Here is your complete, detailed 2nd Year MBBS Pharmacology answer on Iron - covering all asked topics with diagrams and flowcharts, based on KD Tripathi principles supplemented from Katzung, Lippincott, and Rosen's Emergency Medicine.
IRON PHARMACOLOGY - Complete 2nd MBBS Answer
IRON ABSORPTION - Mechanism (Essential Background)
Iron exists in two forms:
- Fe²+ (Ferrous) - absorbed form
- Fe³+ (Ferric) - storage/dietary form (must be reduced first)
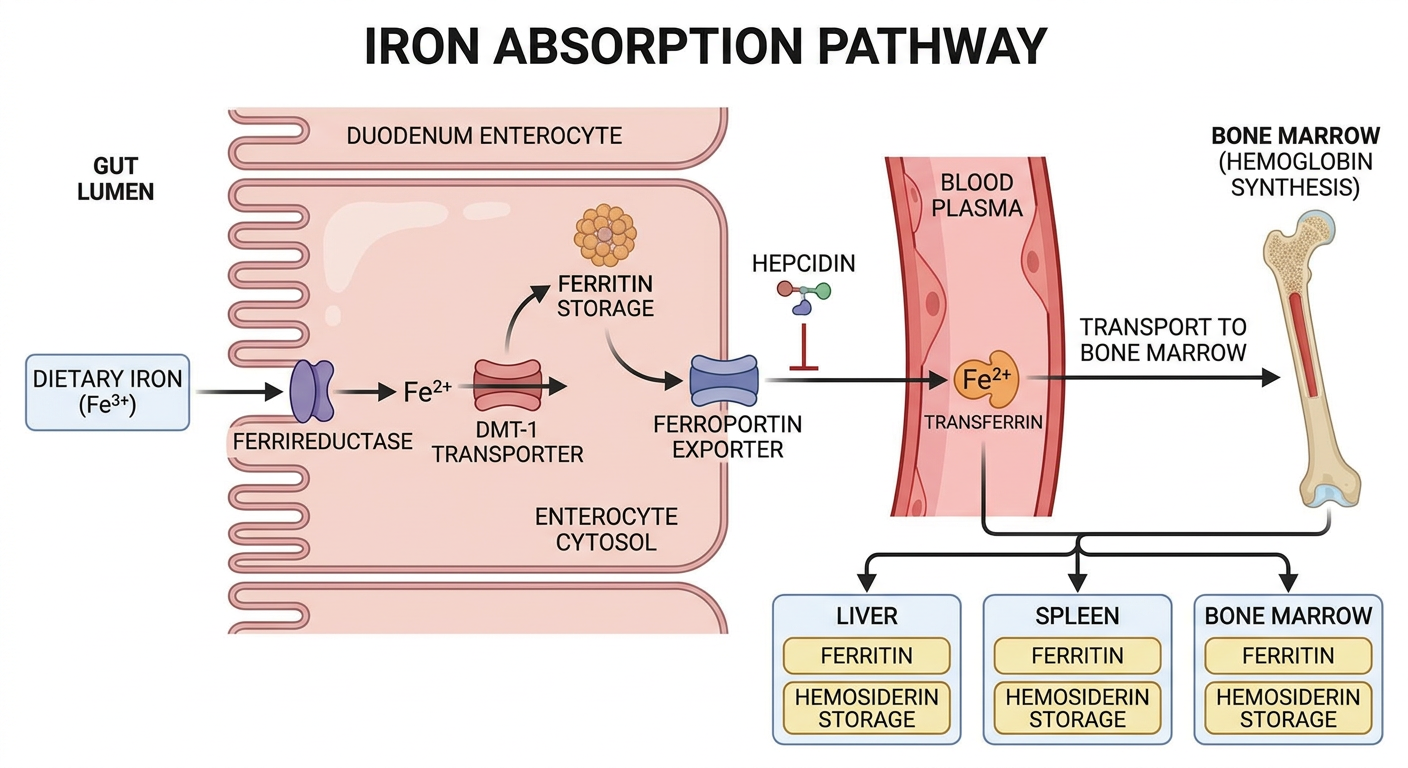
Absorption pathway (Duodenum and upper jejunum):
DIETARY IRON (Fe³⁺ / Haem iron)
↓
Gastric acid + Vitamin C → reduces Fe³⁺ to Fe²⁺
↓
Ferrireductase (Dcytb) on brush border
↓
DMT-1 transporter → enters enterocyte
↓
┌────────────────────────────────┐
│ ENTEROCYTE │
│ • Stored as FERRITIN │
│ • (mucosal block mechanism) │
│ • OR exported via FERROPORTIN│
└────────────────────────────────┘
↓ (ferroportin)
Plasma → binds TRANSFERRIN (Fe³⁺)
↓
BONE MARROW → Hb synthesis
LIVER/SPLEEN/BM → stored as FERRITIN/HEMOSIDERIN
Hepcidin (liver hormone) inhibits ferroportin → blocks iron release from enterocytes and macrophages. In iron deficiency, hepcidin falls → more iron absorbed.
