make a presentation from the given topic from basic to advances, clinical trials, recent advances. No need to make a file, just write in chat with pictures
Reading File
Running Command
Running Command
Running Command
Searching PubMed
age-related macular degeneration treatment advances
Searching the Web
AMD age-related macular degeneration anatomy diagram retinal layers RPE drusen
Loading Image
Loading Image
Searching the Web
geographic atrophy OCT imaging AMD anti-VEGF faricimab 2024 clinical trial
Loading Image
Loading Image
Searching the Web
complement inhibitor pegcetacoplan syfovre geographic atrophy dry AMD gene therapy stem cell
Loading Image
Loading Image
Searching the Web
AMD drusen fundus photograph OCT scan macular degeneration types classification
I now have comprehensive content. Let me deliver the full presentation.
🔬 Age-Related Macular Degeneration (AMD)
A Comprehensive Presentation - Basics to Recent Advances
🏛️ SLIDE 1 - Introduction & Scope
Age-Related Macular Degeneration (AMD) is the leading cause of irreversible central vision loss in the developed world and the third most common globally.
- ~196 million people affected worldwide (2020), projected to rise to 288 million by 2040
- Causes quality of life decline comparable to end-stage prostate cancer or a bedridden stroke
- Advanced AMD costs billions in health resources annually
- Prevention and early treatment are top public health priorities
🧬 SLIDE 2 - Anatomy of the Macula
The macula sits at the center of the retina, responsible for high-acuity central vision. Understanding the layers it depends on is essential to AMD.

The critical anatomical complex involved in AMD is:
| Layer | Function |
|---|---|
| Photoreceptors (cones & rods) | Detect light and color; cones concentrate in the fovea |
| RPE (Retinal Pigment Epithelium) | Nurtures photoreceptors, phagocytoses shed outer segments, forms outer blood-retinal barrier |
| Bruch's Membrane (BrM) | Basement membrane separating RPE from choroid; conduit for nutrients/waste |
| Choriocapillaris | Fenestrated capillary bed supplying the outer retina |
In AMD, this complex breaks down - waste accumulates, RPE dysfunctions, and the choroid thins or invades.
📊 SLIDE 3 - Classification & Staging
The AMD staging system is based on drusen size and pigmentary changes:

| Grade | Stage | Key Features |
|---|---|---|
| Grade 1 | Subclinical AMD | Drusen <63 µm; impaired dark adaptation only |
| Grade 2 | Early AMD | Small-medium drusen (<125 µm); pigmentary abnormalities |
| Grade 3 | Intermediate AMD | Large drusen >125 µm; significant pigmentary changes |
| Grade 4 | Advanced Dry (GA) | Geographic atrophy - RPE loss, no CNV |
