Second Generation Antihistaminics* and Conventional Antihistaminics - compare and contrast; Non-Sedative Antihistaminics - enumerate, advantages, two indications precaution 2. H1 antihistaminics* - uses*, adverse effects* precautions 3. Antihistaminics - classify, moa adv effect uses precautions 2mbbs pharmacology kdt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material. Let me compile the complete answer for this 2nd MBBS pharmacology question:
Antihistaminics - Complete 2nd MBBS Pharmacology (KDT-Pattern)
1. CLASSIFICATION OF ANTIHISTAMINICS
H1 Antihistaminics (H1 Blockers)
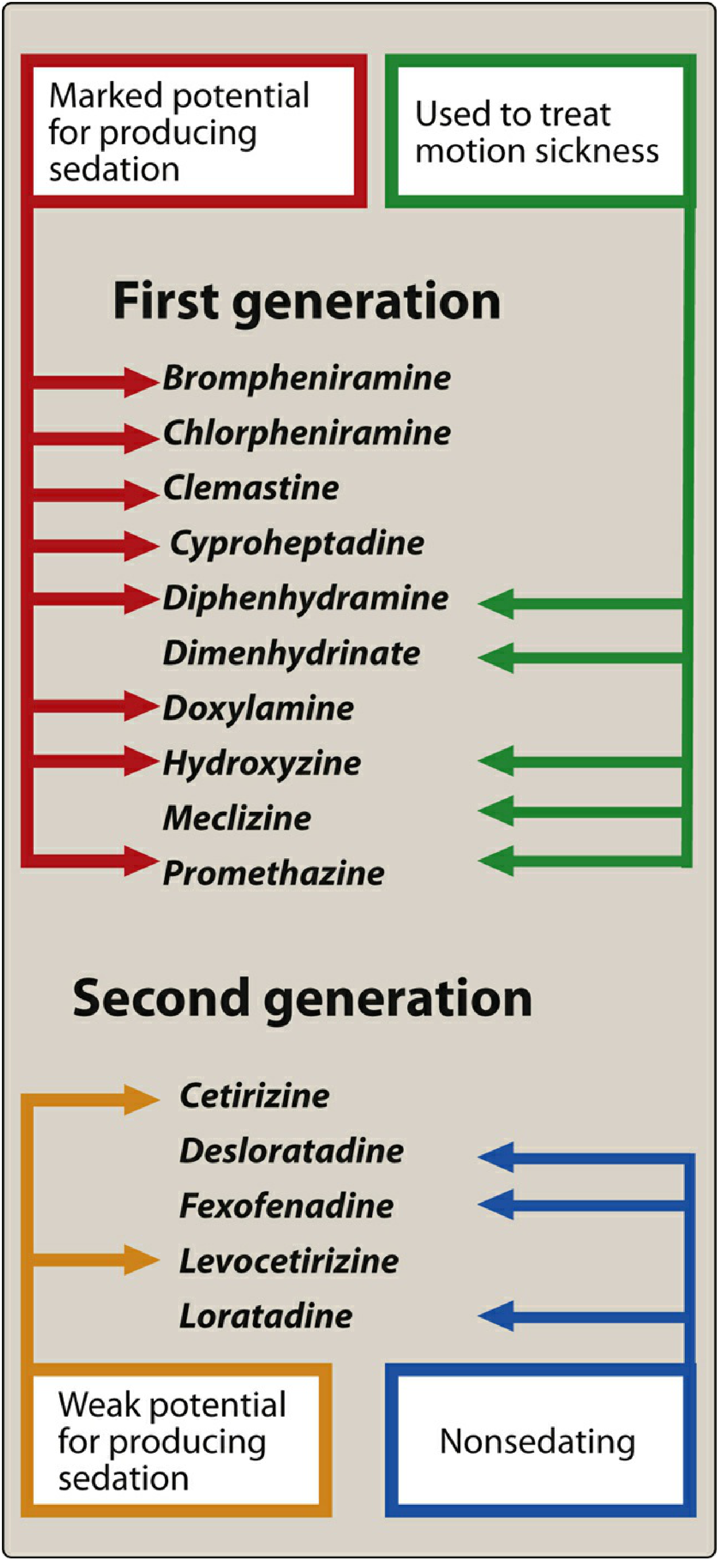
Generation I - Conventional / First Generation (Sedating)
| Chemical Class | Examples |
|---|---|
| Ethanolamines | Diphenhydramine, Dimenhydrinate, Doxylamine |
| Ethylenediamines | Tripelennamine, Mepyramine |
| Alkylamines | Chlorpheniramine, Brompheniramine |
| Piperazines | Hydroxyzine, Cyclizine, Meclizine |
| Phenothiazines | Promethazine |
| Others | Cyproheptadine, Clemastine |
Generation II - Non-Sedating / Second Generation
| Drug | Notes |
|---|---|
| Loratadine | Truly non-sedating |
| Desloratadine | Active metabolite of loratadine; non-sedating |
| Fexofenadine | Active metabolite of terfenadine; non-sedating |
| Cetirizine | Carboxylated hydroxyzine; mildly sedating |
| Levocetirizine | R-enantiomer of cetirizine; mildly sedating |
| Azelastine | Also topical (nasal/ophthalmic) |
H2 Antihistaminics
- Cimetidine, Ranitidine, Famotidine, Nizatidine (see Chapter 62 - peptic ulcer)
H3 Antihistaminics
- Pitolisant (used in narcolepsy)
2. MECHANISM OF ACTION (MOA)
H1 antihistaminics are competitive (surmountable), reversible antagonists at H1 receptors. They do not block histamine synthesis or release - they block the receptor-mediated response in target tissues.
