rheumatic heart diesase in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"rheumatic heart disease"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Rheumatic Heart Disease (RHD) - Comprehensive Overview
1. Definition and Overview
Rheumatic heart disease (RHD) is the chronic, cumulative cardiac valvular damage that results from one or more episodes of acute rheumatic fever (ARF). It is the most common acquired valvular heart disease worldwide and a leading cause of cardiovascular morbidity and premature death in low- and middle-income countries. RHD cannot be separated epidemiologically from ARF - together they form a disease continuum triggered by Group A beta-haemolytic streptococcal (GAS) pharyngitis.
- Park's Textbook of Preventive and Social Medicine, p. 323
2. Epidemiology
-
Worldwide, there are over 15 million cases of RHD, with approximately 282,000 new cases annually; ~220,000 deaths per year (~0.4% of all deaths)
-
ARF primarily affects children 5-15 years of age; RHD peaks in the third and fourth decades of life
-
ARF is equally common in males and females, but RHD is more common in women
-
Severity is greater in females and correlates with number of prior ARF attacks, delay in therapy, and repeated streptococcal exposures
-
Developing countries bear the highest burden; in affluent countries (North America, Western Europe, Japan), incidence has dramatically declined over recent decades, partly due to socioeconomic improvements before modern treatments
-
In South Africa, 82.5% of affected children were previously undiagnosed at presentation - highlighting the silent nature of RHD
-
Goldman-Cecil Medicine, p. 398-399; Park's PSM, p. 343-357; Firestein & Kelley's Rheumatology, p. 9993
3. Pathogenesis and Immunology
RHD is driven by molecular mimicry - a cross-reactive autoimmune response directed against streptococcal antigens that inadvertently attacks host cardiac tissue.
The Molecular Mimicry Mechanism
- Initial trigger: GAS pharyngeal infection generates antibodies and T cells against streptococcal proteins
- Cross-reactivity: Antibodies against GAS N-acetyl-glucosamine (a streptococcal carbohydrate) simultaneously recognize cardiac myosin in the myocardium and troponin/laminin in the valves
- Endothelial activation: These antibodies bind valvular endothelium, upregulating adhesion molecules:
- VCAM-1 (vascular cell adhesion molecule-1) is activated by anti-myosin and anti-N-acetylglucosamine antibodies
- VCAM-1 interacts with VLA-4 (very late activation antigen-4) on CD4+ T lymphocytes, facilitating their extravasation into heart tissue
- Chemokine-mediated infiltration: CCL3/MIP1α is upregulated in myocardium; CCL1/I-309 and CXCL9/Mig are elevated in valvular tissue. Infiltrating T cells migrate along a CXCL9/Mig gradient into valve lesions
- Cytokine storm: Elevated IL-2, TNF, IFN-γ; Th17 cells and IL-17/IL-23 are prominent in valves. Low IL-4-producing cells may account for why regulatory suppression fails in valvular tissue
- Key autoantigen - Cardiac Myosin: 63.2% of intralesional T cell clones recognize light meromyosin (LMM) peptides. 34% show cross-reactivity patterns between myosin, streptococcal M5 peptides, and valve-derived proteins
Valvular Tissue Changes
In valvulitis, there is altered protein expression:
- High expression: Vimentin, lumican, apolipoprotein-A1
- Low expression: Collagen VI, haptoglobin-related protein, prolargin, biglycan, cartilage oligomeric matrix protein
This ultimately causes fibrosis, thickening, fusion, and calcification of valve leaflets and subvalvular apparatus.