Normal daily requirement:
- Men: 1 mg/day
- Premenopausal women: 2 mg/day
- Pregnant women: 3-4 mg/day
SECTION 1: ORAL IRON PREPARATIONS
Enumerate - Oral Iron Preparations
| Preparation | Tablet Size | Elemental Iron | Dose (Adult) |
|---|
| Ferrous Sulfate (most used) | 325 mg | 65 mg (20%) | 2-4 tabs/day |
| Ferrous Gluconate | 325 mg | 36 mg (11%) | 3-4 tabs/day |
| Ferrous Fumarate | 325 mg | 106 mg (33%) | 2-3 tabs/day |
| Ferrous Succinate | - | ~35% | 2-3 tabs/day |
| Ferric Ammonium Citrate | - | ~18% | Syrup form |
| Carbonyl Iron | - | ~100% | Slower absorption, safer |
| Ferric Hydroxide Polymaltose (IPC) | - | ~20% | Less GI side effects |
Key Point (KD Tripathi): Ferrous salts (Fe²⁺) are better absorbed than ferric salts (Fe³⁺). Ferrous sulfate is the cheapest and most widely used.
Elemental iron content (mnemonic - "Fumarate is the FAT one"):
- Fumarate = 33% (highest)
- Sulfate = 20%
- Gluconate = 11% (lowest)
Indications for Oral Iron
- Iron deficiency anemia (IDA) - most common indication
- Prophylaxis during pregnancy (National Iron + Folic Acid supplementation program)
- Premature infants and rapid growth periods in children
- Menorrhagia / chronic blood loss - menstruating women
- Post-gastrectomy (if absorption is adequate)
- Nutritional deficiency states
Mechanism of Action
- Oral iron provides elemental iron for incorporation into hemoglobin in erythroid precursors in bone marrow
- ~50-100 mg of iron can be incorporated into Hb daily
- ~25% of ferrous iron from oral preparation is absorbed
- So 200-400 mg elemental iron/day needed for rapid correction
Uses / Dose
- Therapeutic dose: 200 mg elemental iron/day in 3 divided doses (equivalent to ~300 mg ferrous sulfate TDS)
- Prophylactic dose: 60 mg elemental iron + 500 mcg folic acid daily (in pregnancy)
- Continue treatment 3-6 months after Hb normalizes (to replenish stores)
- Expected Hb rise: ~1 g/dL/week after adequate treatment
Adverse Effects of Oral Iron
GI Side Effects (most common, dose-related):
| Side Effect | Mechanism |
|---|
| Nausea, vomiting | Direct gastric irritation |
| Epigastric discomfort | Local mucosal irritation |
| Constipation | Most common (Fe²⁺ precipitates sulfides → slows motility) |
| Diarrhea | Osmotic effect in some patients |
| Abdominal cramps | |
| Black tarry stools | Iron sulfide formation (no clinical significance per se, but may mask GI bleeding) |
How to minimize GI side effects:
- Take with food (reduces absorption ~30-50% but improves tolerance)
- Start with lower dose and titrate up
- Change to a different iron salt
- Use liquid formulation (children)
- Enteric-coated tablets (reduce GI side effects but also reduce absorption)
Other adverse effects:
- Tooth staining - liquid preparations (use straw)
- Metallic taste
- Darkening of teeth (in liquid forms)
Interactions:
- Tetracyclines, fluoroquinolones, antacids - chelate iron, reduce absorption
- Vitamin C (ascorbic acid) - ENHANCES iron absorption (reduces Fe³⁺ to Fe²⁺)
- Tea, coffee, phytates - reduce iron absorption
- Give iron 1 hour before or 2 hours after these drugs/foods
SECTION 2: PARENTERAL IRON PREPARATIONS
Enumerate - Parenteral Iron Preparations
| Preparation | Route | Key Features |
|---|
| 1. Iron Dextran (INFeD) | IM / IV | Oldest; high risk of anaphylaxis; test dose mandatory |
| 2. Sodium Ferric Gluconate (Ferrlecit) | IV only | Lower anaphylaxis risk; used in dialysis patients |
| 3. Iron Sucrose (Venofer) | IV only | Safest; most widely used; preferred in CKD |
| 4. Ferric Carboxymaltose (Ferinject) | IV only | High dose possible in single infusion; no test dose |
| 5. Ferumoxytol (Feraheme) | IV only | Superparamagnetic; very rapid infusion; used in CKD |
| 6. Low Molecular Weight Iron Dextran | IV only | Less allergenic than high MW form |
KD Tripathi Note: Iron dextran is a stable complex of ferric oxyhydroxide and dextran polymers containing 50 mg elemental iron/mL.
