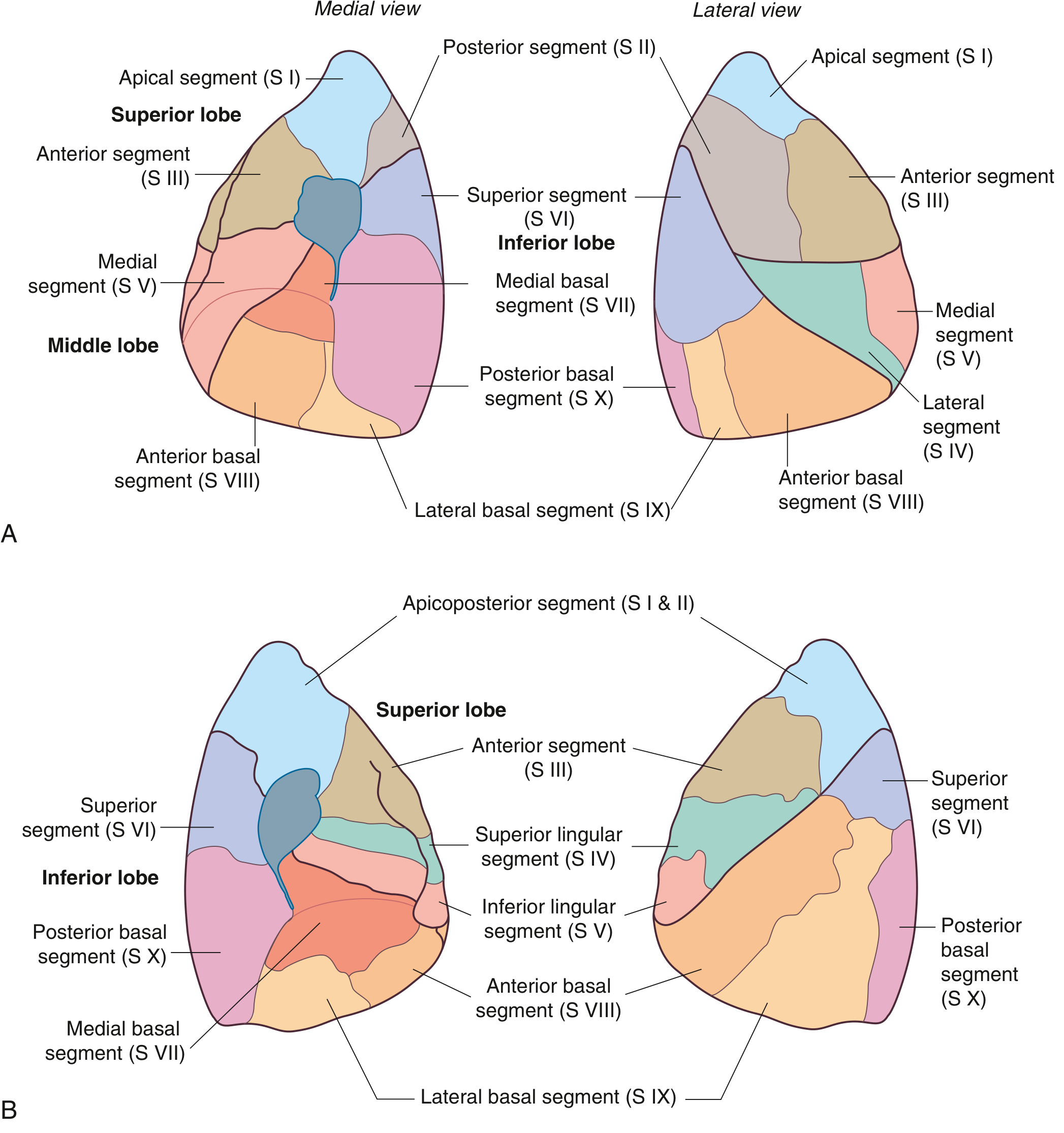
Right lung segments:
- Upper lobe: Apical (SI), Posterior (SII), Anterior (SIII)
- Middle lobe: Lateral (SIV), Medial (SV)
- Lower lobe: Superior (SVI), Medial basal (SVII), Anterior basal (SVIII), Lateral basal (SIX), Posterior basal (SX)
Left lung segments:
- Upper lobe: Apicoposterior (SI+II fused), Anterior (SIII), Superior lingular (SIV), Inferior lingular (SV)
- Lower lobe: Superior (SVI), Medial basal (SVII), Anterior basal (SVIII), Lateral basal (SIX), Posterior basal (SX)
Applied point: A bronchopulmonary segment is the smallest functionally independent unit of the lung - the smallest area that can be surgically resected (segmentectomy) without affecting adjacent segments. Pulmonary veins pass intersegmentally between segments. - Gray's AFS, p.210
Within each segment, segmental bronchi give rise to multiple generations, then to bronchioles - which lack cartilage in their walls (unlike bronchi).
