Myloma in medical terms in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"multiple myeloma"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Searching Images
multiple myeloma plasma cells bone marrow histology
Reading File
Loading Image
Loading Image
I now have comprehensive information to deliver a detailed, well-structured answer. Let me compile everything:
Multiple Myeloma — Comprehensive Medical Overview
Definition
Multiple myeloma (MM) is a malignant neoplasm of plasma cells (terminally differentiated B lymphocytes) that proliferates primarily in the bone marrow. It is the most common primary malignant tumor of bone and accounts for approximately 1.3% of all malignancies and 15% of all hematological malignancies. About 30,000 new cases are diagnosed annually in the United States.
Epidemiology
| Feature | Detail |
|---|---|
| Median age at diagnosis | 62–70 years |
| Sex | Slight male predominance (up to 2:1) |
| Race | More frequent in people of African descent (reason unknown) |
| Age <40 years | Rare (~3% of cases) |
Pathogenesis & Molecular Biology
Myeloma arises from a single clonal plasma cell that undergoes uncontrolled proliferation, driven by several mechanisms:
Chromosomal Abnormalities
- Translocations involving the IgH locus (chromosome 14) fuse it to oncogenes like cyclin D1 (t(11;14)) or cyclin D3 — dysregulation of D cyclins drives cell proliferation
- Hyperdiploidy (trisomies of odd-numbered chromosomes) → associated with better prognosis
- Hypodiploidy → associated with adverse prognosis
- Late-stage: translocations involving MYC — seen in aggressive disease
Key Growth Factor
- Interleukin-6 (IL-6), produced by bone marrow fibroblasts and macrophages, is the principal cytokine supporting myeloma cell proliferation
Bone Destruction Mechanism
- Myeloma cells upregulate RANKL (receptor activator of NF-κB ligand) expression on marrow stromal cells → activates osteoclasts → bone resorption
- Tumor cells simultaneously release inhibitors of osteoblast function
- Net result: uncoupled bone remodeling → lytic lesions, hypercalcemia, pathologic fractures
Immunoglobulin Production (M Protein / Paraprotein)
| Immunoglobulin Type | Frequency |
|---|---|
| IgG | ~60% (most common) |
| IgA | 20–25% |
| Light chains only (κ or λ) | ~20% |
| IgM, IgD, IgE | Rare |
| Non-secretory (no M protein) | ~1% |
Bence Jones proteins = free immunoglobulin light chains excreted in the urine — a hallmark of myeloma.
Clinical Features — The "CRAB" Criteria
The major end-organ damage defining symptomatic myeloma is remembered as CRAB:
| Letter | Feature | Mechanism |
|---|---|---|
| C | Hypercalcemia | Osteoclast activation → bone resorption |
| R | Renal insufficiency | Light chain cast nephropathy, amyloidosis, hypercalcemia |
| A | Anemia | Marrow replacement by plasma cells → normochromic, normocytic anemia |
| B | Bone lesions | Lytic lesions, pathologic fractures, bone pain |
Additional Features
- Bone pain and backache — most common presenting symptom
- Pathologic fractures — especially vertebral column (affects ~50% of patients at some stage) and femur
- Recurrent bacterial infections — due to suppressed normal immunoglobulin production (functional hypogammaglobulinemia despite high total immunoglobulin)
- Neurologic symptoms — spinal cord compression, confusion/lethargy from hypercalcemia
- Rouleaux formation on blood film — due to high paraprotein levels causing red cell aggregation
- Amyloidosis (AL type) — occurs in ~20% of patients; involves kidneys, heart, tongue, peripheral nerves
Morphology & Pathology
Bone Lesions (Gross)
- Punched-out lytic defects 1–4 cm in diameter throughout the skeleton
- Most common sites: vertebral column, ribs, skull, pelvis, femur, clavicle, scapula
- Arise in medullary cavity → erode cancellous bone → destroy cortex
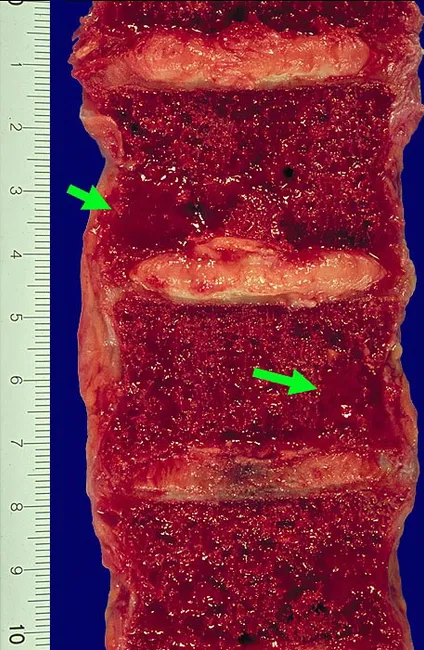
Gross specimen: vertebral bodies showing red-brown, soft-tissue lytic lesions replacing normal bone marrow — characteristic of plasma cell myeloma of the axial skeleton.