Indications for Parenteral Iron
- Intolerance to oral iron (persistent GI side effects)
- Malabsorption syndromes (celiac disease, Crohn's of proximal small bowel)
- Post-gastrectomy / short bowel syndrome - inadequate intestinal surface
- Inflammatory bowel disease (IBD) involving proximal small bowel
- Chronic kidney disease (CKD) on hemodialysis + EPO therapy - PREFERRED route
- Functional iron deficiency in cancer patients on erythropoiesis-stimulating agents
- Non-compliance with oral iron
- Rapid iron repletion required (pre-operative patients)
- Severe IDA where oral route is too slow
Adverse Effects of Parenteral Iron
Iron Dextran - Specific Risks:
| Adverse Effect | Details |
|---|
| Anaphylaxis/Anaphylactoid reaction | Most serious; 1-2% risk; test dose MANDATORY (25 mg IV over 5 min, wait 1 hr) |
| Delayed serum-sickness type reaction | Fever, arthralgia, myalgia, lymphadenopathy (Days 1-2 after injection) |
| Hypotension | Especially with rapid IV infusion |
| Pain at IM site | Brown staining of skin with IM injection (use Z-track technique) |
All Parenteral Iron - General Side Effects:
| Adverse Effect | Details |
|---|
| Pain/phlebitis | At injection site |
| Headache, dizziness | |
| Nausea | |
| Flushing, hypotension | With rapid infusion |
| Iron overload | If given excessively (hemosiderosis) |
| Chest pain, dyspnea | Rare with rapid infusion |
Iron Sucrose / Ferric Carboxymaltose (Safer profile):
- Much lower risk of anaphylaxis compared to iron dextran
- No test dose required for iron sucrose and ferric carboxymaltose
- Ferric carboxymaltose: most common side effect is transient hypophosphatemia
Calculation of parenteral iron dose (Iron Dextran):
Total iron (mg) = Weight (kg) × 2.3 × (Target Hb - Actual Hb) + 500
(g/dL)
OR
= 0.3 × Body weight (lbs) × (100 - [Hb × 100/14.8])
SECTION 3: IRON DEFICIENCY ANEMIA - DRUG TREATMENT
Enumerate: Drug Treatment of IDA
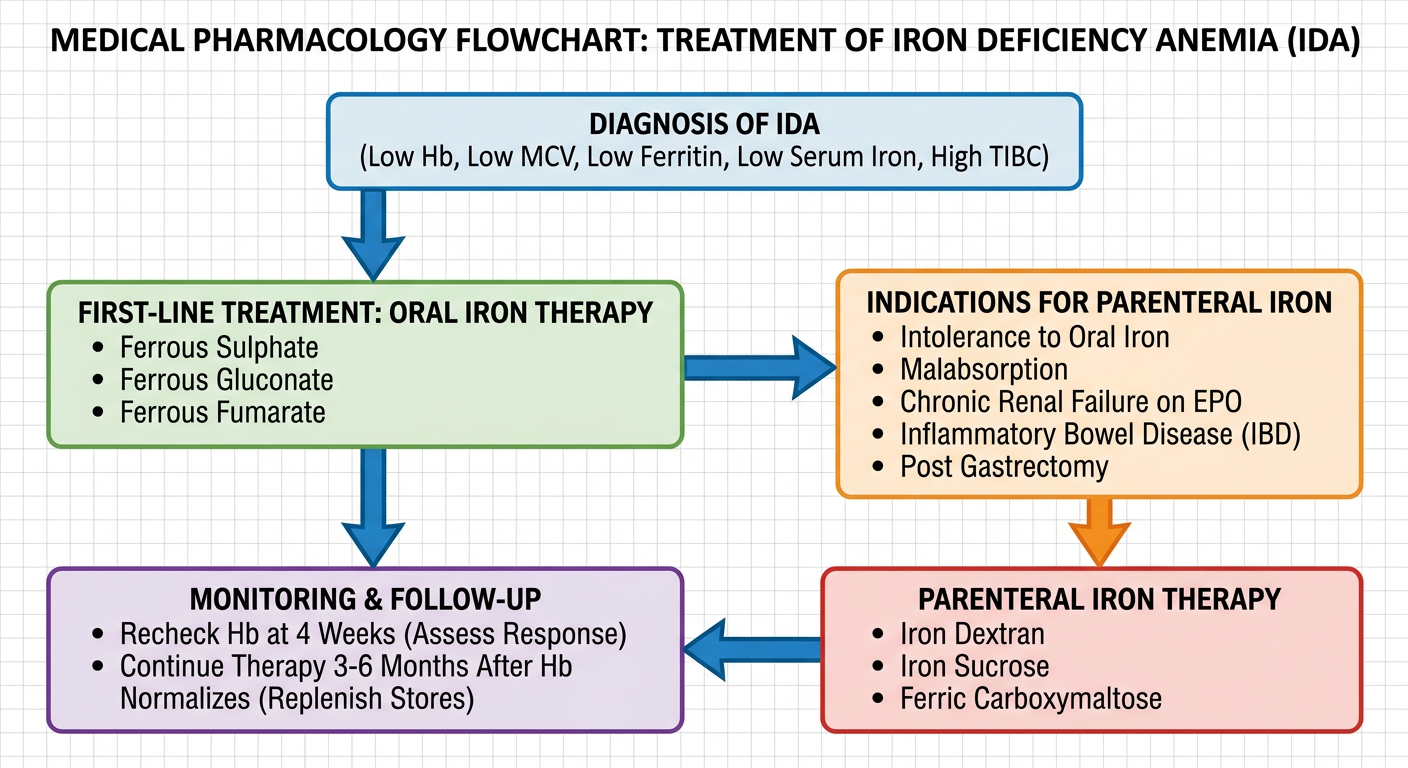
DIAGNOSIS OF IDA
┌──────────────────────────────┐
│ • Low Hb (microcytic, │
│ hypochromic) │
│ • Low MCV (<80 fL) │
