Paralytic strabismus
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Now I have rich, detailed textbook content. Let me compile the comprehensive answer.
Paralytic Strabismus
Paralytic strabismus is a misalignment of the visual axes caused by weakness or paralysis of one or more extraocular muscles (EOMs), most commonly due to a cranial nerve (CN III, IV, or VI) lesion. It is primarily a neurologic problem with localizing value.
Definition and Key Concepts
Strabismus = misalignment of the visual axes.
- Paralytic (incomitant): The angle of deviation varies with gaze direction - it is greatest in the direction of action of the weak muscle.
- Nonparalytic (comitant): The misalignment is the same in all directions of gaze; usually has no discrete neurologic cause.
Tropia vs. Phoria:
- A phoria is a latent misalignment overcome by fusion.
- A tropia is a manifest misalignment that cannot be overcome by fusion.
- Prefixes: eso- (inward), exo- (outward), hyper- (upward), hypo- (downward).
"Paralytic strabismus creates an incomitant misalignment, which is of greatest magnitude with gaze in the direction of action of the weak muscle(s) and less magnitude with gaze in the opposite direction."
- Adams and Victor's Principles of Neurology, 12th Ed.
Extraocular Muscles and Their Innervation
| Muscle | Primary Action | Secondary Action | Nerve |
|---|---|---|---|
| Medial rectus | Adduction | - | CN III |
| Lateral rectus | Abduction | - | CN VI |
| Superior rectus | Elevation | Intorsion | CN III |
| Inferior rectus | Depression | Extorsion | CN III |
| Superior oblique | Intorsion | Depression | CN IV |
| Inferior oblique | Extorsion | Elevation | CN III |
Clinical Features of Individual Nerve Palsies
Third Nerve (Oculomotor) Palsy
- Complete palsy produces:
- Ptosis (levator palpebrae weakness)
- Eye positioned "down and out" (unopposed CN IV + VI action)
- Diplopia - false image projected upward and medially
- Dilated, non-reactive pupil (cycloplegia + iridoplegia) due to parasympathetic fiber involvement
- Key distinction - pupil-sparing vs. pupil-involving:
- Pupil spared → microvasculopathic (e.g., diabetic) - pupilloconstrictor fibers lie superficially and are preserved by ischemia affecting central nerve fascicles
- Pupil involved → compressive lesion (e.g., posterior communicating artery aneurysm) - compresses the superficial parasympathetic fibers early
Fourth Nerve (Trochlear) Palsy
- Most common cause of isolated symptomatic vertical diplopia
- Superior oblique weakness → poor downward movement in adduction
- Patient complains of difficulty reading or going downstairs
- Bielschowsky sign: compensatory head tilt to the opposite shoulder to reduce diplopia; diplopia is worsened by ipsilateral head tilt
- Bilateral trochlear palsy (e.g., after head trauma) → alternating hyperdeviation depending on gaze direction
Sixth Nerve (Abducens) Palsy
- Paralysis of lateral rectus → medial deviation of the affected eye (esotropia)
- Horizontal diplopia maximal on gaze toward the side of the palsy and in the distance
- With incomplete palsy: turning the head toward the paretic side can overcome the diplopia
Diplopia Fields Diagram (Maddox Rod Test)
The image below shows diplopia fields for each right-sided muscle paralysis. The red line (Maddox rod in front of right eye) is displaced in the direction of the paretic muscle's action; image separation is maximal in that direction of gaze.
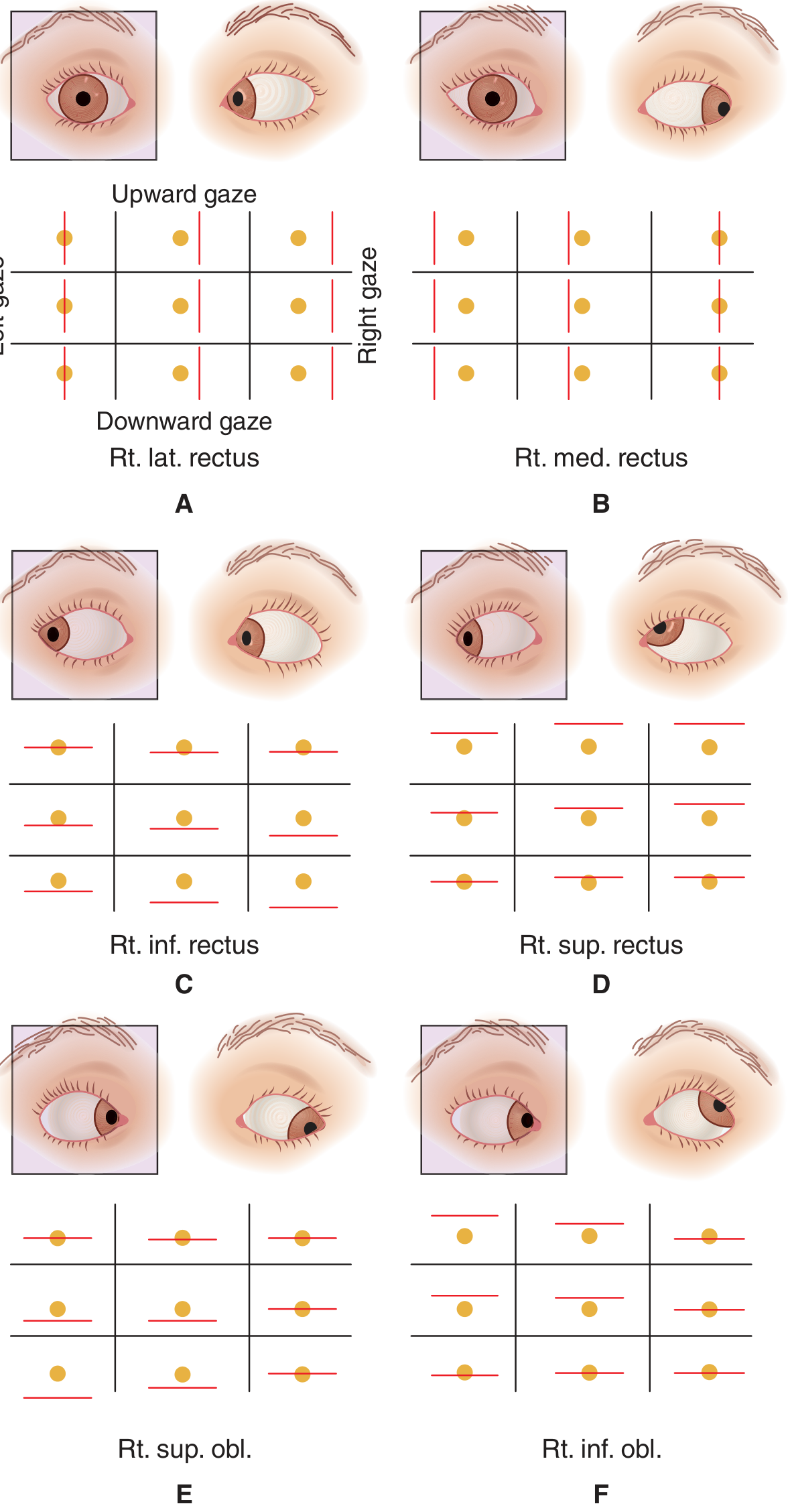
Analysis of Diplopia - Two Rules
-
The direction of maximal image separation = the action of the paretic muscle.
- Maximal horizontal separation on right gaze → right lateral rectus OR left medial rectus weakness.