- They are more effective in preventing than reversing symptoms once established.
- First-generation agents also bind muscarinic-cholinergic, alpha-adrenergic, and serotonin receptors - hence multiple additional effects.
- Second-generation agents are made polar (e.g., by adding carboxyl groups - cetirizine is the carboxylated derivative of hydroxyzine), which prevents BBB penetration and limits CNS effects.
- Some agents (azelastine, ketotifen) also have mast cell-stabilizing effects in addition to H1 blockade.
Source: Lippincott Illustrated Reviews: Pharmacology
3. COMPARISON: CONVENTIONAL vs. SECOND GENERATION ANTIHISTAMINICS
| Feature | 1st Gen (Conventional) | 2nd Gen (Non-Sedating) |
|---|---|---|
| CNS penetration | High (lipophilic) | Low (polar/hydrophilic, do not cross BBB) |
| Sedation | Marked | Minimal to none |
| Duration of action | 4-6 hours | 12-24 hours (once daily dosing) |
| Receptor selectivity | Non-selective (also M, alpha, 5-HT) | Selective for peripheral H1 |
| Anticholinergic effects | Yes (dry mouth, urinary retention, blurred vision) | Minimal |
| Motion sickness | Effective (diphenhydramine, promethazine, meclizine) | Not effective |
| Insomnia | Used (diphenhydramine, doxylamine) | No value |
| Cardiotoxicity | Rare | Terfenadine/astemizole (withdrawn) caused QT prolongation; newer ones (fexofenadine, loratadine) safe |
| Drug interactions | Potentiate CNS depressants, alcohol; MAOIs | Fewer interactions |
| Paradoxical excitation | Yes (children) | No |
| Examples | CPM, promethazine, diphenhydramine | Loratadine, fexofenadine, cetirizine |
| Appetite stimulation | Cyproheptadine (also 5-HT antagonist) | Not used for this |
| Cost | Inexpensive | More expensive |
4. NON-SEDATIVE (SECOND GENERATION) ANTIHISTAMINICS
Enumeration
- Fexofenadine - truly non-sedating; active metabolite of terfenadine; excreted unchanged in feces
- Loratadine - truly non-sedating; metabolized by hepatic CYP system
- Desloratadine - active metabolite of loratadine; truly non-sedating
- Cetirizine - partially sedating; carboxylated hydroxyzine; excreted unchanged in urine
- Levocetirizine - active R-enantiomer of cetirizine; partially sedating
- Azelastine - also topical (nasal spray, ophthalmic); mast cell stabilizer
- Olopatadine - topical ophthalmic; mast cell stabilizer
- Acrivastine - short-acting
Advantages over 1st Generation
- No sedation (or minimal) - do not cross the BBB due to polar/carboxylated structure
- Longer duration of action (12-24 hours) - once daily dosing improves compliance
- More selective for peripheral H1 receptors - fewer side effects
- No anticholinergic effects - no dry mouth, no urinary retention, no blurred vision
- No paradoxical excitation in children
- Suitable for daytime use - pilots, drivers, students, skilled workers
- No tolerance development to antiallergic effect (tachyphylaxis does not develop as readily)
Two Key Indications
- Allergic rhinitis - drug of choice; controls sneezing, rhinorrhoea, and itching (though not nasal congestion)
- Chronic urticaria - preferred over first generation for long-term management
Precautions
- Cetirizine/levocetirizine: Dose reduction required in renal impairment (excreted unchanged in urine); may still cause mild sedation
- Loratadine/desloratadine: Dose reduction in hepatic impairment (CYP metabolism)
- Fexofenadine: Avoid taking with grapefruit juice or antacids (reduced absorption)
- Driving/operating machinery: Even "non-sedating" agents can cause mild drowsiness in some individuals - patients should be warned
- Cardiac precaution: Older 2nd-gen agents terfenadine and astemizole (now withdrawn) caused fatal QT prolongation/torsades de pointes with CYP3A4 inhibitors (ketoconazole, erythromycin) - current agents (fexofenadine, loratadine) are safe
5. H1 ANTIHISTAMINICS - USES (HIGH-YIELD)
- Allergic conditions - Allergic rhinitis (drug of choice), urticaria, angioedema, allergic conjunctivitis, drug rashes, atopic dermatitis
- Anaphylaxis - Adjunct only (NOT drug of choice - epinephrine is DOC; antihistamines cannot reverse massive histamine release quickly)
- Motion sickness and vertigo - Diphenhydramine, dimenhydrinate, meclizine, promethazine (taken BEFORE travel; ineffective once symptoms start); meclizine also useful for vestibular vertigo
- Nausea and vomiting - Promethazine, diphenhydramine (block central H1 and M1 receptors in vestibular and chemoreceptor pathways)
- Pruritus - Topical/systemic (chlorpheniramine, hydroxyzine)
- Pre-medication/sedation - Promethazine, hydroxyzine
- Insomnia - Diphenhydramine, doxylamine (OTC sleep aids)
- Appetite stimulation - Cyproheptadine (5-HT antagonist action; used in children with poor appetite)
- Cough - Promethazine (combination cough syrups)
- Common cold - Reduce rhinorrhoea, sneezing, itching; no evidence for reducing cold duration
- Blood transfusion reactions - Premedication with chlorpheniramine
- Serotonin syndrome - Cyproheptadine (5-HT antagonist)
Note: H1 antihistaminics are NOT indicated in bronchial asthma - histamine is only one of several mediators causing bronchoconstriction; leukotrienes, prostaglandins also contribute. Epinephrine is DOC in systemic anaphylaxis.