│ • Low serum ferritin (<20) │
│ • Low serum iron (<30 mcg/dL)│
│ • High TIBC │
│ • Transferrin sat <10% │
└──────────────┬───────────────┘
↓
TREAT UNDERLYING CAUSE
+
IRON SUPPLEMENTATION
↓
┌────────────────────────────┐
│ FIRST LINE: │
│ ORAL IRON THERAPY │
│ │
│ • Ferrous Sulfate 200mg │
│ elemental iron/day │
│ (in 3 divided doses) │
│ • Continue 3-6 months │
│ after Hb normalizes │
└──────────┬─────────────────┘
│
┌────────────┴──────────────┐
│ Indications for IV/IM │
│ (Parenteral Iron): │
│ • Intolerance to oral │
│ • Malabsorption │
│ • CKD + dialysis + EPO │
│ • IBD (proximal bowel) │
│ • Post-gastrectomy │
│ • Non-compliance │
└────────────┬──────────────┘
↓
PARENTERAL IRON THERAPY
(Iron sucrose preferred)
Drug Treatment - Enumerated List:
A. Oral Iron (First Line):
- Ferrous Sulfate - 325 mg TDS (standard first choice)
- Ferrous Gluconate - 325 mg TDS/QID
- Ferrous Fumarate - 325 mg BD/TDS
- Carbonyl iron (slow release, better GI tolerance)
- Ferric polymaltose complex (IPC) - better GI tolerance, less interaction with food
B. Parenteral Iron (Second Line - specific indications):
- Iron Sucrose (Venofer) - 200 mg IV in 100 mL NS over 15 min
- Ferric Carboxymaltose (Ferinject) - up to 1000 mg single dose
- Sodium Ferric Gluconate - 125 mg IV per session
- Iron Dextran - IM or IV (test dose required)
- Ferumoxytol - 510 mg IV; two doses over 3-8 days
C. Adjuncts:
- Folic acid (if co-deficiency, common in pregnancy)
- Vitamin C (500 mg) with iron - enhances absorption
- Erythropoietin in CKD patients (given WITH parenteral iron)
- Blood transfusion - reserved for Hb <7 g/dL with severe symptoms
Monitoring Response to Iron Therapy:
| Parameter | Expected Change |
|---|
| Reticulocytosis | Peaks at 5-10 days (earliest sign of response) |
| Hb rise | ~1 g/dL/week |
| Hb normalization | 4-8 weeks |
| Iron stores replenished | 3-6 months after Hb normal |
| Serum ferritin | Normalizes last |
Exam Point: If no response to oral iron after 4 weeks, check: compliance, ongoing blood loss, malabsorption, wrong diagnosis.
