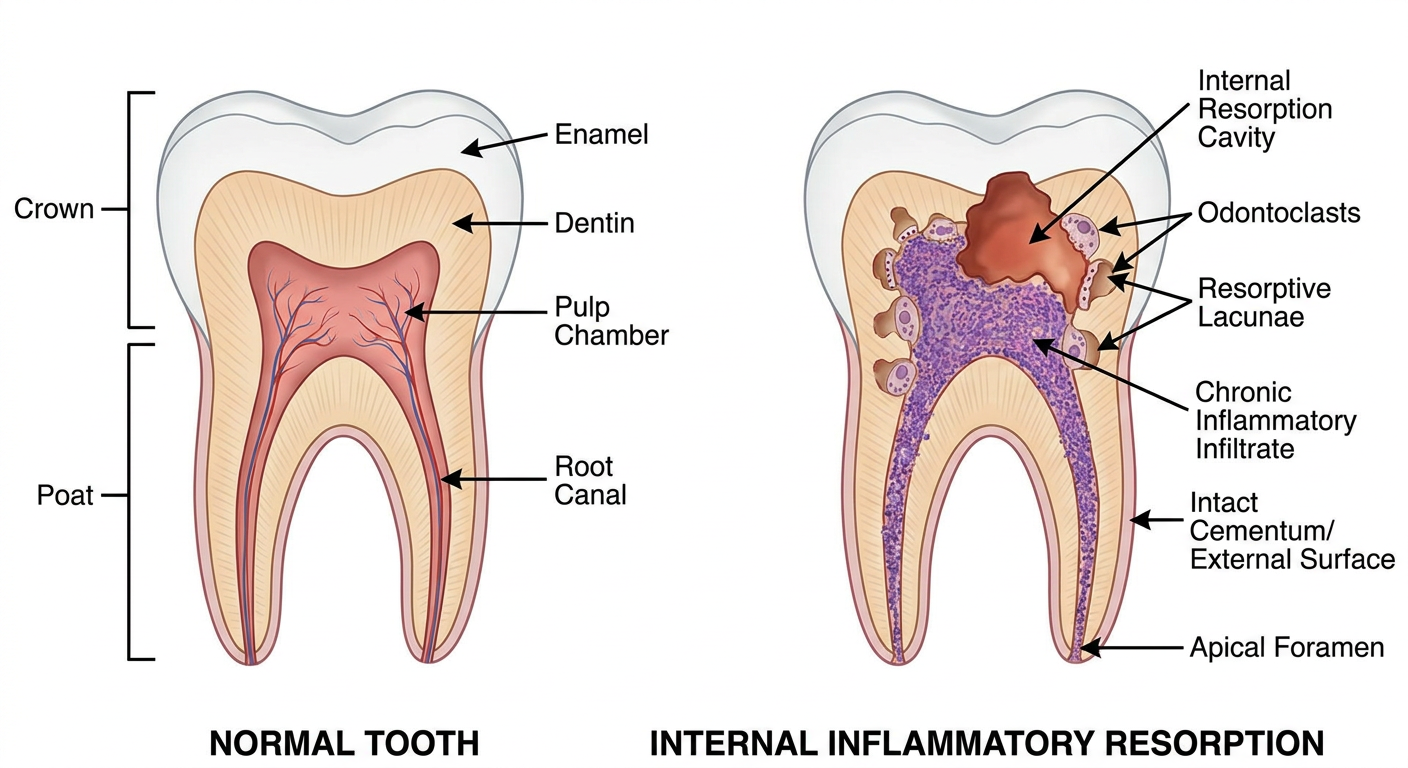
DISCUSSION Internal inflammatory resorption is initiated by clastic activity within chronically inflamed vital pulp tissue.[1] Trauma is considered a major etiologic factor because damage to predentin and the odontoblastic layer may expose mineralized dentin to odontoclasts.[2] In the present case, childhood trauma was considered the probable initiating factor. Diagnosis of internal resorption may be difficult because lesions are often asymptomatic. Conventional radiographs may reveal characteristic enlargement of the pulp space, but their two‑dimensional nature limits accurate assessment of lesion extent and perforation.[11] CBCT enables precise three‑dimensional evaluation and facilitates differentiation from external cervical resorption.[3] In the present case, CBCT confirmed preservation of the external root surface and absence of perforation, enabling conservative nonsurgical management. Histopathologic examination demonstrated chronic inflammatory infiltrate, multinucleated odontoclast‑like cells, and resorptive lacunae adjacent to dentinal fragments, findings consistent with internal inflammatory resorption.[1] Histopathologic correlation is infrequently reported in clinical case reports but provides valuable biological confirmation of the diagnosis and strengthens the correlation between clinical and radiographic findings. The primary objective of treatment is the elimination of inflamed pulp tissue to arrest clastic activity.[1] Chemomechanical debridement and intracanal medication are effective in halting the progression of the lesion. Similar conservative multidisciplinary management approaches for extensive internal inflammatory resorption have also been reported in the literature.[12] In the present case, obturation with bioceramic sealer provided satisfactory adaptation within the irregular canal anatomy.[13] Extensive internal resorption significantly weakens dentinal walls, especially in the cervical region where stress concentration is highest.[4] Conventional management strategies include calcium silicate‑based materials, thermoplasticized obturation techniques, fiber posts, and composite restorations.[5,7,14] Although these approaches provide adequate sealing and clinical success, reinforcement of severely weakened cervical dentin may remain challenging.[14] The present biomimetic approach utilized polyethylene fiber incorporated within fiber‑reinforced composite to provide conservative internal reinforcement without aggressive post preparation. Polyethylene fibers act as a stress‑distributing scaffold capable of limiting crack propagation within weakened dentin.[6] Fiber‑reinforced composites have also demonstrated improved biomechanical behaviour and fracture resistance in structurally compromised teeth.[5] The restorative strategy used in this case was consistent with principles of the Bio block or Bio‑Bulk concept described by Fráter et al., in which short fiber‑reinforced composite was used to reinforce roots affected by internal resorption.[8] However, unlike the Bio block technique where the canal space was extensively reinforced with fiber composite, the present case incorporated polyethylene fiber reinforcement mainly within the cervical region and canal orifice to preserve remaining dentin and enamel. Similar studies have demonstrated favourable stress distribution and reinforcement using fiber‑reinforced restorative materials in weakened teeth.