2. Root of the Lung
Definition
The root of the lung is formed when the mediastinal pleura (at vertebral levels T5-T7) reflects off the mediastinum as a tubular, sleeve-like covering encasing the airway, vessels, nerves, and lymphatics that pass between the lung and mediastinum. The root joins the medial surface of the lung at the hilum. - Gray's AFS, p.201
Below the hilum, the pleural sleeve narrows to form the pulmonary ligament.
Contents of the Root (Hilum)
The following structures pass through the root of each lung:
- Main bronchus (most posterior in the hilum)
- Pulmonary artery (intermediate position)
- Pulmonary veins (most anterior and inferior)
- Bronchial arteries and veins
- Autonomic nerve plexuses (anterior + posterior pulmonary plexuses)
- Lymphatics and lymph nodes
- Loose connective tissue
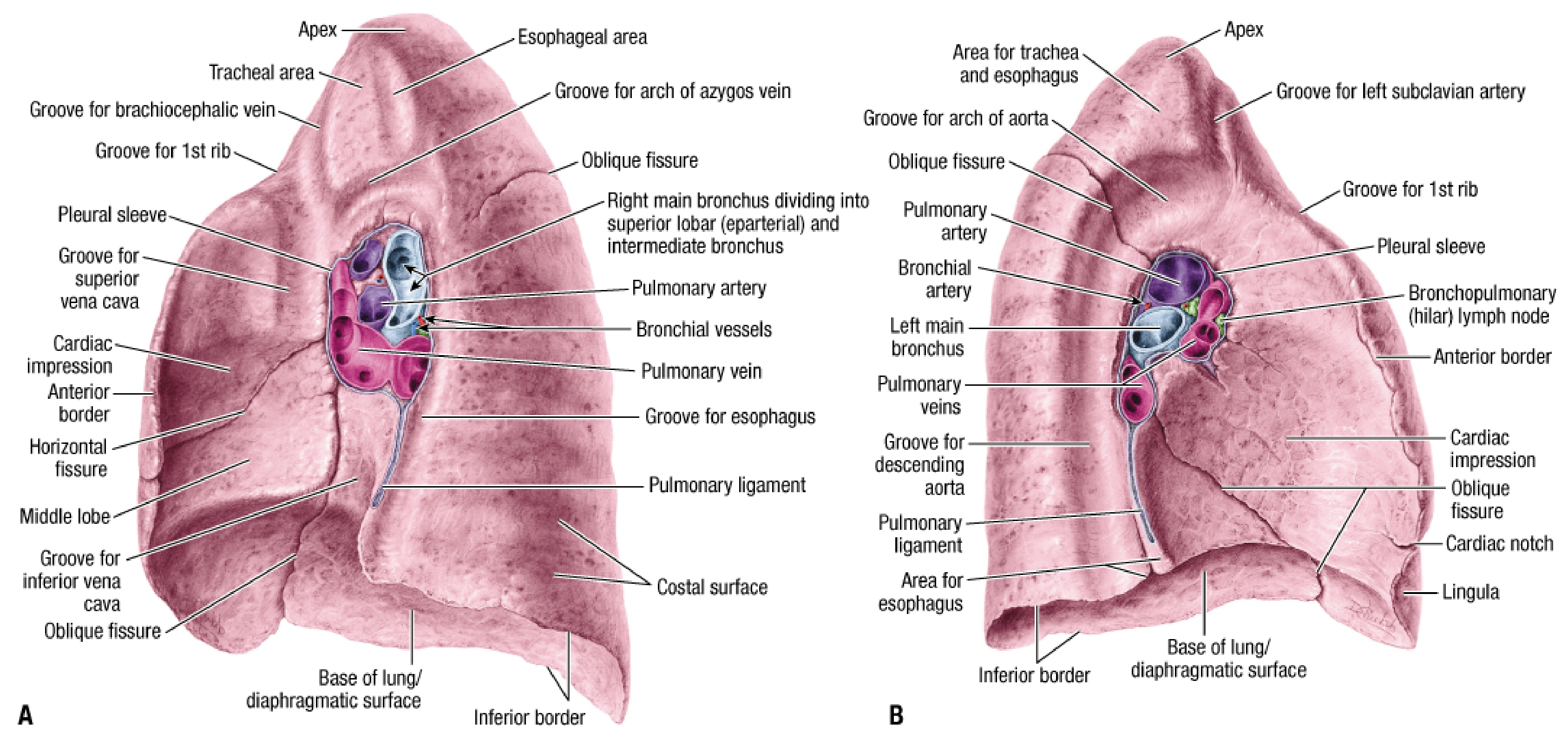
Arrangement at the Hilum
Right hilum:
- Pulmonary veins - most anterior
- Pulmonary artery - intermediate (transverse course)
- Bronchus - most posterior (superolateral course)
- The right phrenic nerve + pericardiophrenic artery are the only longitudinal structures anterior to the root