SECTION 4: IRON POISONING - ANTIDOTES AND TREATMENT
Iron Poisoning - Overview
- Most common in children who accidentally ingest parents' iron tablets or prenatal vitamins
- Toxic dose: >20 mg/kg elemental iron = toxic; >60 mg/kg = potentially lethal
- Fatal dose in children: as low as 200-250 mg elemental iron/kg
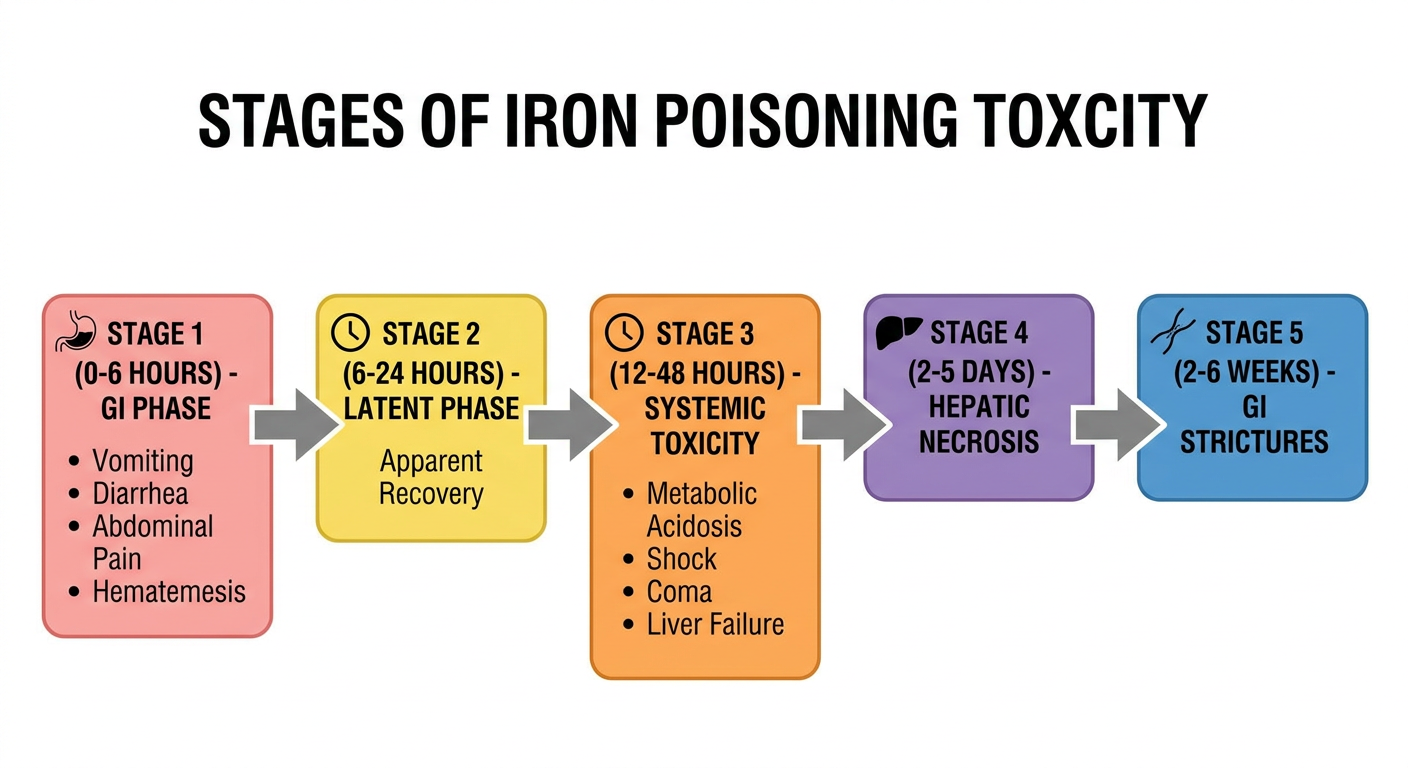
Stages of Iron Toxicity (KD Tripathi / Rosen's Emergency Medicine)
| Stage | Timing | Features | Mechanism |
|---|
| Stage I - GI Phase | 0-6 hours | Vomiting, diarrhea, hematemesis, abdominal pain, GI bleeding | Direct corrosive effect of iron on GI mucosa |
| Stage II - Latent Phase | 6-24 hours | Apparent clinical improvement | Redistribution of iron from GI to systemic circulation |
| Stage III - Systemic Toxicity | 12-48 hours | Metabolic acidosis, shock, hypotension, lethargy, coma, coagulopathy, hepatotoxicity | Free iron catalyzes free radical formation (Fenton reaction) → mitochondrial damage, impaired oxidative phosphorylation |
| Stage IV - Hepatic Necrosis | 2-5 days | Jaundice, liver failure, coagulopathy | Iron deposits in hepatocytes |
| Stage V - Late Complications | 2-6 weeks | GI strictures, pyloric stenosis, bowel obstruction | Fibrosis from GI mucosal injury |
Mnemonic for stages: "GI Lies Sick Having Stenosis" (GI, Latent, Systemic, Hepatic, Strictures)
Mechanism of Iron Toxicity
Free Iron (Fe²⁺/Fe³⁺) in excess
↓
Fenton Reaction:
Fe²⁺ + H₂O₂ → Fe³⁺ + OH⁻ + OH• (hydroxyl radical)
↓
Lipid peroxidation of cell membranes
↓
Mitochondrial dysfunction
↓
↓ ATP production
↓
Cell death in: Liver, Heart, CNS, GI mucosa
↓
Metabolic acidosis (lactic acidosis) + Multi-organ failure
Iron Poisoning - Antidotes
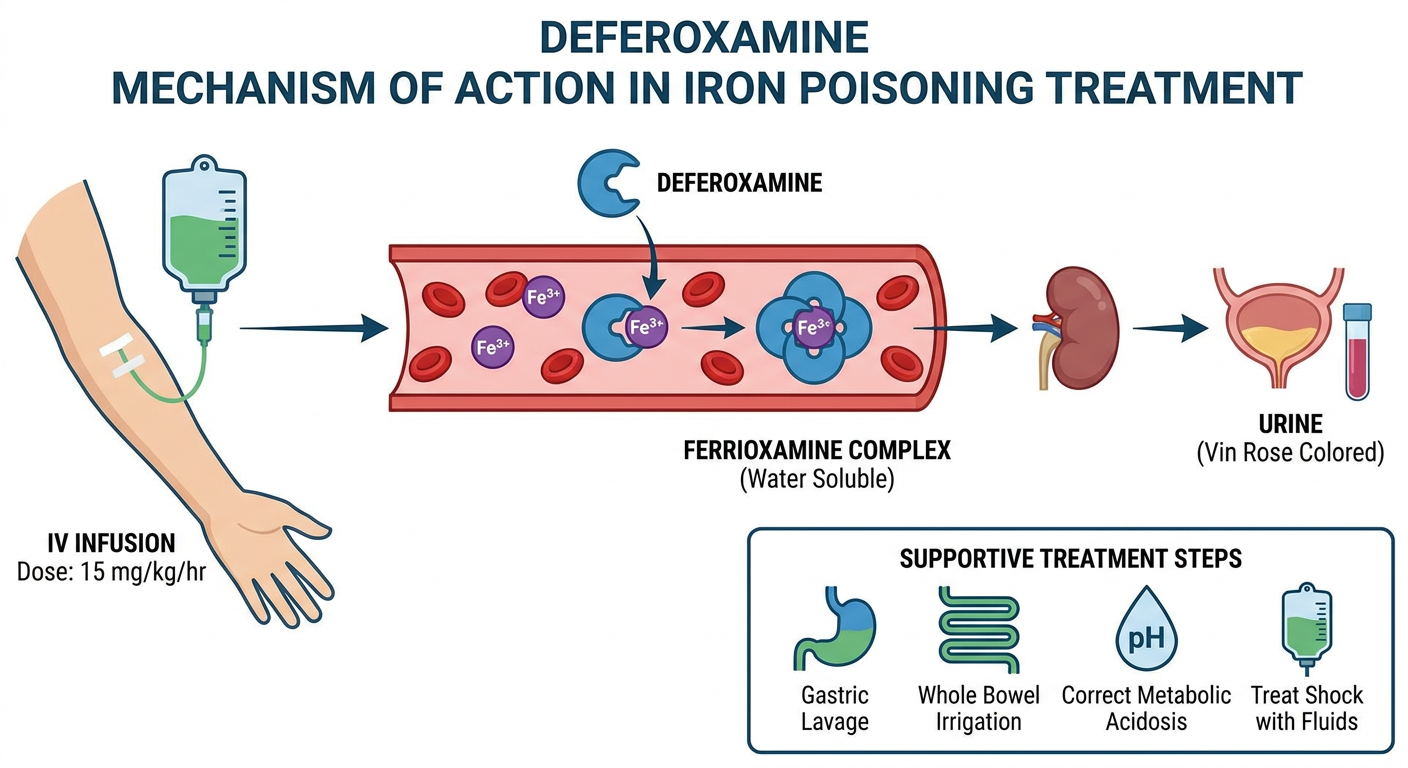
PRIMARY ANTIDOTE: DEFEROXAMINE (Desferrioxamine)
Mechanism:
Deferoxamine + Fe³⁺ → FERRIOXAMINE (water-soluble chelate)
↓
Renally excreted
("Vin rose" / pink-orange colored urine)
- Deferoxamine chelates free iron (Fe³⁺) specifically
- Does NOT chelate iron from hemoglobin, transferrin, or ferritin (selective - only free ionic iron)
- Forms ferrioxamine - excreted in urine (pink/orange = sign of effective chelation)
Dose and Route:
| Route | Dose | Indication |
|---|
| IV (preferred) | 15 mg/kg/hr as continuous infusion (max 35 mg/kg/hr in severe cases) | Severe poisoning |
| IM | 90 mg/kg (max 1 g per dose) every 8 hours | Moderate poisoning |
Indications for Deferoxamine:
- Serum iron >500 mcg/dL
- Serum iron >300 mcg/dL with symptoms
- Metabolic acidosis
- Lethargy, hypotension, signs of shock
- Severe GI symptoms (regardless of measured level)
Duration: Continue until urine color returns to normal (ferrioxamine no longer being excreted) AND patient clinically improves - usually 24 hours; NOT >24 hours unless severe toxicity.
Adverse Effects of Deferoxamine:
- Hypotension (rapid infusion)
- ARDS (with prolonged infusion >24 hours)
- Yersinia sepsis (deferoxamine is a siderophore for Yersinia)
- Tachycardia, urticaria, flushing
- Cataracts with prolonged use (chronic use in thalassemia)
Full Treatment of Iron Poisoning - Enumerate
IRON POISONING MANAGEMENT
│
├─── 1. STABILIZE (ABC)
│ Airway, Breathing, Circulation
│ IV access, O₂, fluids for shock
│
├─── 2. DECONTAMINATION
│ • Gastric lavage (if within 1-2 hr of ingestion)
│ • Activated charcoal - NOT effective for iron
│ (iron does not adsorb to AC)
│ • Whole Bowel Irrigation (WBI) with
│ polyethylene glycol (PEG) solution
│ - if radiopaque tablets visible on X-ray
│ - Rate: 250-500 mL/hr (child) or
│ 1.5-2 L/hr (adult) until effluent clear
│
├─── 3. ANTIDOTE - DEFEROXAMINE
│ • IV: 15 mg/kg/hr continuous infusion