- Firestein & Kelley's Rheumatology, pp. 274-316
4. Pathology of the Heart Valves
Valve involvement in RHD (in order of frequency):
| Valve | Involvement | Common Lesion |
|---|---|---|
| Mitral | ~100% | Regurgitation > Stenosis |
| Aortic | 20-30% | Regurgitation > Stenosis |
| Tricuspid | 15-40% (histologic) | Usually secondary to pulmonary hypertension |
| Pulmonic | Rare | Rarely clinically significant |
Mitral Valve Disease
- Acute phase: Valvular regurgitation from inflammatory leaflet damage
- Chronic phase: Progressive scarring leads to mitral stenosis - the most common cause of mitral stenosis worldwide
- Characteristic "fish mouth" funnel valve deformity: commissural fusion hindering leaflet opening, with fusion and shortening of chordae tendineae and sclerosis reducing leaflet pliability
Aortic Valve Disease
- When involved: regurgitation is more common than stenosis
- Sclerosis impairs both valve opening (stenosis) and closing (regurgitation/gap)
Tricuspid Valve
- Secondary tricuspid regurgitation (TR) develops from upstream hemodynamic stress of mitral stenosis, leading to pulmonary hypertension, right ventricular dilatation, and tricuspid annular dilation
Pathological specimen - Rheumatic Mitral Valve:
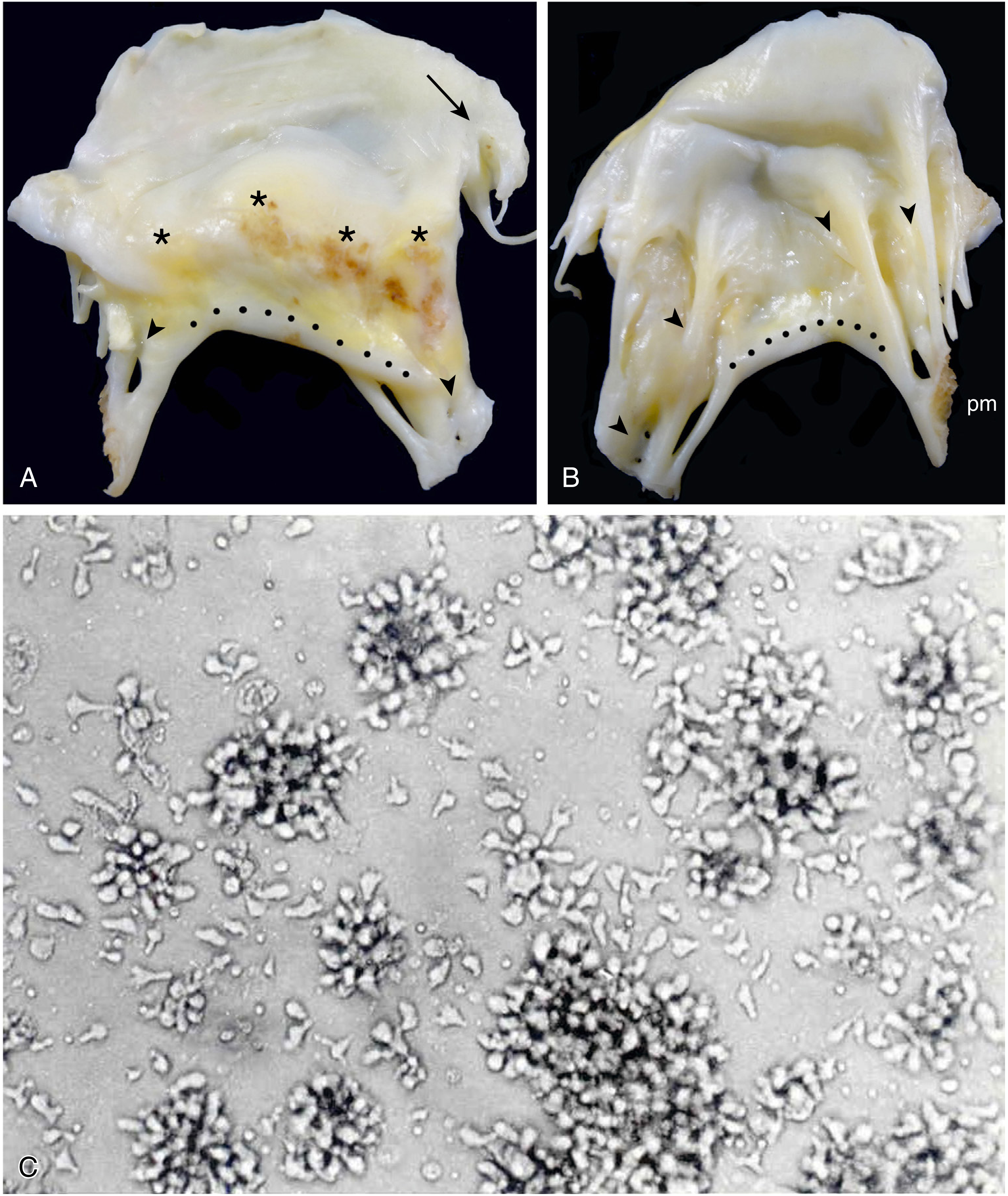 Atrial (A) and ventricular (B) aspects of a surgical specimen showing post-rheumatic mitral insufficiency and stenosis. Note thickened, calcified, distorted leaflets with commissural adherence (arrow), crescentic notching (dotted line), and chord fusion/retraction (arrowheads). (C) CD4+ T cells cultured from valve fragments.