Left hilum:
- Pulmonary artery - superior to the bronchus (arches over it)
- Pulmonary veins - anterior and inferior
- Bronchus - posterior
- On the left, there is no azygos vein crossing superior to the hilum (unlike the right)
Pulmonary Vessels at the Root
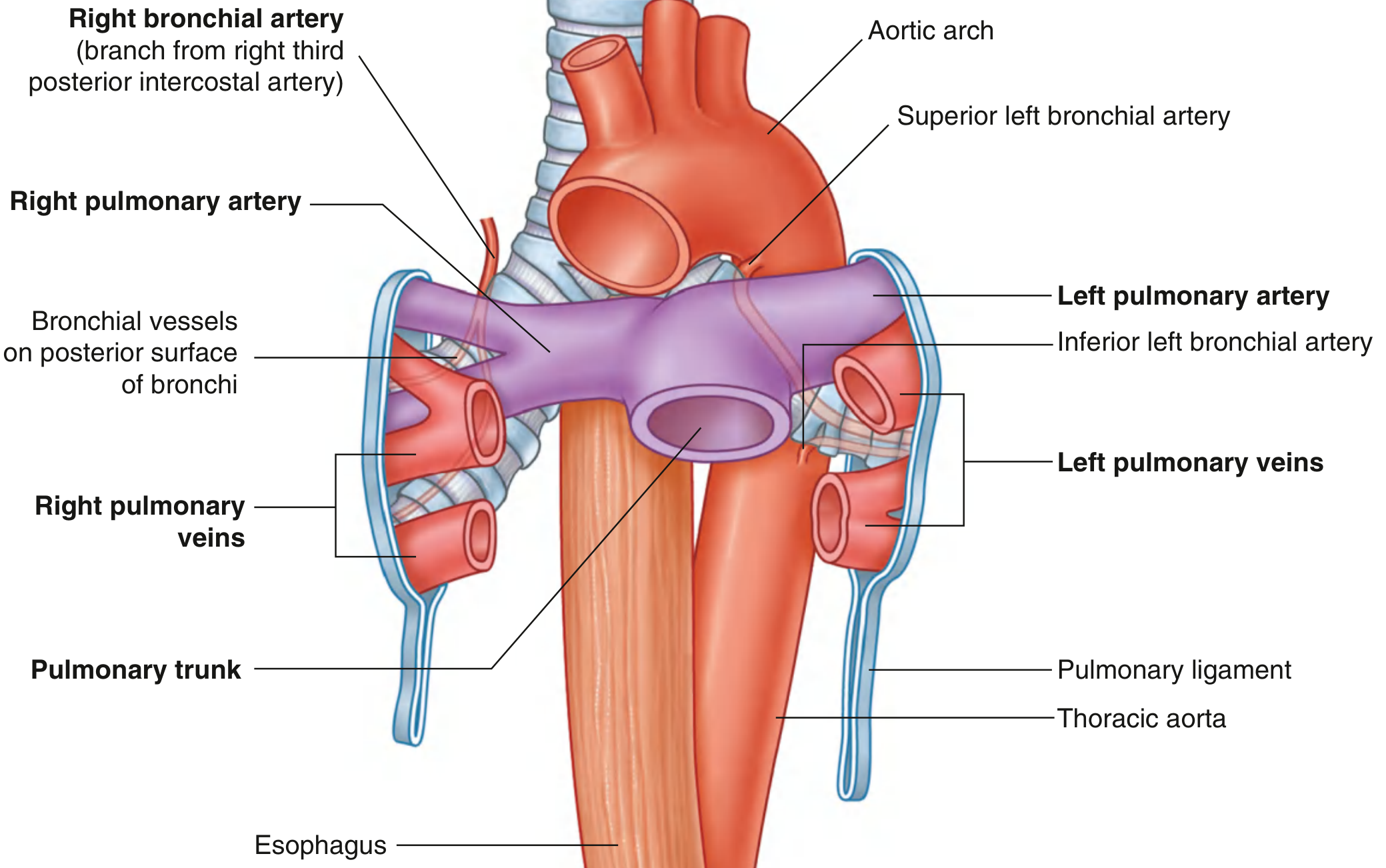
Pulmonary arteries:
- Arise from the pulmonary trunk (at T4/T5, left of midline)
- Right PA: longer, passes horizontally across mediastinum, enters root and gives a large branch to the upper lobe, then continues through hilum
- Left PA: shorter, passes anterior to descending aorta, arches over the left main bronchus
Pulmonary veins:
- Superior and inferior pulmonary veins on each side
- Begin at the hilum, pass through the root, drain directly into the left atrium
Bronchial arteries (nutritive supply):
- Right: single artery from the 3rd posterior intercostal artery
- Left: two arteries from the anterior surface of thoracic aorta - superior (at T5), inferior (below left bronchus)
- Run on the posterior surfaces of the bronchi
Bronchial veins drain into:
- Pulmonary veins or left atrium (inner drainage)
