hemangioma in lower limb muscle usg
Reading File
Finding Sources
Finding Sources
Searching PubMed
intramuscular hemangioma lower limb ultrasound
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
intramuscular hemangioma lower limb ultrasound sonography features phlebolith
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC7905120
I now have comprehensive information to give a detailed answer. Let me compile this.
Intramuscular Hemangioma of the Lower Limb - Ultrasound (USG)
Overview
Intramuscular hemangioma (IMH) is a benign vascular neoplasm arising within skeletal muscle. About 50% occur in the lower limbs, with the thigh (quadriceps, adductors) being the most common site, followed by the calf (gastrocnemius). The lesion is commoner in younger patients - 80-90% present before age 30, with a male:female ratio of 1:2.
Ultrasound Features
B-Mode (Greyscale)
| Feature | Description |
|---|---|
| Echogenicity | Most commonly hyperechoic (most frequent finding); can be heterogeneous or hypoechoic depending on lesion composition |
| Margins | Typically ill-defined / poorly circumscribed - infiltrates between muscle fascicles |
| Internal architecture | Complex mass with serpentine/tubular vascular channels visible within it |
| Compressibility | Venous channels may be partially compressible on probe pressure |
| Phleboliths | Appear as echogenic foci with posterior acoustic shadowing - highly specific; seen in ~25% of cases |
| Fat component | Echogenic foci from intralesional fat (fatty replacement of muscle fibers) |
| Muscle atrophy | Surrounding muscle may show loss of normal fibrillar echotexture in chronic lesions |
Color Doppler / Power Doppler
| Feature | Description |
|---|---|
| Venous type | Low-flow or no-flow channels; augmentation on distal compression |
| Arteriovenous (AV) type | High-flow pattern with arterial waveforms, low resistance; prominent Doppler signal |
| Cavernous type | Variable flow; large sinusoidal spaces, sometimes no detectable flow |
| Capillary type | Diffuse low-velocity flow throughout the mass |
A key USG finding: size increases when the limb is placed in a dependent position (due to venous engorgement) - clinically confirmatory.
Limitations of USG
- Superficial lesions: USG is adequate and reliable
- Deep-seated lesions (common in thigh): USG cannot define the full extent of the lesion - may underestimate involvement
- USG does NOT reliably identify all pathognomonic features of IMH
- MRI is the imaging modality of choice - superior for extent, tissue characterization, and surgical planning
Comparison of Imaging Modalities
| Modality | Key Finding |
|---|---|
| X-ray | Calcified phleboliths (25% of cases); may be normal |
| USG | Hyperechoic/heterogeneous mass, vascular channels, phleboliths with shadowing, Doppler flow |
| CT | Poorly defined lesion isodense to muscle; phleboliths well seen; variable contrast enhancement |
| MRI (gold standard) | T1: high signal (fat + subacute blood); T2: marked hyperintensity (blood-filled channels); poorly circumscribed; "lobulated" appearance |
Clinical Correlation
- Painful episodes associated with warmth and swelling, worsening with physical activity
- Symptoms may mimic a muscle strain or deep venous thrombosis
- Phleboliths on X-ray + typical USG findings can narrow the diagnosis considerably
- High-frequency ultrasound has an 87% concordance with pathological diagnosis
- Recommended workflow: if abnormal Doppler flow or mass found on USG → proceed to MRI for definitive characterization
Differential Diagnosis on USG
- Lipoma - uniformly hyperechoic, compressible, no Doppler flow
- Soft tissue sarcoma - irregular, infiltrative, internal necrosis, aggressive Doppler; suspect if rapidly enlarging
- Vascular malformation (venous) - low-flow, compressible, phleboliths, no arterial waveforms
- Myositis ossificans - peripheral calcification with "zoning" pattern, history of trauma
- Abscess - hypoechoic, posterior enhancement, clinical features of infection
Key Teaching Points
- Phlebolith (echogenic focus + posterior shadowing) in a lower limb muscle mass = near-pathognomonic for hemangioma/vascular malformation
- Doppler flow pattern distinguishes AV (high-flow) from venous/cavernous (low/no flow) types
- USG is the first-line tool for superficial lesions; MRI is mandatory for deep/large lesions before surgical planning
- Intralesional fat creates echogenic foci - corresponds to T1 high signal on MRI
- Always look for positional size change (increases dependent, decreases elevated) as a confirmatory clinical sign
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 1260 (Vascular Lesions - Intramuscular Hemangioma)
- PMC Imaging of intramuscular haemangiomas (PMID 32488279)
- PMC Intramuscular Hemangiomas review
- Frontiers in Surgery 2025 - IMH case & literature review
usg images
Searching the Web
intramuscular hemangioma lower limb ultrasound images sonography
Searching the Web
intramuscular hemangioma thigh calf ultrasound color doppler images radiology
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here are USG images of intramuscular hemangioma in the lower limb, annotated with their key findings:
USG Images - Intramuscular Hemangioma, Lower Limb
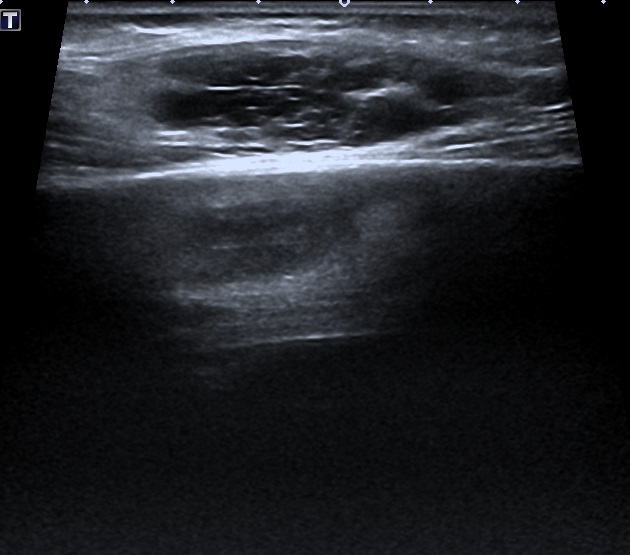
1. Greyscale USG - Hypoechoic intramuscular mass (flexor hallucis longus, lower leg)
(Oval, macro-lobulated, hypoechoic mass with echogenic trabeculae - lower leg)