| Grade 5 | Advanced Wet (nAMD) | Macular neovascularization (MNV) with exudation |
🔬 SLIDE 4 - Pathogenesis (The "Deposit-Driven Disease")
AMD is fundamentally a deposit-driven disease. The key pathologic deposits form between the RPE and Bruch's membrane.
Drusen Formation
- The RPE continuously recycles lipids, outer segment debris, and metabolites
- With aging, Bruch's membrane thickens and hydraulic conductivity falls
- Uncleared waste accumulates as soft drusen (the hallmark of AMD risk)
- Lipid content in Bruch's membrane increases exponentially after the 4th decade - phospholipids, triglycerides, free cholesterol
- Peroxidized lipids (from DHA, linolenic acid in photoreceptor outer segments) drive angiogenic cytokines, triggering neovascularization
Key Molecular Pathways
- Complement dysregulation - inappropriate activation damages RPE and choriocapillaris
- Lipid/cholesterol metabolism - lipid accumulation impairs RPE function
- Oxidative stress - mitochondrial ROS damages the RPE
- VEGF upregulation - hypoxic RPE secretes VEGF-A, driving choroidal neovascularization (CNV)
- Inflammation/inflammasome - NLRP3 activation in RPE, macrophage infiltration
Drusen Subtypes
| Type | Location | Significance |
|---|---|---|
| Hard drusen | Sub-RPE | Small, low risk |
| Soft drusen | Sub-RPE | Large, high risk for progression |
| Subretinal drusenoid deposits (SDD) | Above RPE | Associated with rod dysfunction, GA risk |
| Basal linear deposits (BLinD) | Within BrM | Diffuse lipid accumulation |
| Pachydrusen | Sub-RPE | Linked to polypoidal choroidal vasculopathy |
🧪 SLIDE 5 - Risk Factors
Non-Modifiable
- Age - strongest risk factor. 5% of >75 yr olds have late AMD vs <0.1% in 50-55 yr olds
- Genetics - CFH, ARMS2/HTRA1, C3, CFB - heritability ~50-70%
- Ethnicity - White Europeans highest prevalence (~12%); African Americans lowest (~2.5%)
- Sex - slightly higher in females (partly longevity)
- Iris color/hyperopia - lighter iris, hyperopia = increased risk; myopia = protective
Modifiable
- Smoking - 2-4x increased risk; most powerful modifiable factor. Risk persists years after cessation. Up to 25% of female AMD cases attributable to smoking
- Diet - Mediterranean diet protective; omega-3 fatty acids, leafy greens (lutein/zeaxanthin) reduce risk
- AREDS supplements (Vitamins C, E, beta-carotene, zinc) reduce progression in intermediate AMD by ~25%
- Cardiovascular risk factors - HTN, obesity, sedentary lifestyle associated
- UV/blue light - some association, less consistent evidence
🏥 SLIDE 6 - Clinical Presentation & Symptoms
Symptoms by Stage
Early/Intermediate (Non-neovascular)
- Often asymptomatic or mild