- Azygos vein (right) or hemiazygos/superior intercostal vein (left)
Innervation at the Root
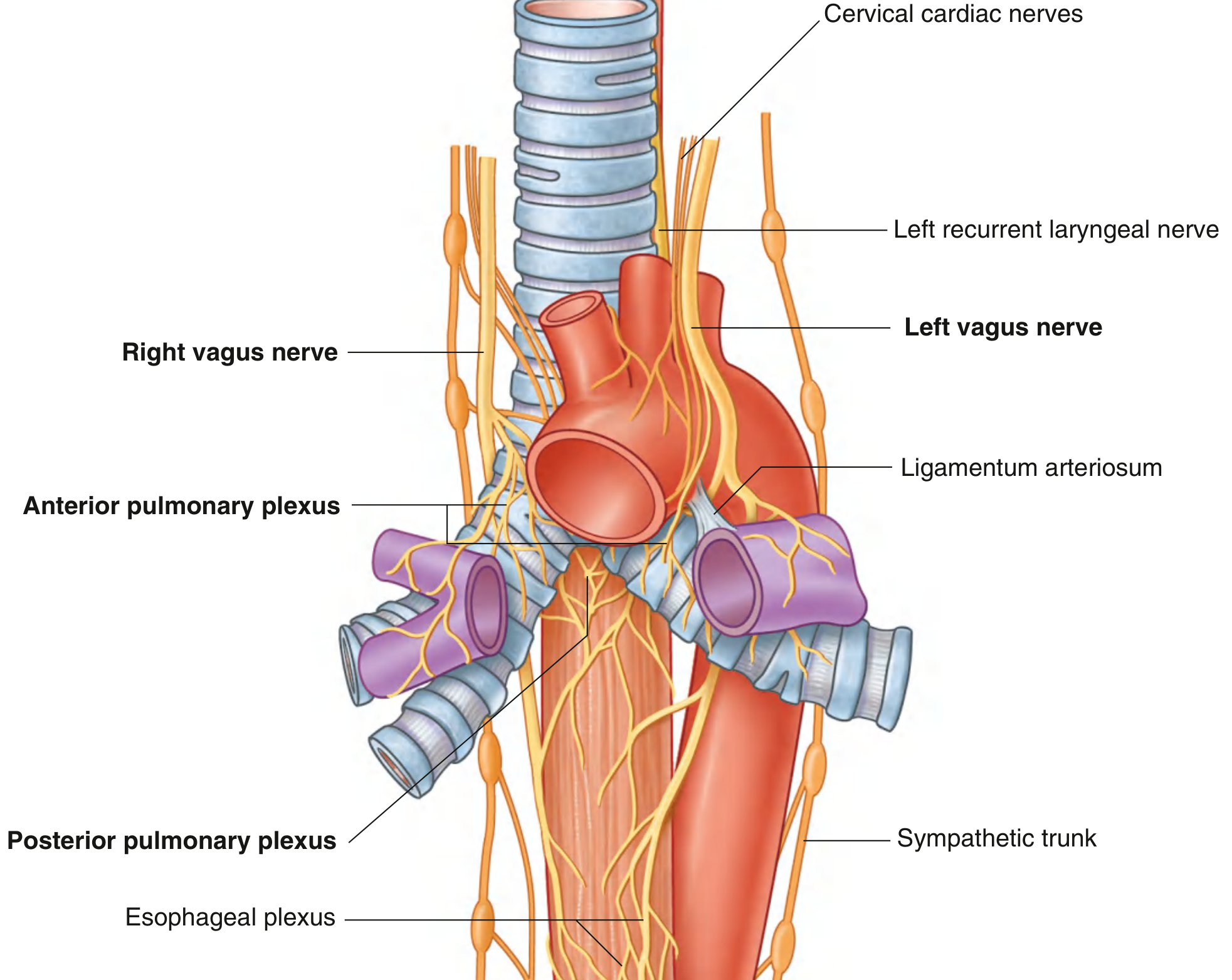
The anterior and posterior pulmonary plexuses lie around the tracheal bifurcation and main bronchi:
- Vagus (parasympathetic): constricts bronchioles, increases secretion
- Sympathetic: dilates bronchioles, decreases secretion
Applied point - Left side danger: The left recurrent laryngeal nerve loops under the arch of the aorta near the ligamentum arteriosum, close to the left pulmonary root. It can be injured during left pneumonectomy if care is not taken when cleaning the pulmonary artery before vascular stapling. - Fischer's Mastery of Surgery, p.2214
Lymphatic Drainage
Superficial (subpleural) and deep lymphatics drain into tracheobronchial nodes around the roots of lobar and main bronchi and along the trachea. Efferent vessels form the right and left bronchomediastinal trunks, which drain into deep veins at the base of the neck (or the right lymphatic trunk/thoracic duct).
Applied Summary - Clinically Important Points
| Point | Applied Significance |
|---|---|
| Right bronchus wider and more vertical | Foreign bodies, aspirated material, misplaced ETTs go right |
| Right upper lobe bronchus arises in the root | Can be missed or inadvertently intubated |
| Carina widening on CXR/CT | Suggests enlarged subcarinal lymph nodes (malignancy, sarcoidosis) |
| Bronchopulmonary segment = independent unit | Allows segmentectomy without damage to adjacent segments |
| Phrenic nerve anterior to root | Only longitudinal structure anterior to the root - must be protected during pulmonary surgery |
| Left recurrent laryngeal nerve near left hilum | Risk of hoarseness/vocal cord palsy with left lung surgery or mediastinal tumors |
| Tracheobronchial lymph nodes at root | Sentinel node for lung and esophageal cancer spread |
| Pulmonary ligament below hilum | Must be incised to mobilize lower lobe; phrenic nerve at risk if cut too superiorly |
Gray's Anatomy for Students (9780323934237) | Fischer's Mastery of Surgery, 8th ed. (9781975176433)
Clinical anatomy
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
I now have all the material needed for a thorough clinical anatomy answer. Let me compile it.