Bone Marrow Histology
- Plasma cells >30% of marrow cellularity (diagnostic threshold)
- Cells may resemble normal plasma cells or show abnormal features: prominent nucleoli, cytoplasmic inclusions (Russell bodies = condensed immunoglobulin in dilated ER)
- Late disease: spread to viscera, soft tissue; rarely a leukemic picture
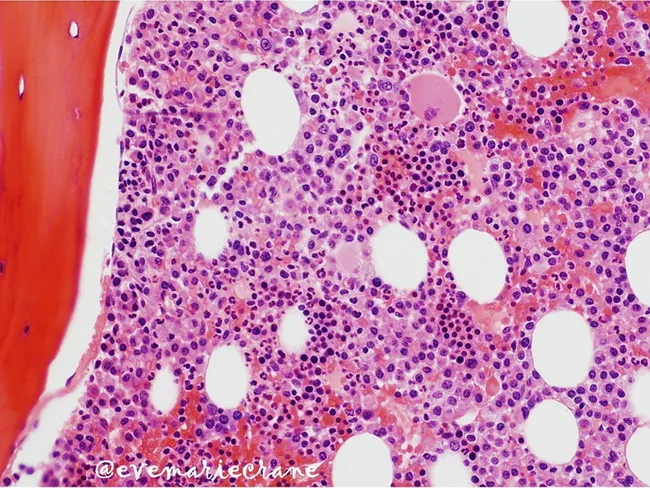
H&E bone marrow biopsy: clonal plasma cells with hyperchromatic nuclei, clumped chromatin, and moderate cytoplasm progressively replacing normal marrow.
Myeloma Kidney
- Obstructive casts (Bence Jones proteins + albumin + tubular proteins) in distal convoluted tubules and collecting ducts → surrounded by multinucleate macrophage giant cells
- AL amyloidosis depositing in glomeruli and vessel walls
- Metastatic calcification from hypercalcemia
- Bacterial pyelonephritis (secondary to hypogammaglobulinemia)
Radiological Features
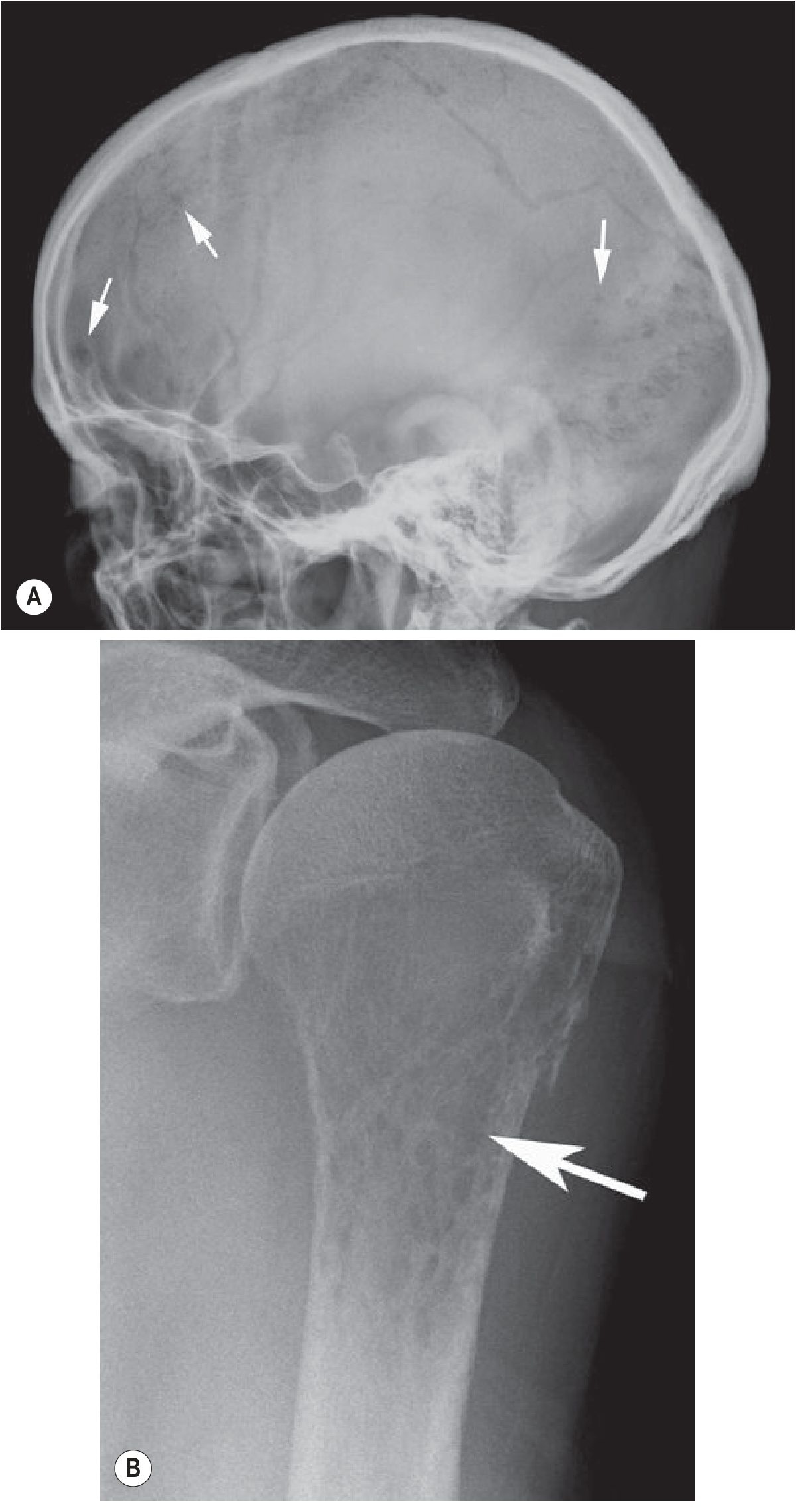
From Grainger & Allison's Diagnostic Radiology. (A) Lateral skull X-ray showing classic "peppered" lytic lesions. (B) Moth-eaten destruction of the proximal humerus.
| Modality | Findings |
|---|---|
| Plain X-ray | Multiple "punched-out" lytic lesions; diffuse osteopenia; vertebral compression fractures |
| CT (whole-body low-dose) | More sensitive than X-ray; focal soft-tissue density lesions; endosteal scalloping; cortical destruction |
| PET/CT | Most sensitive for active lesion detection and treatment response |
| MRI | Best for bone marrow involvement; 5 patterns: normal, focal, diffuse, variegated, combined; discs appear hyperintense compared to vertebral bodies in diffuse disease |
| Sclerotic lesions | Rare; seen in POEMS syndrome (osteosclerotic myeloma) |
Diagnostic Criteria
Spectrum of Plasma Cell Disorders
| Condition | M-protein | Marrow Plasma Cells | End-organ Damage (CRAB) |
|---|---|---|---|
| MGUS (Monoclonal Gammopathy of Undetermined Significance) | <30 g/L | <10% | None |
| Smoldering Myeloma | ≥30 g/L | ≥10% | None |
| Plasma Cell Myeloma (Active) | Present (any level) | Clonal plasma cells present | Present (CRAB + or myeloma-defining events) |
Diagnosis Requires:
- M protein in serum or urine (serum protein electrophoresis + immunofixation)
- Clonal bone marrow plasma cells (biopsy/aspirate)