[9,10] Although fiber‑reinforced restorative strategies have been investigated in endodontically treated teeth, reports describing polyethylene fiber reinforcement combined with CBCT‑guided diagnosis and histopathologic correlation in extensive internal inflammatory resorption remain limited. The present case is clinically relevant because treatment was directed not only toward elimination of the resorptive process but also toward biomechanical rehabilitation of the structurally compromised tooth. Unlike conventional restorative approaches focused primarily on obturation or defect repair, the present technique emphasized conservative internal reinforcement and preservation of weakened cervical dentin. The combined use of CBCT‑guided diagnosis, histopathologic confirmation, and biomimetic polyethylene fiber reinforcement therefore highlights the novelty and multidisciplinary relevance of the present management approach. Nevertheless, long‑term clinical studies and larger case series are required to further evaluate the durability, fracture resistance, and long‑term clinical performance of this conservative biomimetic reinforcement approach.
internal inflammatory resorption CBCT diagnosis treatment
fiber reinforced composite endodontically treated teeth fracture resistance
internal inflammatory resorption polyethylene fiber reinforced composite biomimetic treatment case report
Analysis of the Discussion Section
What This Discussion Does Well
Weaknesses and Areas for Improvement
Summary Assessment
| Criterion | Score (out of 5) |
|---|---|
| Logical structure and flow | 5/5 |
| Accuracy of clinical content | 4/5 |
| Use of current literature | 3/5 |
| Strength of novelty argument | 3/5 |
| Acknowledgment of limitations | 4/5 |
| Language precision | 3/5 |
| Overall | 3.7/5 |
Need better discussion and also need images
internal inflammatory resorption pathogenesis odontoclast trauma pulp
fiber reinforced composite fracture resistance endodontically treated teeth cervical
CBCT internal resorption external cervical differentiation diagnosis
internal inflammatory resorption CBCT diagnosis treatment fiber reinforced composite polyethylene biomimetic 2023 2024 2025
internal root resorption nonsurgical endodontic treatment bioceramic sealer obturation
fiber reinforced composite fracture resistance endodontically treated teeth
polyethylene fiber reinforcement biomimetic tooth fracture resistance
https://pocketdentistry.com/the-use-of-cbct-in-the-diagnosis…
PMID: 37574536
PMID: 36862198
PMID: 39346441
A detailed scientific cross-sectional diagram of a tooth showing internal inflammatory resorption. The diagram shows: on the left, a normal tooth with labeled pulp chamber and root canal; on the right, the same tooth with internal inflammatory resorption showing: enlarged irregular pulp space, odontoclasts (multinucleated giant cells) lining resorptive lacunae, chronic inflammatory infiltrate in pulp, intact external root surface, predentin layer loss in resorption zone. Labels include: crown, enamel, dentin, pulp chamber, internal resorption cavity, odontoclasts, resorptive lacunae, intact cementum/external surface, apical foramen. Clean white background, professional medical illustration style, educational dental anatomy diagram.