Clinical Anatomy of the Bronchial Tree and Root of the Lung
1. Foreign Body Inhalation
Why the Right Side?
The right main bronchus is wider, shorter, and takes a more vertical/direct course from the trachea. This means:
- Inhaled foreign bodies preferentially lodge in the right main bronchus or its branches
- Distribution: Right main bronchus (~60%) > Left main bronchus (~30%) > Trachea (~3-12%) > Larynx (~1-7%)
- In children (the commonest victims - especially toddlers), food particles are the most frequent culprit
"The object will often lodge in the right mainstem bronchus due to its larger diameter and unique angle." - Cummings Otolaryngology
Ball-Valve (Check-Valve) Mechanism
When a foreign body partially obstructs a bronchus, it creates a ball-valve effect:
- Inspiration: Intrathoracic pressure falls, bronchus dilates slightly - air gets past the foreign body
- Expiration: Intrathoracic pressure rises, bronchus compressed around the foreign body - air cannot escape
- Result: Hyperinflation of the affected lobe/lung on CXR
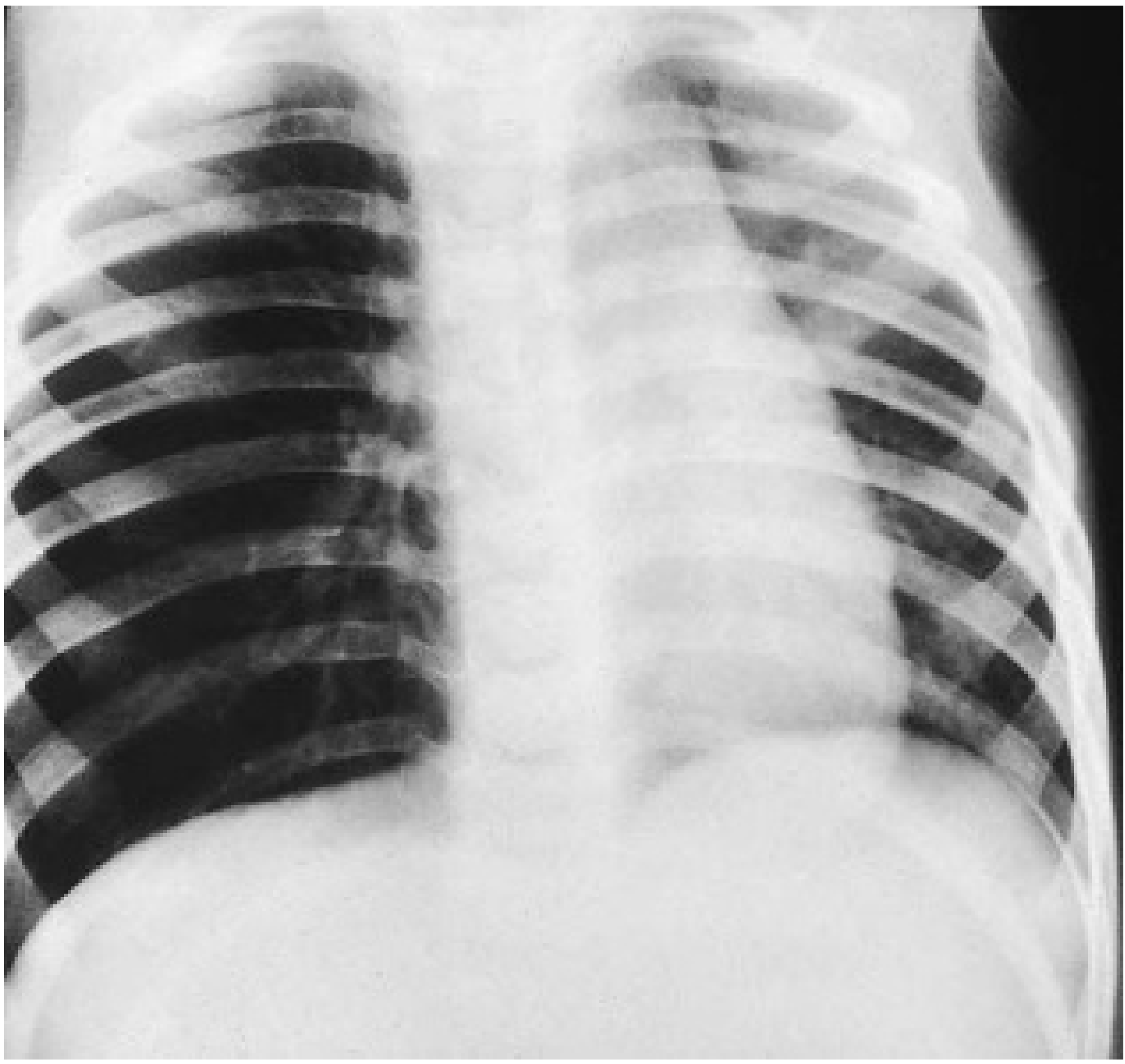
Radiological Findings (Foreign Body)
| Finding | Mechanism |
|---|---|
| Normal CXR (11-26%) | Radiolucent foreign body |
| Hyperinflation | Ball-valve effect (air trapping) |
| Atelectasis | Complete obstruction |
| Mediastinal shift | Towards atelectasis; away from hyperinflation |
| Pneumonia / consolidation | Secondary infection |
| Pneumothorax | Rare complication |
Sensitivity of plain CXR = 73%, specificity = 45% - so a normal film does NOT rule out a foreign body. CT virtual bronchoscopy is highly sensitive. Definitive treatment is rigid bronchoscopy (flexible bronchoscopy is an alternative but less effective for retrieval). - Scott-Brown's Otolaryngology
2. Endobronchial Intubation (Clinical Hazard)
Because the right main bronchus is more vertical and is the natural continuation of the trachea:
- An endotracheal tube passed too deeply will enter the right main bronchus preferentially