6. ADVERSE EFFECTS
CNS Effects (mainly 1st generation)
- Sedation - most common; chlorpheniramine, diphenhydramine, promethazine, hydroxyzine
- Fatigue, dizziness, lack of coordination, tremors
- Paradoxical CNS stimulation in children - hyperactivity, insomnia, convulsions (diphenhydramine)
- Elderly more sensitive to CNS effects
Anticholinergic Effects (1st generation)
- Dry mouth, dry nasal passages
- Blurred vision (cycloplegia)
- Urinary retention (especially in elderly males with BPH)
- Constipation
- Tachycardia
Cardiovascular
- Terfenadine, astemizole (withdrawn): QT prolongation, torsades de pointes
- Current agents: generally safe
GI Effects
- Nausea, vomiting, epigastric distress, anorexia (or increased appetite - cyproheptadine)
Topical
- Contact dermatitis with topical diphenhydramine
Overdose (especially children)
- Hallucinations, excitement, ataxia, convulsions, deep coma, cardiorespiratory collapse
Drug Interactions
- CNS depressants + alcohol: potentiation of sedation
- MAOIs: exacerbate sedative and anticholinergic effects - AVOID combination
- CYP inhibitors (ketoconazole, erythromycin) + terfenadine/astemizole: QT prolongation (reason for withdrawal)
- Cholinesterase inhibitors (donepezil): anticholinergic H1 blockers may reduce efficacy in Alzheimer's treatment
7. PRECAUTIONS
| Condition | Reason |
|---|---|
| Prostatic hypertrophy | Anticholinergic effects worsen urinary retention |
| Narrow-angle glaucoma | Mydriasis worsens intraocular pressure |
| Epilepsy | Lowers seizure threshold (especially in overdose) |
| Driving/operating machinery | Sedation risk with 1st gen |
| Elderly | More sensitive to CNS and anticholinergic effects |
| Pregnancy | Doxylamine + pyridoxine (Diclegis) - safe for morning sickness; general caution with others |
| Renal failure | Reduce dose of cetirizine/levocetirizine |
| Hepatic failure | Reduce dose of loratadine/desloratadine |
| Concurrent CNS depressants | Additive sedation |
| MAO inhibitors | Contraindicated with antihistamines |
| Children | Paradoxical excitation; risk of overdose toxicity |
Quick Summary Table for Exam
| Drug | Generation | Sedation | Special Feature |
|---|---|---|---|
| Chlorpheniramine | 1st | ++ | Most used; least sedating among 1st gen |
| Promethazine | 1st | +++ | Antiemetic, preanesthetic |
| Diphenhydramine | 1st | +++ | Motion sickness, insomnia |
| Cyproheptadine | 1st | + | 5-HT antagonist; appetite stimulant |
| Hydroxyzine | 1st | ++ | Anxiety, pruritus |
| Meclizine | 1st | + | Vertigo, motion sickness |
| Loratadine | 2nd | 0 | Truly non-sedating |
| Fexofenadine | 2nd | 0 | Truly non-sedating; excreted in feces |
| Desloratadine | 2nd | 0 | Active metabolite of loratadine |
| Cetirizine | 2nd | +/- | Mildly sedating; renally excreted |
| Levocetirizine | 2nd | +/- | R-enantiomer of cetirizine |
| Azelastine | 2nd | +/- | Topical + mast cell stabilizer |
Sources: Lippincott Illustrated Reviews: Pharmacology (Fig. 39.4, 39.5, 39.6, 39.7); Katzung's Basic and Clinical Pharmacology, 16th ed.; Scott-Brown's Otorhinolaryngology (Antihistamines section)
This is a shared conversation. Sign in to Orris to start your own chat.