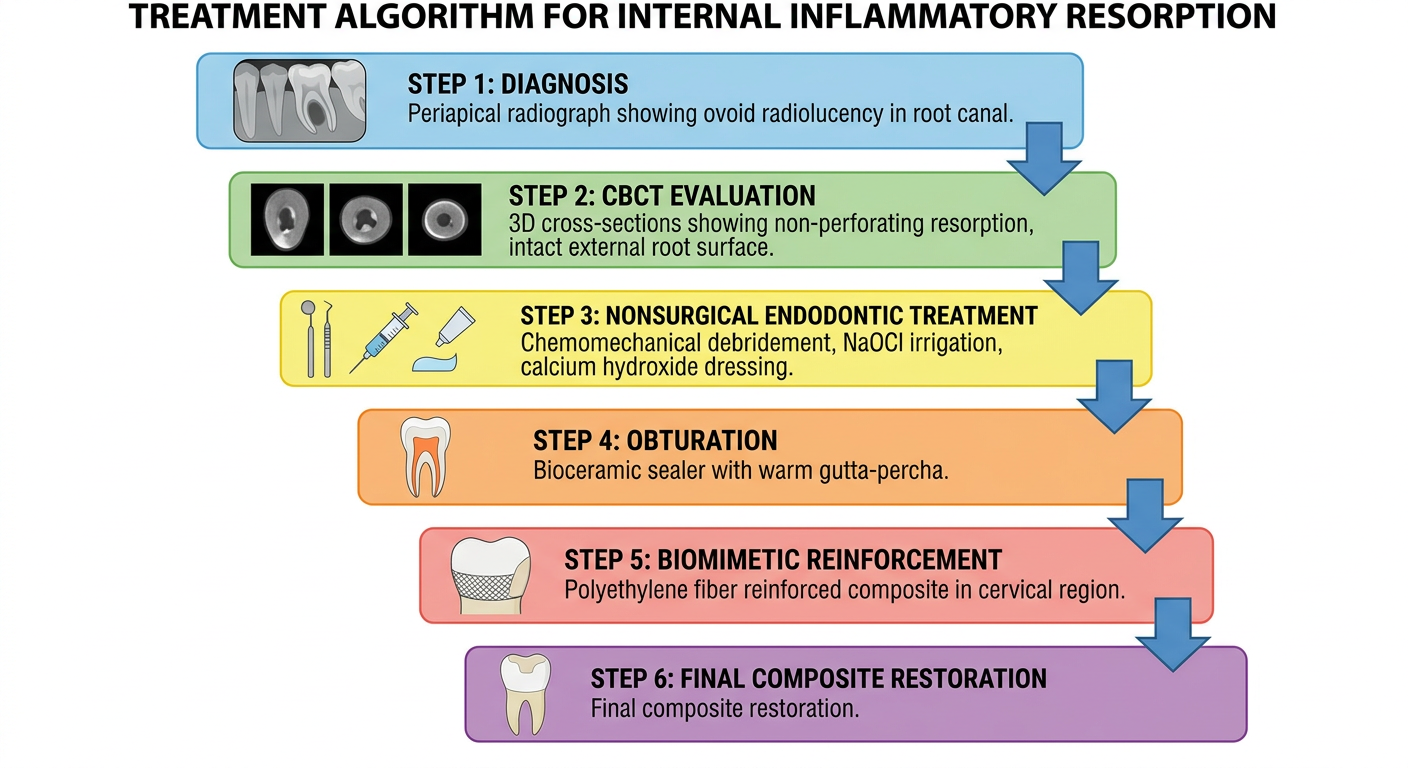
A clear scientific dental diagram showing the step-by-step treatment algorithm for internal inflammatory resorption. Flowchart style with boxes and arrows: Step 1 - Diagnosis (periapical radiograph showing ovoid radiolucency in root canal); Step 2 - CBCT evaluation (3D cross-sections showing non-perforating resorption, intact external root surface); Step 3 - Nonsurgical endodontic treatment (chemomechanical debridement, NaOCl irrigation, calcium hydroxide dressing); Step 4 - Obturation (bioceramic sealer with warm gutta-percha); Step 5 - Biomimetic reinforcement (polyethylene fiber reinforced composite in cervical region); Step 6 - Final composite restoration. Professional clinical flowchart, clean white background, dental educational infographic style with color coding per step.