- Mainly vertical separation → paresis in a vertically acting muscle.
-
The image projected farther from center belongs to the eye with the paretic muscle.
- The false image from the non-fixing paretic eye is displaced in the direction of the weak muscle's action.
- A red glass is placed over one eye (usually the right) and the patient identifies which image (red vs. white) is peripheral in each gaze position.
Alternate cover test: Rapidly alternate an occluder between eyes; observe recovery movement. More practical in children and inattentive patients.
Maddox rod: A transparent red lens with parallel cylindrical bars that converts a point light source into a red line - used to precisely quantify and characterize the deviation.
Causes by Location
CN III Palsy
| Location | Causes |
|---|---|
| Nuclear/fascicular (midbrain) | Infarction, demyelination, tumor, trauma, Wernicke disease |
| Subarachnoid space | Posterior communicating artery aneurysm, meningitis, diabetic infarction, uncal herniation |
| Cavernous sinus / SOF | Diabetic infarction, ICA aneurysm, carotid-cavernous fistula, cavernous thrombosis, pituitary tumor/apoplexy, Tolosa-Hunt syndrome, herpes zoster |
| Orbit | Trauma, fungal infection (mucormycosis), tumor, orbital pseudotumor |
| Uncertain | Migraine, post-infectious cranial neuropathy |
CN IV Palsy
| Location | Causes |
|---|---|
| Nuclear/fascicular (midbrain) | Hemorrhage, infarction, tumor, AVM, demyelination |
| Subarachnoid | Trauma (most common), tumor (pineal, meningioma), meningitis |
| Cavernous sinus / SOF | Tumor, Tolosa-Hunt, ICA aneurysm, herpes zoster, diabetic infarction |
| Raised ICP | Pseudotumor cerebri, meningitis |
CN VI Palsy
| Location | Causes |
|---|---|
| Nuclear/fascicular (pons) | Mobius syndrome, Wernicke syndrome, pontine infarction, demyelination, tumor, lupus |
| Subarachnoid | Aneurysm, trauma, meningitis, skull base tumor |
| Petrous | Mastoiditis/petrous bone infection, inferior petrosal vein thrombosis, trauma (Gradenigo syndrome) |
| Cavernous sinus / SOF | Carotid aneurysm, cavernous sinus thrombosis, pituitary tumor, Tolosa-Hunt, herpes zoster, diabetic infarction |
| Uncertain | Migraine, viral/post-viral |
Note: CN VI palsy is a false localizing sign in raised intracranial pressure, as the nerve is stretched over the petrous ridge by downward displacement of the brainstem.
Important Differentials to Consider
- Myasthenia gravis - fatiguable ophthalmoplegia, variable ptosis, pupil always spared; can mimic any cranial nerve palsy
- Thyroid eye disease - restrictive (not paralytic) due to fibrotic EOM enlargement; diplopia typically worse on upward/outward gaze
- Internuclear ophthalmoplegia (INO) - ipsilateral adduction deficit with contralateral abducting nystagmus; from MLF lesion (MS, brainstem stroke)
- Duane syndrome - congenital; retraction of globe on adduction with limited abduction
- Orbital fracture ("blow-out") - restrictive, not neurogenic
Management Principles
- Treat the underlying cause (e.g., steroids for Tolosa-Hunt, antibiotics for cavernous sinus thrombosis, neurosurgical referral for aneurysm)
- Prism glasses for symptomatic diplopia relief
- Occlusion (patch) to eliminate diplopia acutely
- Botulinum toxin injection to the antagonist muscle during recovery phase (especially CN VI palsy)
- Surgery (recession/resection of EOMs) after 6-12 months if spontaneous recovery has not occurred and deviation is stable
Adams and Victor's Principles of Neurology, 12th Edition, pp. 282-286 | Bradley and Daroff's Neurology in Clinical Practice | Kanski's Clinical Ophthalmology, 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.