Atrial (A) and ventricular (B) aspects of a surgical specimen showing post-rheumatic mitral insufficiency and stenosis. Note thickened, calcified, distorted leaflets with commissural adherence (arrow), crescentic notching (dotted line), and chord fusion/retraction (arrowheads). (C) CD4+ T cells cultured from valve fragments.
"Fish mouth" mitral valve deformity:
 Classic pathognomonic mixed stenotic/regurgitant "fish mouth" funnel valve lesion with commissural fusion.
Classic pathognomonic mixed stenotic/regurgitant "fish mouth" funnel valve lesion with commissural fusion.
- Sabiston Textbook of Surgery, pp. 1249-1276; Goldman-Cecil Medicine, p. 499
5. Clinical Manifestations of Acute Rheumatic Fever (ARF)
ARF develops approximately 2 weeks after GAS pharyngitis and lasts 2-4 weeks.
| Manifestation | Frequency | Features |
|---|---|---|
| Fever | >90% | Usually >38.5°C |
| Polyarthritis | ~75% | Large-joint, migratory; sterile synovial fluid with lymphocyte predominance; resolves dramatically with NSAIDs |
| Carditis | >50% (clinical); additional ~18% subclinical | Pancarditis - pericarditis, myocarditis, valvulitis |
| Chorea (Sydenham's) | ~30% | Non-rhythmic, purposeless, jerky movements; worse on one side; stops during sleep; associated with emotional lability and personality changes |
| Erythema marginatum | <10% | Pink, non-pruritic, blanching macules/papules spreading in a serpiginous pattern on trunk and proximal limbs |
| Subcutaneous nodules | <10% | 0.5-2 cm, painless, over bony prominences or extensor tendons |
Other findings: Prolonged PR interval on ECG, elevated ESR/CRP, normochromic normocytic anemia, leukocytosis, tachycardia out of proportion to fever.
- Goldman-Cecil Medicine, pp. 407-411
6. Diagnosis - Revised Jones Criteria (2015, AHA)
ARF is a diagnosis of exclusion - no single test confirms it. The 2015 revised Jones criteria (updated for Doppler echocardiography) are used.
Diagnostic thresholds:
- Initial ARF: 2 major OR 1 major + 2 minor criteria
- Recurrent ARF: 2 major OR 1 major + 2 minor OR 3 minor criteria
Major Criteria
| Low-Risk Populations | Moderate/High-Risk Populations | |
|---|---|---|
| Carditis | Clinical and/or subclinical echocardiographic valvulitis | Same |
| Arthritis | Polyarticular only | Monoarticular OR polyarticular |
| Chorea | Yes | Yes |
| Erythema marginatum | Yes | Yes |
| Subcutaneous nodules | Yes | Yes |
Minor Criteria
| Low-Risk | Moderate/High-Risk | |
|---|---|---|
| Arthralgia | Polyarthralgia | Monoarthralgia |
| Fever | ≥38.5°C | ≥38.5°C |
| Inflammatory markers | ESR ≥60 mm AND/OR CRP ≥3.0 mg/dL | ESR ≥30 mm AND/OR CRP ≥3.0 mg/dL |
| ECG | Prolonged PR interval | Prolonged PR interval |
Key update: The 2015 revision introduced subclinical carditis (echocardiographic valvulitis without auscultatory findings) as a major criterion for moderate/high-risk populations.