Key features: Ill-defined, heterogeneous hypoechoic mass within muscle. The arrow points to echogenic internal trabeculae representing fibrous septa between vascular channels. Poorly circumscribed margins blending with surrounding muscle.
2. Color Doppler USG - High-flow AV-type hemangioma (superficial lower limb)
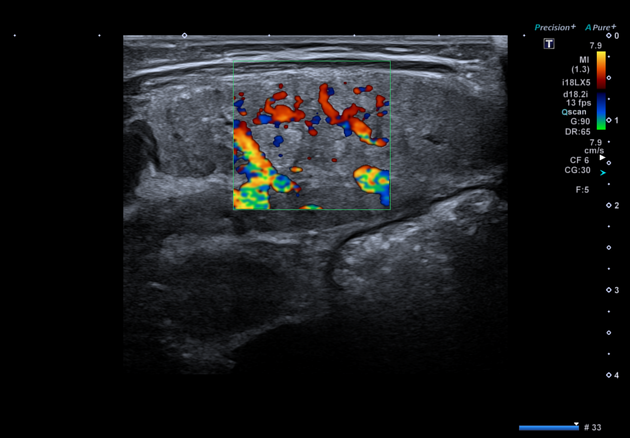
Key features: Prominent color Doppler signal filling the lesion. Mixed red (towards probe) and blue (away) channels indicate the tortuous, high-density vascular network. This pattern is typical of AV or capillary-type hemangioma with active arterial flow.
3. Color Doppler USG - Intramuscular hemangioma with extensive vascular channels (deep thigh/lower limb)

Key features: Large ill-defined intramuscular lesion with chaotic, high-density Doppler signal throughout. The serpiginous course of color-filled channels represents the dilated, tortuous vascular spaces. Background muscle shows echogenic fat replacement.
4. Greyscale USG - Cavernous hemangioma, left calf (Radiopaedia)

Key features: Labelled "LT CALF" - heterogeneous mass with multiple anechoic/hypoechoic spaces (blood-filled sinusoidal channels). Calipers mark the lesion (~1.3 x 1.0 cm). Poorly defined margins merging with surrounding gastrocnemius muscle.
5. Greyscale USG - Intramuscular hemangioma with phlebolith (lower limb)
Key features: Heterogeneous intramuscular mass with internal echogenic focus and posterior acoustic shadowing - this is a phlebolith (calcified thrombus), a near-pathognomonic finding for hemangioma/vascular malformation. Posterior shadowing is the key clue.
6. Greyscale USG - Superficial cavernous hemangioma with vascular channels and phlebolith

Key features: Round, relatively well-defined mass showing internal tubular/serpiginous anechoic vascular channels. Echogenic focus with posterior shadow (phlebolith) visible. Subcutaneous/superficial location.
Summary of What to Look For on USG
| Finding | Significance |
|---|---|
| Ill-defined heterogeneous mass within muscle | Typical of IMH - infiltrates fascicles |
| Hypoechoic/anechoic tubular channels | Blood-filled vascular sinuses |
| Echogenic foci (no shadow) | Intralesional fat |
| Echogenic focus + posterior shadow | Phlebolith - near-pathognomonic |
| High-density color Doppler signal | AV or capillary type (high-flow) |
| Low/no Doppler flow, compressible | Venous/cavernous type (low-flow) |
| Size increases on dependency | Venous engorgement - confirmatory sign |
This is a shared conversation. Sign in to Orris to start your own chat.