Functions and connections of internal capsule physiology for 8 marks mbbs 1st year
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from the textbooks. Let me compile the complete 8-mark answer.
Internal Capsule: Functions and Connections
(MBBS 1st Year Physiology - 8 Marks)
Definition and Position
The internal capsule is a compact lamina (band) of white matter representing the largest projection fiber tract in the brain. It contains both afferent (ascending) and efferent (descending) nerve fibers passing to and from the cerebral cortex, brainstem, and spinal cord.
Location: It lies medial to the lenticular nucleus (putamen + globus pallidus) and lateral to the caudate nucleus and thalamus. On a horizontal section, it appears V-shaped (or like two arrowheads pointing inward), with its convexity directed medially.
- Caudate nucleus and thalamus are always medial to the internal capsule
- Globus pallidus and putamen are always lateral to the internal capsule
Parts / Segments
The internal capsule has five segments (from anterior to posterior):
| Part | Location |
|---|---|
| 1. Anterior limb | Between caudate nucleus (medial) and lentiform nucleus (lateral) |
| 2. Genu | The bend/knee - between anterior and posterior limbs |
| 3. Posterior limb | Between thalamus (medial) and lentiform nucleus (lateral) |
| 4. Retrolenticular segment | Behind the lentiform nucleus |
| 5. Sublenticular segment | Below the lentiform nucleus |
The internal capsule continues rostrally as the corona radiata and caudally as the cerebral peduncles.
Fibers Carried (Connections)
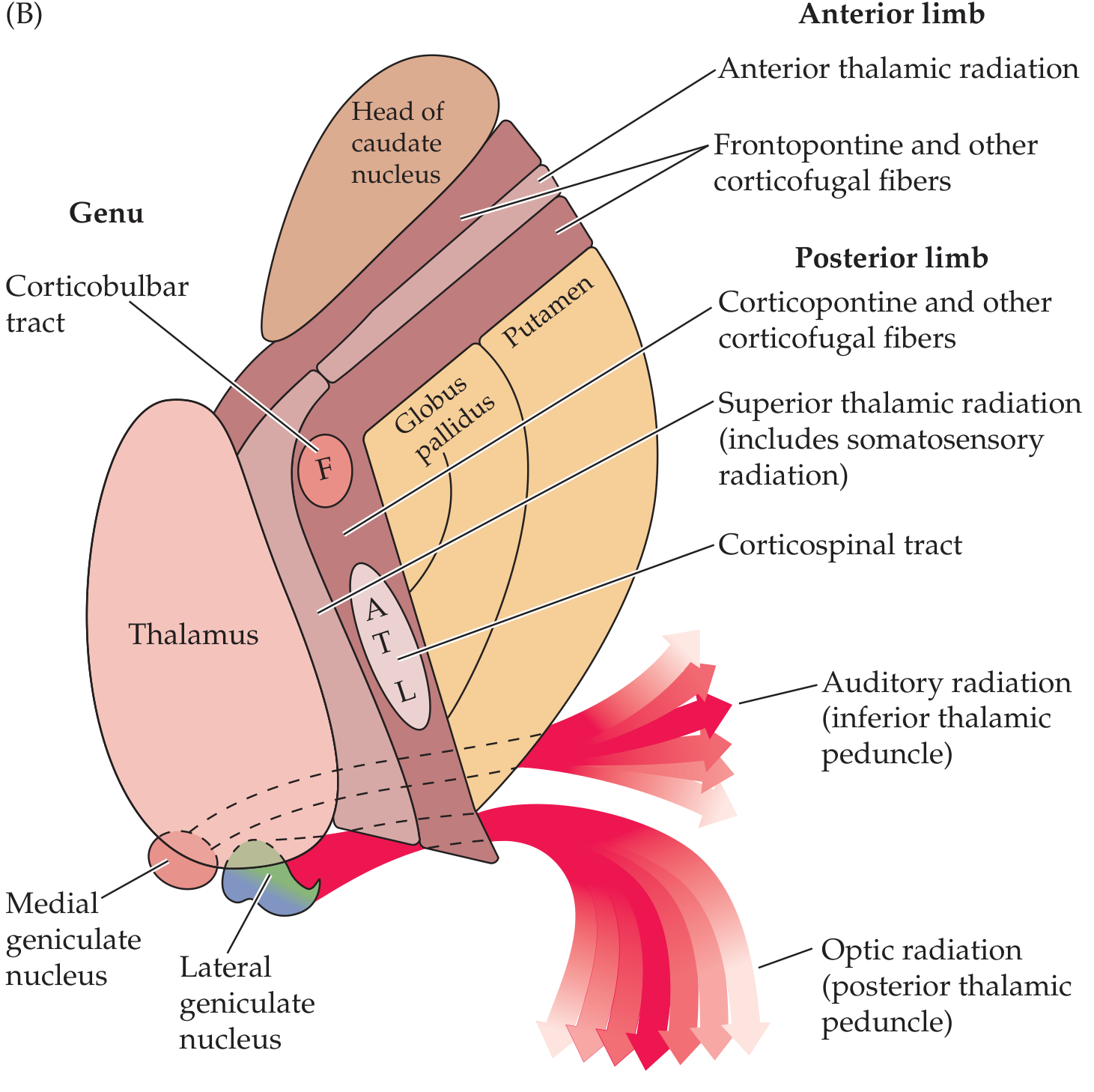
1. Anterior Limb
- Frontopontine fibers (corticopontine from frontal lobe to pons)
- Anterior thalamic radiation - thalamocortical and corticothalamic fibers connecting the frontal lobe to the thalamus (feedback loop)
- Caudate-putaminal fibers
2. Genu
- Corticobulbar (corticonuclear) fibers - from motor cortex to motor nuclei of cranial nerves in the brainstem
- Corticoreticular fibers (from motor cortex to brainstem reticular formation)
- The face is represented at the genu - "Face at the knee"
3. Posterior Limb
- Corticospinal tract (most important efferent pathway)
- Somatotopically arranged (anterior to posterior): Face (F) > Arm (A) > Trunk (T) > Leg (L)
- Face fibers most anterior; leg fibers most posterior
- Superior thalamic radiation (somatosensory radiation) - thalamocortical fibers carrying sensory information from ventroposterolateral/ventroposteromedial nuclei of thalamus to parietal sensory cortex
- Corticorubral fibers (cortex to red nucleus)
- Additional corticopontine fibers