- End-organ damage (CRAB criteria) OR myeloma-defining events (e.g., marrow plasmacytosis ≥60%, serum FLC ratio ≥100, >1 focal MRI lesion)
Immunophenotype
- Positive: CD38, CD138 (hallmark plasma cell markers)
- Positive (aberrant): CD56, CD117
- Negative (abnormally lost): CD19, CD20
- Light chain restriction (κ or λ) confirms clonality
Laboratory Investigations
| Test | Expected Finding |
|---|---|
| Serum protein electrophoresis (SPEP) | M-spike (monoclonal band) |
| Serum immunofixation | Identifies M-protein isotype (IgG, IgA, etc.) |
| Urine protein electrophoresis (UPEP) | Bence Jones proteinuria |
| Serum free light chains (FLC) | Elevated κ or λ; abnormal κ:λ ratio |
| CBC | Normochromic normocytic anemia; rouleaux on smear |
| Serum calcium | Elevated (hypercalcemia) |
| Creatinine | Elevated (renal insufficiency) |
| Serum β2-microglobulin | Elevated (used for ISS staging) |
| Serum albumin | Decreased (used for ISS staging) |
| LDH | Elevated in aggressive disease (R-ISS staging) |
| Bone marrow biopsy | >10% clonal plasma cells; cytogenetics/FISH |
Staging
International Staging System (ISS)
| Stage | Criteria | Median Survival |
|---|---|---|
| I | β2-microglobulin <3.5 mg/L + Albumin ≥3.5 g/dL | ~62 months |
| II | Neither I nor III | ~44 months |
| III | β2-microglobulin ≥5.5 mg/L | ~29 months |
Revised ISS (R-ISS) also incorporates:
- High-risk cytogenetics: del(17p), t(4;14), t(14;16)
- Elevated LDH
Treatment
Induction Therapy (Transplant-Eligible)
- VRd regimen: Bortezomib (proteasome inhibitor) + Lenalidomide (immunomodulatory agent/IMiD) + Dexamethasone
- Daratumumab (anti-CD38 monoclonal antibody) increasingly added (Dara-VRd)
Autologous Stem Cell Transplantation (ASCT)
- Standard of care for eligible patients (generally age <70, good performance status)
- High-dose melphalan conditioning followed by autologous hematopoietic cell rescue
- Single ASCT standard; tandem ASCT in select cases or at relapse (if prior response >1 year)
Maintenance Therapy
- Lenalidomide post-ASCT is standard
- Bortezomib for high-risk cytogenetics
Non-Transplant Eligible
- VRd or DaraRd (Daratumumab + Lenalidomide + Dexamethasone)
Relapsed/Refractory Myeloma
- Pomalidomide, carfilzomib, ixazomib (next-gen IMiDs and proteasome inhibitors)
- Daratumumab, elotuzumab, isatuximab (monoclonal antibodies)