Low-risk populations: ARF incidence <2 per 100,000 school-aged children/year OR RHD prevalence ≤1 per 1000 population.
Evidence of preceding GAS infection is also required: positive throat culture/rapid antigen test OR elevated/rising streptococcal antibody titres (ASO, anti-DNase B).
- Goldman-Cecil Medicine, pp. 422-483
7. Clinical Presentation of Chronic RHD
RHD is typically oligosymptomatic until heart failure (HF) is established.
Age-related presentation patterns:
- Young patients: Pure mitral regurgitation
- Middle-aged adults: Mitral stenosis
- Older patients: Mixed mitral valve disease
Heart failure features: Third heart sound, tachycardia, dyspnea, pulmonary rales, peripheral edema.
Prognosis by NYHA class:
- Oligosymptomatic at diagnosis: 60% will not progress over 10 years; survival >80%
- NYHA class III-IV without surgery: 0-15% survival over 10 years
- Severe pulmonary hypertension without surgery: survival <3 years
Classic murmurs in RHD:
- Mitral stenosis: Rumbling mid-diastolic murmur at apex; opening snap; loud S1
- Mitral regurgitation: Pansystolic murmur at apex radiating to axilla
- Aortic regurgitation: Early diastolic decrescendo murmur at left sternal border
Complications: Atrial fibrillation, systemic embolism/stroke, infective endocarditis, pulmonary hypertension, heart failure
- Firestein & Kelley's Rheumatology, pp. 9992-10005; Goldman-Cecil Medicine, pp. 499-503
8. Investigations
| Investigation | Findings in RHD/ARF |
|---|---|
| Throat culture | GAS identified (but ~75% negative by time of ARF symptoms) |
| ASO titre | Elevated (>200 Todd units in adults, >320 in children); rises 3-4 weeks post-infection |
| Anti-DNase B | More sensitive than ASO for skin infections |
| ESR / CRP | Elevated; used in Jones criteria |
| CBC | Normochromic normocytic anemia, leukocytosis |
| ECG | Prolonged PR interval (1st degree AV block); atrial fibrillation in chronic disease |
| Chest X-ray | Cardiomegaly, left atrial enlargement, pulmonary congestion |
| Echocardiography | KEY diagnostic tool - identifies subclinical carditis; assesses valve morphology, gradients, regurgitation severity; guides management |
9. Treatment
A. Treatment of Acute Rheumatic Fever
Hospitalization is indicated for all patients with ARF.
1. Eradication of GAS:
- Intramuscular (IM) benzathine penicillin G 1.2 million units (single dose)
- Alternative: Oral penicillin V 10 days OR oral amoxicillin
- Penicillin-allergic patients: Oral macrolide (azithromycin) or cephalosporin
2. Anti-inflammatory therapy (joint symptoms):
- First-line: Aspirin 80-100 mg/kg/day in divided doses (max 4-8 g/day) for 1-2 weeks
- Alternative: Naproxen 10-20 mg/kg/day in divided doses
- Treatment should continue 1-2 weeks after ALL symptoms resolve
3. Carditis management:
- Mild-moderate: NSAIDs/aspirin
- Severe carditis with HF: Corticosteroids (prednisone) may be used, though evidence for preventing chronic RHD is limited
4. Chorea:
- Self-limiting; may require valproic acid or haloperidol for severe cases
B. Secondary Prophylaxis (Most Critical Intervention)
Secondary prophylaxis prevents recurrent ARF and halts further valve damage. Insufficiency from acute rheumatic valve disease resolves in 60-80% of patients who adhere to antibiotic prophylaxis.
| Drug | Dose | Route | Frequency |
|---|---|---|---|
| Benzathine penicillin G (preferred) | 1.2 million units | IM | Every 3-4 weeks |
| Penicillin V | 250 mg | Oral | Twice daily |
| Amoxicillin | 250 mg | Oral | Once daily |
| Sulfadiazine | 0.5 g (<30 kg) / 1 g (>30 kg) | Oral | Once daily |
| Erythromycin (penicillin allergic) | 250 mg | Oral | Twice daily |
Duration of secondary prophylaxis:
| Condition | Duration |
|---|---|
| ARF without carditis | 5 years or until age 21 (whichever is longer) |
| ARF with carditis, no residual valve disease | 10 years or until age 21 |
| ARF with carditis + residual valve disease | Minimum 10 years or until age 40 (often lifelong) |
| High-risk patients (teachers, healthcare workers, crowded conditions) | Lifelong |
A 2024 Cochrane systematic review (PMID 39312290) confirmed that long-term antibiotic prophylaxis prevents recurrence and progression to RHD.