- Impaired dark adaptation (night vision difficulty) - often the first functional sign
- Subtle color/contrast changes
- Found incidentally on funduscopy
Geographic Atrophy (Advanced Dry)
- Progressive central visual field loss
- Loss worsens as GA enlarges toward fovea
- Reading and facial recognition become difficult
- Bilateral in most patients
Neovascular (Wet) AMD
- Sudden metamorphopsia (visual distortion) - Amsler grid test positive
- Rapid central vision loss (days to weeks)
- Central scotoma
- Subretinal fluid/hemorrhage
🔭 SLIDE 7 - Diagnosis & Imaging
Clinical Tools
1. Fundus Photography (Color)
- Identifies drusen, RPE changes, hemorrhage, exudate
2. Fluorescein Angiography (FA)
- Was gold standard for CNV detection
- Hyperfluorescent leakage = active neovascularization
- Classifies CNV as classic (well-demarcated leakage), occult (late ill-defined), or mixed
3. Indocyanine Green Angiography (ICGA)
- Better visualization of type 1 (sub-RPE) MNV and polypoidal choroidal vasculopathy
- Detects late hypofluorescence in GA
4. Optical Coherence Tomography (OCT) - The Modern Standard
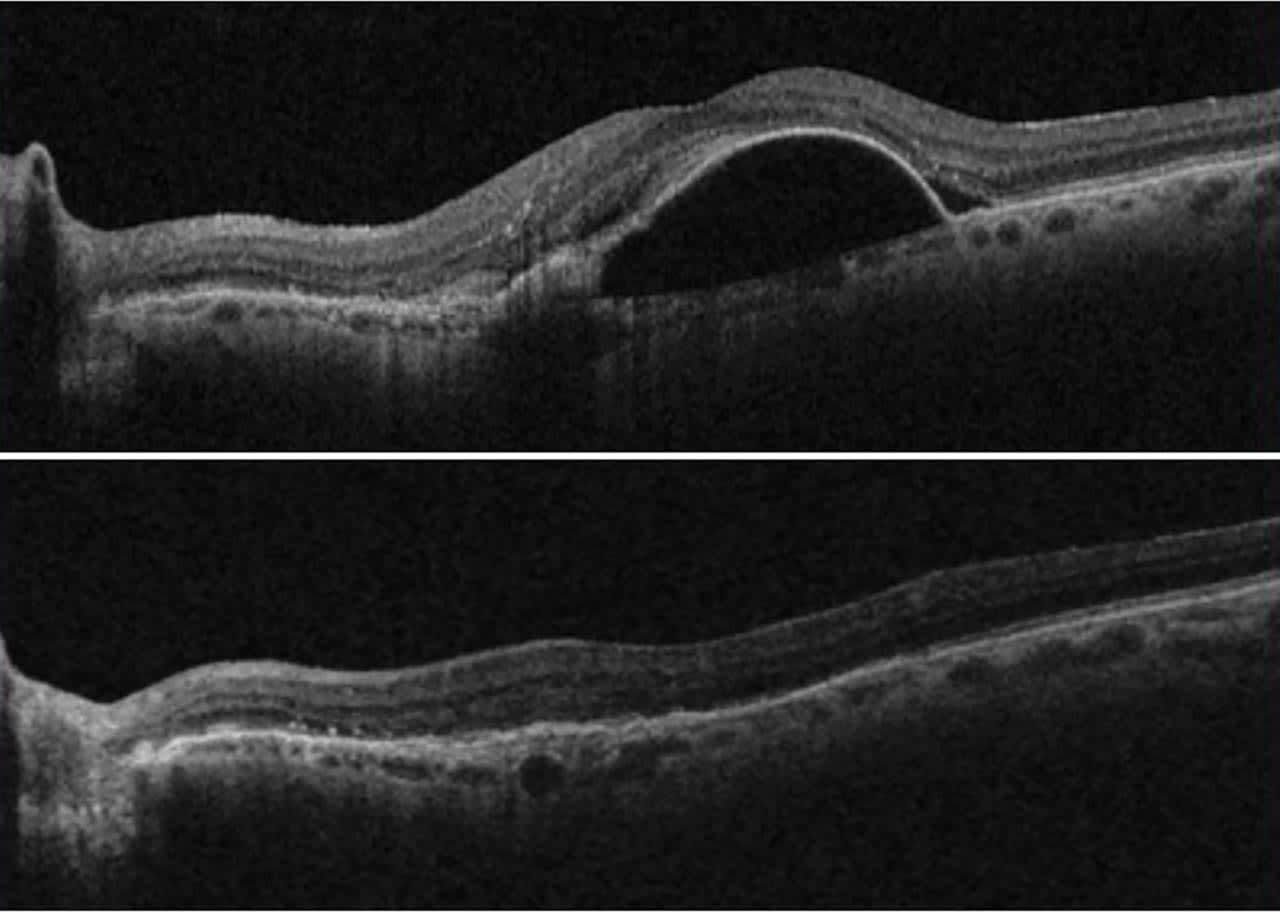
- Cross-sectional microstructural imaging at 5-10 µm resolution
- Identifies: drusen, subretinal fluid (SRF), intraretinal fluid (IRF), fibrovascular PED, RPE atrophy, EZ (ellipsoid zone) integrity
- Key OCT biomarkers for progression risk: hyperreflective foci (strongest single predictor), subretinal drusenoid deposits, drusen volume >0.03 mm³ in the central 3 mm circle
5. OCT-Angiography (OCTA)
- Non-invasive, dye-free angiography
- Visualizes flow in all retinal layers
- Detects MNV subtypes precisely: Type 1 (sub-RPE plaque), Type 2 (subretinal "glomerulus"), Type 3 (intraretinal tuft)
- Detects "nascent" type 3 MNV as hyperreflective foci with flow
6. Fundus Autofluorescence (FAF)
- Lipofuscin distribution maps
- Hypoautofluorescence = RPE loss (GA)
- Junctional hyperautofluorescence = active GA border (fastest growth zone)
🩺 SLIDE 8 - Types of Macular Neovascularization (MNV)
| MNV Type | Location | Old Name | Angiographic Appearance |
|---|---|---|---|
| Type 1 | Sub-RPE | "Occult CNV" | Fibrovascular PED; late leakage; plaques on ICGA |
| Type 2 | Subretinal (above RPE) | "Classic CNV" | Hot spot; brisk early leakage on FA |
| Type 3 | Intraretinal | "RAP" (Retinal Angiomatous Proliferation) | Deep retinal tuft; often bilateral |
- Wet AMD (diagram below) - abnormal vessels breach the RPE, leading to leakage and hemorrhage

Type 1 MNV may actually be neuroprotective in early stages - proposed to act as a surrogate choriocapillaris, supporting hypoxic RPE. It only becomes harmful when it exudes fluid.