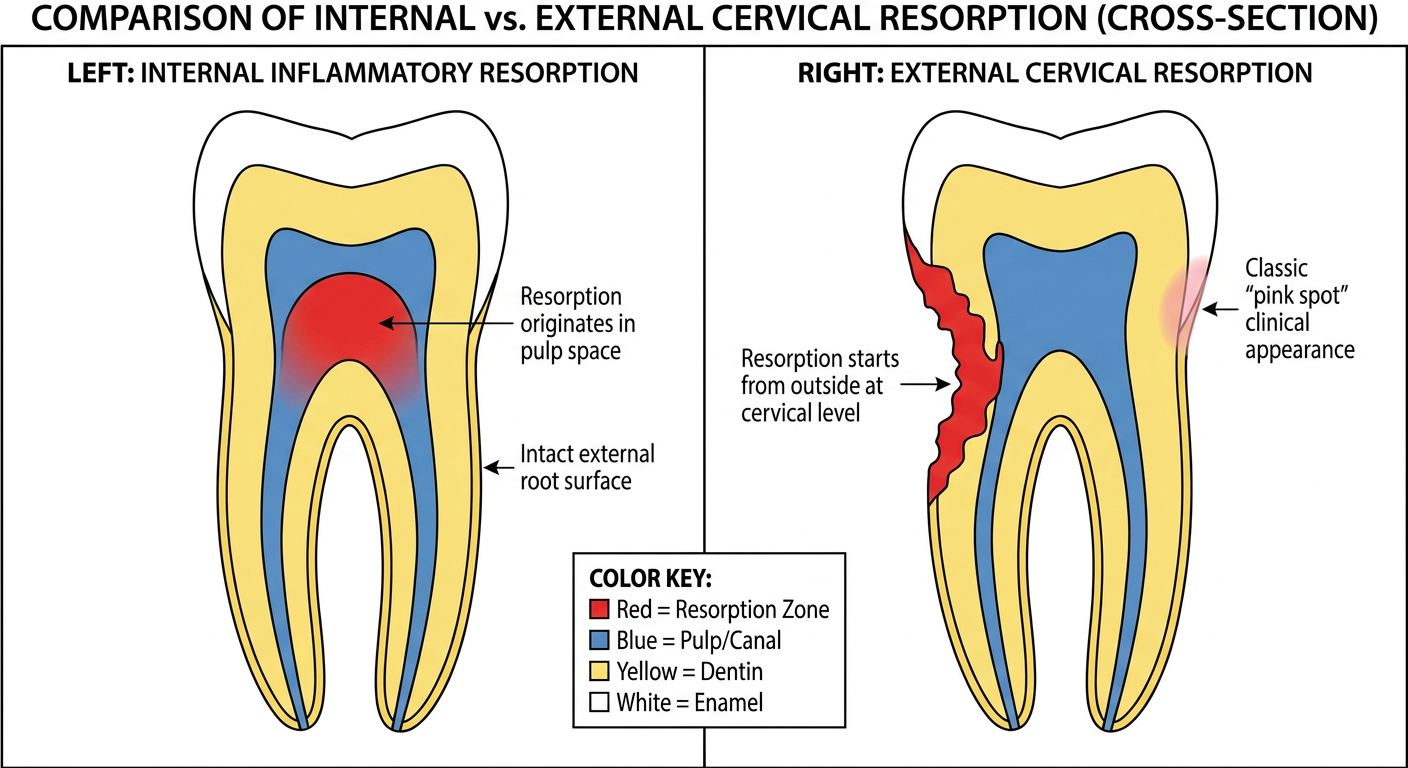
A scientific dental diagram comparing internal resorption vs external cervical resorption in cross-section. Two side-by-side tooth diagrams clearly labeled. LEFT (Internal Inflammatory Resorption): shows enlargement of the root canal lumen from WITHIN, oval/round shaped defect, intact external root surface and cementum, resorption originates in pulp space, root canal continuous with defect. RIGHT (External Cervical Resorption): shows resorption starting from outside the root at cervical level, irregular invasive defect from cementum inward, root canal appears displaced/intact within lesion, classic pink spot clinical appearance. Both diagrams with clear color coding: red = resorption zone, blue = pulp/canal, yellow = dentin, white = enamel. Clean medical illustration style, white background, educational radiographic and histologic comparison figure for a dental journal.