C. Interventional/Surgical Management
Mitral Stenosis:
- Percutaneous mitral balloon valvuloplasty (PMBV/PMC): Preferred for pliable, non-calcified valves with favorable morphology (Wilkins score ≤8); now feasible even with left atrial appendage thrombus (2026 meta-analysis, PMID 41862112)
- Closed mitral commissurotomy: Historic procedure; still performed in resource-limited settings
- Open mitral commissurotomy: Under cardiopulmonary bypass
- Mitral valve replacement (MVR): Mechanical or bioprosthetic valve; for severely distorted, calcified valves not amenable to repair
Mitral Regurgitation:
- Mitral valve repair preferred over replacement when feasible
- Replacement required for severely deformed valves
Aortic Valve Disease:
- Repair less commonly feasible; typically requires aortic valve replacement (AVR)
- TAVR increasingly used in high-risk surgical patients
General surgical indications follow the severe hemodynamic derangement and symptom threshold (NYHA class, LV function, pulmonary pressures).
- Goldman-Cecil Medicine, pp. 486-503; Sabiston Textbook of Surgery, pp. 1249-1276; Goodman & Gilman's Pharmacology, p. 722
10. Prevention
Primary Prevention
- Early identification and complete treatment of GAS pharyngitis with a 10-day course of penicillin (or amoxicillin) - prevents the first episode of ARF
- Improved socioeconomic conditions, reduced overcrowding, better nutrition
Secondary Prevention
- As above - long-term benzathine penicillin G prophylaxis
Echocardiographic Screening
- In endemic regions, echocardiographic screening detects latent/subclinical RHD before clinical presentation
- Guides secondary prophylaxis to reduce progressive disease at a population level
- Follows World Heart Federation (WHF) echocardiographic diagnostic criteria (2012)
11. Prognosis and Natural History
| Phase | Key Points |
|---|---|
| Post-ARF | 35-72% develop clinical carditis; 18% subclinical carditis |
| Resolution | Some have complete resolution within 1 year, especially if prophylaxis maintained |
| Progressive RHD | Severe valvular disease typically manifests in the 3rd-4th decade |
| NYHA I-II at diagnosis | 60% stable at 10 years; >80% survival |
| NYHA III-IV | 0-15% survival at 10 years without surgery |
| Pulmonary hypertension | <3 years survival without intervention |
Variables that worsen prognosis:
- Multiple prior ARF attacks
- Delayed treatment initiation
- Female sex
- Poor adherence to secondary prophylaxis
12. Recent Evidence Updates (2024-2026)
- [PMID 39542478] - A 2024 meta-analysis found that adherence to secondary prophylaxis among RHD/ARF patients remains suboptimal globally, highlighting a major gap in prevention
- [PMID 39312290] - 2024 Cochrane review confirmed long-term antibiotic prophylaxis prevents recurrence and RHD progression; IM benzathine penicillin G is superior to oral regimens
- [PMID 41862112] - 2026 meta-analysis showed PMBV (percutaneous mitral balloon valvuloplasty) is feasible and effective even in patients with severe mitral stenosis and left atrial appendage thrombus, expanding interventional options
Sources:
- Firestein & Kelley's Textbook of Rheumatology
- Goldman-Cecil Medicine International Edition
- Sabiston Textbook of Surgery (The Biological Basis of Modern Surgical Practice)
- Park's Textbook of Preventive and Social Medicine
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- PubMed systematic reviews (2024-2026)
This is a shared conversation. Sign in to Orris to start your own chat.