│ • Indication: serum Fe >500 mcg/dL
│ OR severe symptoms
│ • Monitor: vin rose urine
│ • Duration: max 24 hours continuous
│
├─── 4. SUPPORTIVE CARE
│ • Correct metabolic acidosis (sodium bicarbonate)
│ • Fluid resuscitation for hemorrhagic shock
│ • Vasopressors if refractory hypotension
│ • Correct coagulopathy
│ • Monitor liver function tests
│
├─── 5. DIALYSIS / EXCHANGE TRANSFUSION
│ • Hemodialysis - NOT effective
│ (iron has large Vd)
│ • Exchange transfusion - only if not
│ responding to chelation (rare)
│
└─── 6. MONITORING
• Serum iron (3-5 hr post ingestion,
repeat at 6-8 hr)
• LFTs, PT/INR, electrolytes, ABG
• Abdominal X-ray (radiopaque tablets)
Summary Table: Iron Poisoning Treatment
| Step | Treatment | Notes |
|---|
| Decontamination | Whole bowel irrigation | Activated charcoal NOT used |
| Specific antidote | Deferoxamine (IV) | 15 mg/kg/hr; vin rose urine = working |
| Metabolic acidosis | NaHCO₃ | |
| Shock | IV fluids, vasopressors | |
| Hepatic failure | Supportive | LFT monitoring |
| Enhanced elimination | NOT dialysis | Large volume of distribution |
| Late strictures | Surgical | Pyloric/bowel strictures (Stage V) |
QUICK REVISION TABLES
Oral vs Parenteral Iron - Comparison
| Feature | Oral Iron | Parenteral Iron |
|---|
| First choice | Yes | No (reserved) |
| Absorption | ~25% | 100% |
| Cost | Cheap | Expensive |
| GI side effects | Yes (common) | No |
| Anaphylaxis risk | No | Yes (iron dextran) |
| Convenience | Daily tablets | Hospital/clinic visit |
| Test dose needed | No | Yes (iron dextran) |
| Preferred in CKD+EPO | No | Yes |
| Onset of Hb rise | 2-4 weeks | Faster |
| Iron overload risk | Low (mucosal block) | Higher |
Mnemonic - Indications for Parenteral Iron: "MAGIC"
- M - Malabsorption
- A - Advanced CKD / hemodialysis