4. Retrolenticular Segment
- Optic (visual) radiation - geniculocalcarine tract from lateral geniculate body to primary visual cortex (area 17)
- Corticotectal, corticonigral, and corticotegmental fibers
- Posterior thalamic radiation
5. Sublenticular Segment
- Auditory radiation - from medial geniculate body to primary auditory cortex (area 41/42) via inferior thalamic peduncle
- Temporopontine fibers
Functions
| Segment | Key Function |
|---|---|
| Anterior limb | Frontal lobe - thalamus communication; motor planning and cognitive relay |
| Genu | Voluntary control of face, tongue, and throat muscles (cranial nerve motor control) |
| Posterior limb | Voluntary movement of limbs and trunk (corticospinal); conscious sensation (thalamocortical sensory) |
| Retrolenticular | Visual transmission |
| Sublenticular | Auditory transmission |
Blood Supply
| Segment | Artery |
|---|---|
| Anterior limb | Recurrent artery of Heubner (branch of anterior cerebral artery) |
| Genu + middle/inferior posterior limb | Anterior choroidal artery |
| Superior anterior and posterior limb | Lenticulostriate arteries (branches of middle cerebral artery) |
The lenticulostriate arteries are prone to hypertensive rupture, making the internal capsule a common site of hemorrhagic stroke.
Clinical Importance (Effects of Lesion)
Because fibers are densely packed, even a small lesion causes widespread deficits on the contralateral side:
- Contralateral hemiplegia - damage to corticospinal and corticobulbar fibers (upper motor neuron lesion with spasticity, hyperreflexia, Babinski sign)
- Contralateral hemisensory loss - damage to sensory thalamic radiations
- If retrolenticular lesion: contralateral homonymous hemianopia (visual field loss)
- Capsular genu syndrome - corticobulbar fiber involvement causes contralateral facial and lingual weakness with only mild limb involvement
- Internal capsule hemorrhage (hypertensive bleed into lenticulostriate territory): sudden contralateral hemiplegia + hemisensory loss + hemianopia = "capsular triad"
- Decoricate rigidity can follow severe capsular lesions
Summary Table for Quick Revision
| Segment | Fibers |
|---|---|
| Anterior limb | Frontopontine + Anterior thalamic radiation |
| Genu | Corticobulbar (face) + Corticoreticular |
| Posterior limb | Corticospinal (arm/trunk/leg) + Superior thalamic radiation (sensory) |
| Retrolenticular | Visual (optic) radiation |
| Sublenticular | Auditory radiation |
Sources: Localization in Clinical Neurology, 8e | Neuroanatomy through Clinical Cases, 3rd Ed
This is a shared conversation. Sign in to Orris to start your own chat.