💊 SLIDE 9 - Treatment of Neovascular AMD (Wet AMD)
Pre-anti-VEGF Era (Historical)
- Laser photocoagulation - direct ablation of CNV; not useful for subfoveal lesions
- Photodynamic therapy (PDT) with Verteporfin - selective vessel closure; largely replaced but still used for polypoidal CVP
- Pegaptanib (Macugen) - first anti-VEGF (VEGF-165 selective); modest results; 2004 FDA approval
Anti-VEGF Era - The Revolution
The introduction of intravitreal anti-VEGF injections transformed nAMD from a blinding disease to a manageable one.
| Drug | Mechanism | Key Trials | Outcomes |
|---|---|---|---|
| Bevacizumab (Avastin) | Full IgG; binds all VEGF-A isoforms | CATT, IVAN | Non-inferior to ranibizumab; off-label; ~$50/inj |
| Ranibizumab (Lucentis) | Fab fragment; all VEGF-A | ANCHOR, MARINA, PIER, CATT | +8-11 letters at 1yr; monthly; ~$2000/inj |
| Aflibercept (Eylea) | VEGF trap (binds VEGF-A, B, PlGF) | VIEW 1, VIEW 2 | Non-inferior to ranibizumab; q8wk dosing |
| Brolucizumab (Beovu) | scFv antibody; high concentration | HAWK, HARRIER | q12wk dosing; risk of vasculitis (rare) |
| Faricimab (Vabysmo) | Bispecific: anti-VEGF-A + anti-Ang-2 | TENAYA, LUCERNE | Up to q16wk dosing; 46% on q16wk at 2yrs |
Dosing Regimens
- Monthly fixed - best outcomes, least practical
- PRN (as needed) - fewer injections, slightly worse visual outcomes
- Treat-and-Extend (T&E) - gold standard in practice; extends intervals if dry, contracts if recurrence
- Individualized maintenance - based on monitoring
CATT Trial Key Findings (2yr data)
- Bevacizumab and ranibizumab were equivalent for visual acuity
- Continuous > PRN dosing (discontinuous dosing = ~2.4 letters less gained)
- Mean gain: ranibizumab monthly = +8.8 letters; bevacizumab monthly = +7.8 letters
🧠 SLIDE 10 - Treatment of Geographic Atrophy (Dry AMD)
AREDS / AREDS2 Supplements
The Age-Related Eye Disease Study (AREDS) was a landmark NIH-sponsored trial:
- AREDS formula: Vitamin C 500mg, Vitamin E 400 IU, Beta-carotene 15mg, Zinc 80mg
- 25% risk reduction of progression from intermediate to advanced AMD at 5 years
- AREDS2 replaced beta-carotene (lung cancer risk in smokers) with lutein/zeaxanthin 10/2mg
2023 - First-Ever FDA Approvals for GA: A Milestone
GA had no approved treatment for decades. The complement system was identified as the key driver via AMD genetics (CFH, C3, C5 variants), leading to complement inhibitor trials.
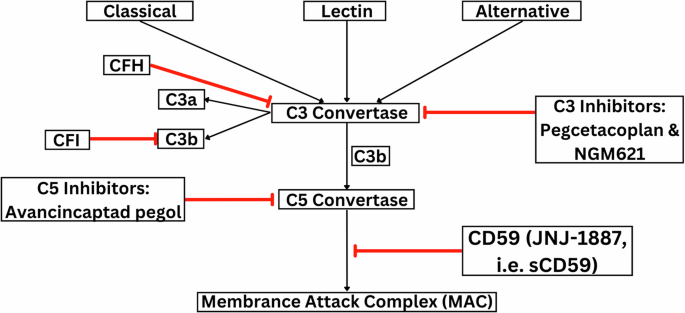
| Drug | Target | Trial | Outcome |
|---|---|---|---|
| Pegcetacoplan (Syfovre) | C3 inhibitor (complement) | OAKS, DERBY | ~22% GA growth reduction at 24mo (monthly); FDA approved Feb 2023 |
| Avacincaptad pegol (Izervay) | C5 inhibitor | GATHER1, GATHER2 | ~14-18% GA growth reduction; FDA approved Aug 2023 |
Important caveat: Both drugs slow the rate of GA expansion on fundus autofluorescence, but neither has demonstrated a statistically significant improvement in visual acuity. The clinical significance of slowing lesion growth without demonstrable visual benefit remains a subject of debate. Side effects include increased risk of new-onset neovascular AMD (conversion to wet AMD).