- G - GI intolerance to oral iron
- I - IBD (proximal bowel)
- C - Compliance failure / post-gastrectomy
Mnemonic for Iron Deficiency Lab Findings: "Low SFTM, High T"
- Low Serum iron
- Low Ferritin
- Low Transferrin saturation (<10%)
- Low MCV, MCH, MCHC
- High TIBC (Total Iron Binding Capacity)
Key Drug Interactions
| Drug/Food | Effect on Iron |
|---|
| Vitamin C | ↑ absorption (reduces Fe³⁺ → Fe²⁺) |
| Tetracyclines | ↓ absorption (chelation) |
| Fluoroquinolones | ↓ absorption |
| Antacids (Mg, Al, Ca) | ↓ absorption |
| Proton pump inhibitors | ↓ absorption (need acid for Fe³⁺ → Fe²⁺) |
| Tea, coffee, phytates | ↓ absorption |
| Milk/dairy | ↓ absorption |
SOURCES
- Katzung's Basic & Clinical Pharmacology, 16e - Chapter 33 (Agents Used in Anemias)
- Lippincott Illustrated Reviews: Pharmacology - Chapter 44 (Iron) & Chapter 46 (Toxicology)
- Rosen's Emergency Medicine - Chapter 146 (Iron Toxicity)
- KD Tripathi Essentials of Medical Pharmacology - Chapter on Haematinics
HIGH-YIELD EXAM POINTS (2nd MBBS)
- Iron sucrose is the safest parenteral iron (preferred in pregnancy and CKD)
- Activated charcoal does NOT adsorb iron - a common MCQ trap
- Vin rose (pink-orange) urine = sign that deferoxamine is working
- Deferoxamine chelates ONLY free iron, not iron in Hb/transferrin/ferritin
- Deferoxamine >24 hours continuous infusion → risk of ARDS and Yersinia sepsis
- Ferrous fumarate has highest elemental iron content (33%)
- Black stools with oral iron = normal, clinically insignificant (but may mask GI bleeding)
- Reticulocytosis peaks at 5-10 days = earliest sign of response to iron therapy
- Stage II (latent phase) of iron poisoning = dangerous - patient seems to recover but systemic toxicity is developing
- Iron dextran requires test dose - other parenteral irons (sucrose, carboxymaltose) do not