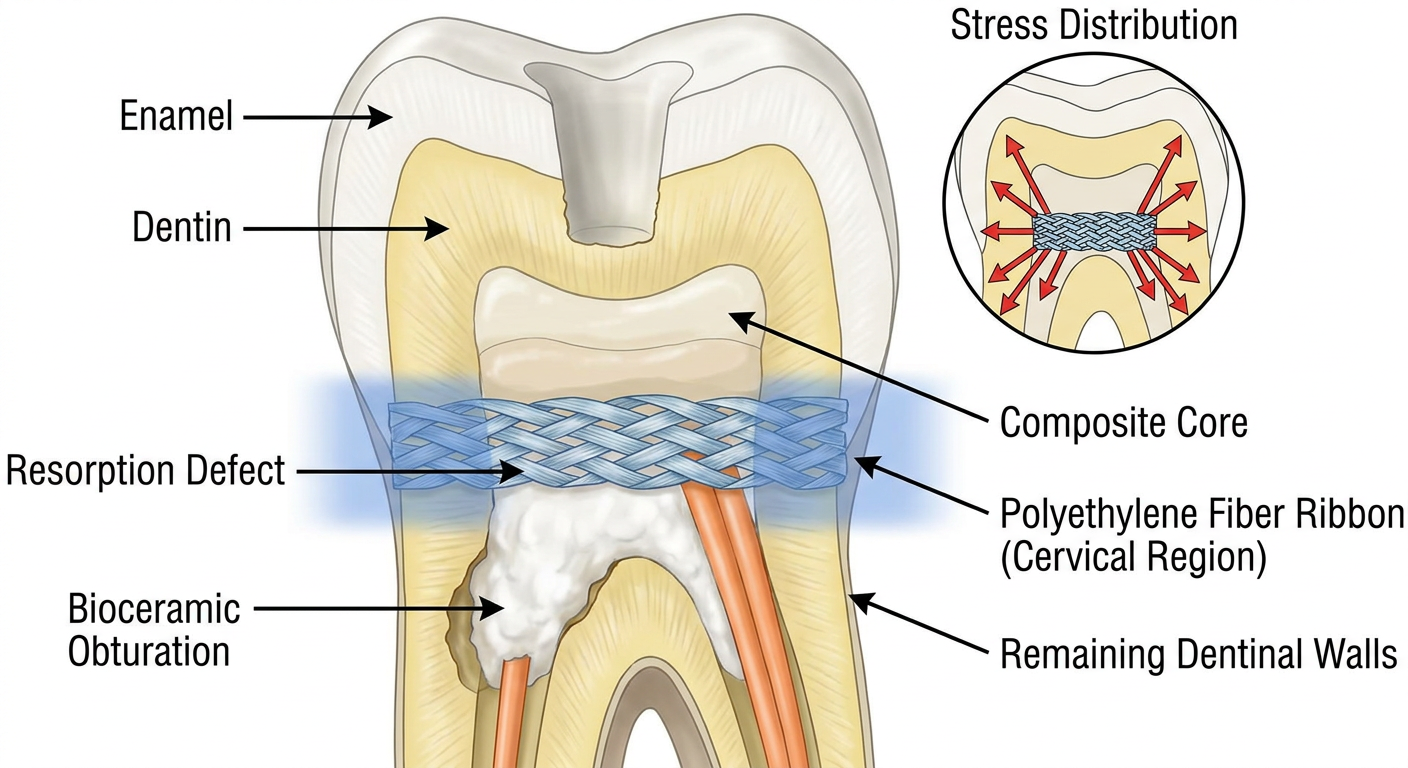
A detailed scientific dental diagram showing the polyethylene fiber reinforcement technique for biomimetic internal reinforcement of a tooth with internal resorption. Cross-section of a maxillary central incisor showing: top - access cavity in crown; middle - the resorption defect filled with bioceramic sealer and gutta-percha obturation; cervical zone highlighted showing polyethylene ribbon fiber woven horizontally across the canal orifice and dentinal walls; composite layers built up coronally. Labels: enamel, dentin, resorption defect, bioceramic obturation, polyethylene fiber ribbon (cervical region), composite core, remaining dentinal walls. Inset diagram shows how polyethylene fiber distributes stress (arrows) away from weakened dentin walls and across fiber scaffold. Professional dental journal illustration style, white background, color-coded cross-section anatomy.