- CAR-T cell therapy (e.g., Idecabtagene vicleucel targeting BCMA) — approved for late-line therapy
- Bispecific antibodies (e.g., Teclistamab, targeting BCMA × CD3) — recent approvals for third-line and beyond
Recent Evidence Note: A 2024 meta-analysis (PMID 39551604) compared CAR-T vs. bispecific antibodies as third-line+ treatment — both show strong activity; selection depends on patient fitness and logistics.
Mechanism of Proteasome Inhibitors
Myeloma cells accumulate misfolded immunoglobulin chains; proteasome inhibitors (bortezomib, carfilzomib) block degradation of these misfolded proteins → activate apoptotic pathways → selective myeloma cell death.
Supportive Care
- Bisphosphonates (zoledronic acid, pamidronate) — prevent skeletal-related events
- G-CSF, EPO — manage cytopenias
- IVIG — for recurrent infections
- Plasmapheresis — for hyperviscosity syndrome
- Radiation — for localized painful lesions
Prognosis
- Median survival: approximately 5 years with modern therapy
- Untreated patients with multiple bony lesions: survival rarely >6–12 months
- Smoldering myeloma: may not require treatment for many years
- Favorable factors: hyperdiploid cytogenetics, t(11;14), low ISS stage, good performance status
- Adverse factors: del(17p), t(4;14), t(14;16), elevated LDH, high β2-microglobulin, plasmablastic morphology
- Cure has not yet been consistently achieved, but outcomes continue to improve with combination immunotherapy and cellular therapies
Related Plasma Cell Disorders
| Disorder | Key Feature |
|---|---|
| Solitary plasmacytoma | Single bone or extramedullary lesion; no systemic M protein |
| MGUS | Pre-malignant; 1% per year risk of progression to myeloma |
| Waldenström macroglobulinemia | IgM-secreting lymphoplasmacytic lymphoma |
| AL amyloidosis | Light chain deposition in organs (heart, kidney, liver) |
| POEMS syndrome | Polyneuropathy, Organomegaly, Endocrinopathy, M protein, Skin changes; sclerotic bone lesions |
Sources: Robbins & Kumar Basic Pathology, p. 422 | Grainger & Allison's Diagnostic Radiology | Henry's Clinical Diagnosis and Management by Laboratory Methods | Goldman-Cecil Medicine | Robbins, Cotran & Kumar Pathologic Basis of Disease
Serum protein electrophoresis
Reading File
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.