- This results in right lung ventilation only - left lung collapse (atelectasis), hypoxia, and pneumothorax risk
How to confirm correct depth:
- Auscultate equal breath sounds bilaterally
- One technique: intentionally advance the ETT into the right main bronchus, then withdraw slowly until breath sounds equalize bilaterally - Morgan & Mikhail's Clinical Anesthesiology
Applied use: In intrabronchial bleeding (hemoptysis), an ETT can be deliberately advanced into the right main bronchus to ventilate the right lung while isolating a bleeding left lung.
3. Aspiration Pneumonia - Segment-Specific Anatomy
The segment in which aspiration pneumonia or a lung abscess develops depends on the patient's posture at the time of aspiration - a direct consequence of gravity acting through the bronchial tree:
| Patient Position | Dependent Segments Affected |
|---|---|
| Supine (recumbent) | Posterior segments of upper lobes (S II); Apical segments of lower lobes (S VI) |
| Upright / semi-recumbent | Basal segments of lower lobes (S VIII, IX, X) |
| Right lateral decubitus | Right-sided segments |
| Left lateral decubitus | Left-sided segments |
"In patients who aspirate in the recumbent position, the commonest sites of involvement are the posterior segments of the upper lobes and the apical segments of the lower lobes." - Fishman's Pulmonary Diseases, p.802
If untreated, aspiration pneumonia can progress to cavitation and lung abscess formation - particularly in the posterior segment of the upper lobe (S II) or the apical segment of the lower lobe (S VI), which are the lowest points in the supine lung.
Postural Drainage - Applied
Because bronchopulmonary segments are anatomically discrete, each can be drained by placing the patient in a specific position so that the segment's bronchus opens downward toward the main bronchus - the basis of physiotherapy/postural drainage for bronchiectasis, lung abscess, and retained secretions.