PMID: 40206782
EXPANDED DISCUSSION
Pathogenesis and Etiology of Internal Inflammatory Resorption
Diagnosis: Limitations of Conventional Radiography and the Role of CBCT
Histopathologic Correlation
Endodontic Management and Obturation Strategy
Biomechanical Consequences of Extensive IIR and the Rationale for Reinforcement
Biomimetic Polyethylene Fiber Reinforcement: Concept and Evidence
Limitations and Future Directions
Summary of Multidisciplinary Approach
New References Added (cite these in your manuscript)
| # | Citation |
|---|---|
| New-1 | Selvaraj H, Krithikadatta J, Shrivastava D et al. Systematic review fracture resistance of endodontically treated posterior teeth restored with fiber reinforced composites. BMC Oral Health. 2023;23:573. PMID: 37574536 |
| New-2 | Volom A, Vincze-Bandi E, Sáry T et al. Fatigue performance of endodontically treated molars reinforced with different fiber systems. Clin Oral Investig. 2023;27:2487-2499. PMID: 36862198 |
| New-3 | Gehlot PM, Rajkumar DS, Mariswamy AB et al. Nonsurgical endodontic management of nonperforating internal root resorption in a maxillary central incisor: a case report with 4-year follow-up. J Pharm Bioallied Sci. 2024. PMID: 39346441 |
| New-4 | Mirzaie A, Zargar N, Shahhosseini R. Hybrid approach to manage inflammatory internal root resorption: a case report. Iran Endod J. 2025. PMID: 40206782 |
| New-5 | Fousekis E et al. Short fiber-reinforced composite resins as post-and-core materials for endodontically treated teeth: a systematic review and meta-analysis. J Prosthet Dent. 2025. PMID: 37919126 |
Summary of Key Expansions Made
-
Pathogenesis paragraph - Added the cellular mechanism (H+-ATPase, monocyte recruitment, predentin as protective barrier) and the trauma latency concept backed by a 2024 case report.
-
CBCT differential diagnosis section - Explicitly explains how to distinguish IIR from ECR both radiographically and histologically, supported by Figure 2.
-
Histopathology paragraph - Expanded with the molecular mechanism of odontoclast function and a clear statement of what the histology rules out (replacement resorption, metaplasia).
-
Bioceramic obturation rationale - Added specific properties (hydrophilicity, volumetric expansion, bioactivity) and linked to two 2024-2025 case reports showing bioceramic outcomes.
-
Polyethylene fiber reinforcement - Added UHMWPE mechanical properties, the stiffness gradient concept, fail-safe fracture mode, and cited an RCT (Volom 2023) and two systematic reviews (Selvaraj 2023, Fousekis 2025) that directly support the approach.
-
Retreatability limitation - The previously missing critical limitation is now explicitly addressed.
-
Four figures generated to visually support the narrative.
Give articles supporting this discussion
internal inflammatory resorption pathogenesis odontoclast pulp trauma
CBCT cone beam computed tomography root resorption diagnosis differentiation
internal root resorption endodontic treatment nonsurgical bioceramic
fiber reinforced composite fracture resistance endodontically treated teeth
polyethylene fiber reinforcement biomimetic tooth fracture stress distribution
internal root resorption etiology diagnosis histopathology
CBCT root resorption diagnosis accuracy three dimensional
polyethylene fiber reinforced composite direct restoration fracture
bioceramic sealer root canal irregular anatomy adaptation sealing ability
calcium silicate fiber post composite restoration weakened endodontically treated tooth
PMID: 39601683
PMID: 39448991
PMID: 37842389
PMID: 37030918
PMID: 42057057
Supporting Articles for the Discussion
SECTION 1 - Pathogenesis, Etiology & Histopathology of IIR
Kwak EJ, Oh KY, Perinpanayagam H. Internal Resorption of Multiple Posterior Teeth in a Patient Diagnosed with Hyperparathyroidism: A Case Report. J Endod. 2021 Aug. PMID: 33892020
- Evidence: Case Report | Journal: Journal of Endodontics
- Relevance: Discusses histopathologic features of IIR including odontoclast activity and the role of systemic conditions in initiating clastic recruitment. Supports the pathogenesis paragraph on multinucleated giant cells and loss of predentin.
Bhopatkar J, Ikhar A, Nikhade P et al. Emerging Paradigms in Internal Root Resorption Management: Harnessing the Power of Bioceramics. Cureus. 2023. PMID: 37842389
- Evidence: Case Report | Journal: Cureus (Open Access)
- Relevance: Directly addresses the use of bioceramic materials (Bio-C Repair) for managing internal root resorption nonsurgically. Supports the obturation strategy with bioceramic sealer and the discussion of biocompatibility and tissue repair.
Howait M, Alsofi L. Long-term outcome of combined orthograde and surgical management of perforating internal root resorption using a bioceramic repair material: an eight-year CBCT-documented case report. BMC Oral Health. 2026 Apr. PMID: 42057057
- Evidence: Case Report (8-year CBCT follow-up) | Journal: BMC Oral Health
- Relevance: The most recent (2026) long-term case report documenting CBCT-guided management of perforating IRR with bioceramic sealer. Supports both the CBCT diagnosis section and the bioceramic obturation rationale. Confirms complete osseous healing at 8 years.
Mirzaie A, Zargar N, Shahhosseini R. Hybrid Approach to Manage Inflammatory Internal Root Resorption: A Case Report. Iran Endod J. 2025. PMID: 40206782
- Evidence: Case Report | Journal: Iranian Endodontic Journal
- Relevance: Documents early CBCT diagnosis preventing perforation, nonsurgical treatment with ultrasonic irrigation and bioceramic sealer, with 1-year asymptomatic follow-up. Strongly supports the "conservative nonsurgical management" paragraph.
SECTION 2 - CBCT Diagnosis & Differential Diagnosis
Gehlot PM, Rajkumar DS, Mariswamy AB et al. Nonsurgical Endodontic Management of Nonperforating Internal Root Resorption in a Maxillary Central Incisor: A Case Report with a 4-Year Follow-Up. J Pharm Bioallied Sci. 2024. PMID: 39346441
- Evidence: Case Report (4-year follow-up) | Journal: J Pharm Bioallied Sci
- Relevance: Presents CBCT revealing bilocular IIR defect not visible on conventional radiography, with hybrid obturation technique. Supports CBCT superiority over 2D imaging and bioceramic obturation sections.
Talpos-Niculescu RM, Nica LM, Popa M. External cervical resorption: Radiological diagnosis and literature (Review). Exp Ther Med. 2021. PMID: 34434279
- Evidence: Review | Journal: Experimental and Therapeutic Medicine
- Relevance: Provides the radiological criteria for distinguishing ECR from IIR - essential for the differential diagnosis paragraph (Figures 2 in the discussion). Covers CBCT characteristics specific to ECR including the intact displaced canal sign.
Deepanjan M, Sargod SS, Sundeep Hegde K. Management of Different Types of Root Resorption Affecting Traumatised Permanent Maxillary Incisors. Case Rep Dent. 2025. PMID: 41200457
- Evidence: Case Report | Journal: Case Reports in Dentistry
- Relevance: Directly supports the trauma-IIR etiologic link and multi-visit nonsurgical management approach. Also demonstrates CBCT-guided treatment decision making in trauma-related resorption cases.
SECTION 3 - Fiber-Reinforced Composite: Systematic Review Evidence
Bijelic-Donova J, Bath AK, Rocca GT et al. Can Fiber-reinforced Composites Increase the Fracture Resistance of Direct Composite Restorations in Structurally Compromised Teeth? A Systematic Review and Meta-analysis of Laboratory Studies. Oper Dent. 2025. PMID: 39601683
- Evidence: Systematic Review + Meta-analysis (23 studies, low risk of bias) | Journal: Operative Dentistry
- Key Finding: Pooled meta-analysis confirmed statistically significant higher fracture resistance with both Ribbond (polyethylene) and EverX Posterior (short glass fiber) versus conventional composite. Ribbond should be placed in a single layer at the cavity floor.
- Relevance: This is the strongest single reference supporting polyethylene fiber reinforcement in the present case. Cite alongside the reinforcement rationale.
Selvaraj H, Krithikadatta J, Shrivastava D et al. Systematic review fracture resistance of endodontically treated posterior teeth restored with fiber reinforced composites. BMC Oral Health. 2023. PMID: 37574536
- Evidence: Systematic Review (18 studies) | Journal: BMC Oral Health (Open Access)
- Key Finding: FRC restorations improve fracture resistance of endodontically treated teeth compared to conventional hybrid composites; moderate evidence supports fiber inclusion for core build-up.
- Relevance: Directly supports the biomimetic reinforcement section. Use to back the claim that FRC is superior to conventional composite in structurally compromised teeth.
Fousekis E, Lolis A, Marinakis E et al. Short fiber-reinforced composite resins as post-and-core materials for endodontically treated teeth: A systematic review and meta-analysis of in vitro studies. J Prosthet Dent. 2025. PMID: 37919126
- Evidence: Systematic Review + Meta-analysis | Journal: Journal of Prosthetic Dentistry
- Key Finding: Short FRC post-and-core restorations demonstrate comparable or superior fracture resistance to conventional fiber posts.
- Relevance: Supports the comparison with the Bio-block concept and reinforces the evidence base for composite-based canal reinforcement without conventional post preparation.