4. Bronchoscopy and the Carina - Surgical Significance
The carina is the key bronchoscopic landmark. Its angle and sharpness are clinically informative:
- Normal carina: Vertical, sharp, narrow, acute angle
- Widened / splayed carina: Subcarinal lymph node enlargement (malignancy, sarcoidosis, TB, lymphoma) - suggests spread to nodes between the main bronchi
- Involvement of main bronchus within 1.5 cm of carina: Makes the tumor inoperable (within reach of carina resection margin)
- Compression of trachea or paralysis of vocal cord = further signs of non-operability
"Widening of the carina, involvement of the main bronchus within 1.5 cm from the carina, compression of the trachea and paralysis of the vocal cord are the features of non-operability." - S. Das Manual on Clinical Surgery
Bronchoscopy also allows:
- Biopsy of central tumors
- Bronchial washing and brushing for cytology
- Assessment of the distance from the tumour to the carina (resectability)
5. Lung Surgery - Hilar and Root Hazards
Structures at risk during lung surgery
Phrenic nerve:
- Lies anterior to the root on both sides - the only longitudinal structure anterior to the root
- Must be identified and protected during pneumonectomy or lobectomy
- If the pulmonary ligament is divided too superiorly (to mobilize the lower lobe), the inferior pulmonary vein and phrenic nerve are at risk
Left recurrent laryngeal nerve:
- Loops under the arch of the aorta near the ligamentum arteriosum, close to the left pulmonary root
- Risk of injury = left pneumonectomy, especially during cleaning/stapling of the left pulmonary artery
- Injury produces hoarseness and vocal cord palsy
Vagus nerve (right side):
- Lies between the azygos vein and the trachea/left bronchus near the right root
- Can be damaged if the azygos vein is divided carelessly
- Also at risk from lung retraction causing "tenting" of vagal contributions to pulmonary plexuses
Azygos vein:
- Arches over the superior aspect of the right root - landmark in right thoracotomy
- No equivalent on the left (hemiazygos does not cross superiorly)
6. Bronchial Carcinoma - Applied Root Anatomy
| Feature | Clinical Consequence |
|---|---|
| Central tumor compressing main bronchus | Lobar/lung collapse (atelectasis), obstructive pneumonitis |
| Subcarinal node enlargement | Splayed carina on bronchoscopy/CT, dysphagia (esophageal compression) |
| Left recurrent laryngeal nerve palsy | Tumor under arch of aorta |
| Right recurrent laryngeal nerve palsy | Apical tumor below right subclavian artery |
| Phrenic nerve palsy (raised hemidiaphragm) | Tumor invading mediastinum - inoperable |
| Superior vena cava syndrome | Mediastinal/hilar nodal involvement compressing SVC |
| Pancoast tumor (apex) | Invades cervical pleura, brachial plexus, sympathetic chain (Horner's syndrome) |
7. Pulmonary Embolism - Root Vascular Anatomy Relevance
The pulmonary arteries are relatively fragile and carry the entire right heart output. A massive PE lodging at the bifurcation of the pulmonary trunk (saddle embolus) or in the right or left main pulmonary artery within the root causes sudden right heart failure and haemodynamic collapse. CT pulmonary angiography identifies clot at the hilar level - the root anatomy determines the extent of perfusion loss.
Quick-Reference Clinical Anatomy Summary
| Anatomical Fact | Clinical Application |
|---|---|
| Right bronchus wider + vertical | Foreign body, inadvertent ETT placement goes right |
| Ball-valve partial obstruction | Hyperinflation on CXR |
| Carina widened | Subcarinal nodes enlarged |
| Carina <1.5 cm from tumor | Inoperable bronchial carcinoma |
| Supine aspiration → posterior S II + apical S VI | Segment for aspiration pneumonia/abscess |
| Each segment has own bronchus | Segmentectomy possible; postural drainage is segment-directed |
| Phrenic nerve anterior to root | Protected during lung surgery |
| Left recurrent laryngeal nerve near left root | Hoarseness after left thoracic surgery / aortic/left hilar tumors |
| Azygos vein arches over right root | Surgical landmark; no equivalent on left |
| Pulmonary veins most anterior in hilum | Identified first in surgical dissection |
Sources: Gray's Anatomy for Students | Fischer's Mastery of Surgery, 8th ed. | S. Das Manual on Clinical Surgery | Scott-Brown's Otolaryngology | Fishman's Pulmonary Diseases | Cummings Otolaryngology | Morgan & Mikhail's Clinical Anesthesiology
This is a shared conversation. Sign in to Orris to start your own chat.