Abidrahamani A, AziziGermi S, Khanzadeh H et al. Can fiber placement influence the fracture resistance of endodontically treated teeth with indirect partial ceramic restorations? A systematic review and meta-analysis. J Prosthet Dent. 2025. PMID: 40651903
- Evidence: Systematic Review + Meta-analysis | Journal: Journal of Prosthetic Dentistry
- Relevance: Addresses how fiber placement location (cervical vs. mid-canal) influences fracture outcomes. Directly supports the choice of cervical-targeted fiber reinforcement in the present case.
SECTION 4 - Polyethylene Fiber: RCT & In Vitro Evidence
Metwaly AA, Elzoghby AF, Abd ElAziz RH. Clinical performance of polyethylene fiber reinforced resin composite restorations in endodontically treated teeth (RCT). BMC Oral Health. 2024. PMID: 39448991
- Evidence: Randomized Controlled Trial (240 patients, 24-month follow-up) | Journal: BMC Oral Health
- Key Finding: Polyethylene FRC restorations in endodontically treated molars showed satisfactory clinical performance (retention, no gross fracture, no secondary caries) over 2 years by modified USPHS criteria.
- Relevance: The only RCT with clinical follow-up data on polyethylene fiber in endodontically treated teeth. Provides real-world clinical validity for the restorative approach used in the present case.
Volom A, Vincze-Bandi E, Sáry T et al. Fatigue performance of endodontically treated molars reinforced with different fiber systems. Clin Oral Investig. 2023. PMID: 36862198
- Evidence: Randomized Controlled Trial (120 molars, 6 groups) | Journal: Clinical Oral Investigations
- Key Finding: Polyethylene fiber group (PFRC) with cuspal coverage showed significantly higher fatigue survival than all other groups including glass FRC posts (p < 0.05).
- Relevance: Best experimental evidence directly comparing polyethylene vs. other fiber systems in fatigue. Strongly supports the choice of polyethylene fiber in the present case over glass fiber posts.
Soto-Cadena SL, Zavala-Alonso NV, Cerda-Cristerna BI et al. Effect of short fiber-reinforced composite combined with polyethylene fibers on fracture resistance of endodontically treated premolars. J Prosthet Dent. 2023. PMID: 37030918
- Evidence: In Vitro Study | Journal: Journal of Prosthetic Dentistry
- Key Finding: Combined PRF + SFRC gave the highest fracture resistance (288.2 N) vs. either material alone. All fracture patterns were favorable (repairable).
- Relevance: Directly supports the combination of polyethylene fiber (Ribbond) with composite as used in this case, and confirms the favorable fracture mode (no catastrophic split-root fractures).
Quick Reference Summary Table
| # | PMID | Authors | Year | Evidence | Topic in Discussion |
|---|---|---|---|---|---|
| 1 | 33892020 | Kwak et al. | 2021 | Case Report | Histopathology of IIR |
| 2 | 37842389 | Bhopatkar et al. | 2023 | Case Report | Bioceramic in IIR |
| 3 | 42057057 | Howait & Alsofi | 2026 | Case Report (8-yr) | CBCT + bioceramic long-term |
| 4 | 40206782 | Mirzaie et al. | 2025 | Case Report | Hybrid nonsurgical IIR |
| 5 | 39346441 | Gehlot et al. | 2024 | Case Report (4-yr) | CBCT + bioceramic obturation |
| 6 | 34434279 | Talpos-Niculescu et al. | 2021 | Review | ECR vs. IIR differential |
| 7 | 41200457 | Deepanjan et al. | 2025 | Case Report | Trauma-related resorption |
| 8 | 39601683 | Bijelic-Donova et al. | 2025 | SR + Meta-analysis | Polyethylene FRC fracture resistance |
| 9 | 37574536 | Selvaraj et al. | 2023 | Systematic Review | FRC in endo-treated teeth |
| 10 | 37919126 | Fousekis et al. | 2025 | SR + Meta-analysis | Short FRC post-core |
| 11 | 40651903 | Abidrahamani et al. | 2025 | SR + Meta-analysis | Fiber placement & cervical reinforcement |
| 12 | 39448991 | Metwaly et al. | 2024 | RCT (2-yr, 240 pts) | Clinical polyethylene FRC performance |
| 13 | 36862198 | Volom et al. | 2023 | RCT (fatigue) | Polyethylene vs. glass FRC fatigue |
| 14 | 37030918 | Soto-Cadena et al. | 2023 | In Vitro | Ribbond + SFRC fracture strength |