🚀 SLIDE 11 - Advanced Drug Delivery Systems
A major limitation of anti-VEGF therapy is the injection burden (8-12 per year). Several innovations aim to reduce this:
Port Delivery System (PDS) with Ranibizumab (Susvimo)
- Surgically implanted sustained-release ocular device
- Placed in the pars plana, contains a drug reservoir
- Refilled in-office every ~6 months
- LADDER trial (Phase 2) and ARCHWAY trial (Phase 3) demonstrated non-inferiority to monthly ranibizumab
- FDA approved October 2021; voluntary withdrawal Feb 2022 (device issues); reapproved 2023
High-Concentration Formulations
- Aflibercept 8mg (Eylea HD) - higher dose allows q12-16wk dosing; FDA approved 2023 (PULSAR trial)
Sustained-Release Implants / Biodegradable Systems
- Graybug Vision sunitinib implant (Phase 2)
- Clearside Biomedical axitinib suprachoroidal injection
- Goal: 6-month or longer dosing intervals
🧬 SLIDE 12 - Gene Therapy for AMD
Gene therapy aims for a "one-and-done" injection that provides permanent anti-VEGF delivery.
| Product | Target | Vector | Stage |
|---|---|---|---|
| RGX-314 (RegenxBio) | Anti-VEGF protein (ranibizumab-like) | AAV8, subretinal | Phase 2/3 (ATMOSPHERE, ABBRIATA trials) |
| ADVM-022 (Adverum) | Aflibercept gene | AAV.7m8, intravitreal | Phase 1 (OPTIC trial) |
| 4D-150 | Anti-VEGF-A + VEGF-C | Intravitreal AAV | Phase 2 (PRISM trial) |
- RGX-314 subretinal injection showed sustained anti-VEGF protein expression for 2+ years with reduced injection need
- Gene therapy for dry AMD: GT005 (Gyroscope/Novartis) - CFI gene for complement regulation; Phase 2 data showed safety, efficacy signals
- OCU410 - nuclear receptor RORa gene therapy for dry AMD; Phase 1/2 ongoing
🔬 SLIDE 13 - Cell-Based Therapies & Regenerative Medicine
Stem Cell / RPE Cell Replacement
The concept: replace degenerated RPE with new cells to rescue photoreceptors before they die.
| Product | Cell Source | Delivery | Stage |
|---|---|---|---|
| OpRegen (Lineage Cell Therapeutics) | hESC-derived RPE | Subretinal surgical injection | Phase 1/2a (NCT02286089, NCT05626114) |
| MA09-hRPE (Astellas) | hESC-derived RPE | Subretinal | Phase 1/2 |
| iPSC-RPE (Japan/RIKEN) | Patient's own iPSC | Subretinal sheet | Phase 1 (autologous) |
- OpRegen Phase 1/2 results: Patients with advanced GA showed signs of vision stabilization and improved RPE coverage on OCT
- Key challenge: immune rejection (allogeneic), engraftment efficiency, and host integration
🖥️ SLIDE 14 - Multimodal Imaging & AI Diagnostics
The Imaging Revolution
OCT has become the cornerstone of AMD management - >80% of retreatment decisions in the CATT trial were guided by OCT rather than FA.
Key OCT Biomarkers (Systematic Review - Hanson et al., Eye 2023, PMID 36526863):
- Intraretinal fluid (IRF) - strongest predictor of poor visual outcome
- Subretinal hyperreflective material (SHRM) - fibrovascular activity
- Hyperreflective foci (HRF) - strongest single OCT predictor of progression to late AMD
- Outer retinal atrophy (ORA) - precursor state to complete RPE and outer retinal atrophy (cRORA)
AI / Deep Learning in AMD
A growing body of evidence demonstrates that deep learning models trained on OCT images can:
- Predict conversion from early to advanced AMD (outperforming clinical grading)
- Quantify GA area automatically
- Grade drusen and pigmentary changes
- Recommend retreatment decisions
Google DeepMind's study (2018) demonstrated AI-equivalent-to-expert retinal specialist performance at diagnosing and referring AMD from OCT scans.
💉 SLIDE 15 - Clinical Trials Landscape (2023-2026)
Neovascular AMD - Emerging Agents
| Drug | Mechanism | Trial | Status |
|---|---|---|---|
| Faricimab (Vabysmo) | Anti-VEGF-A + Anti-Ang-2 (bispecific) | TENAYA/LUCERNE | Approved 2022; 46% q16wk at 2yr |
| Aflibercept 8mg (Eylea HD) | VEGF-A/B + PlGF trap, high dose | PULSAR | Approved 2023; q12/q16wk |
| Susvimo (PDS ranibizumab) | Sustained release ranibizumab | ARCHWAY | Re-approved 2023 |
| KSI-301 (Kodiak) | Anti-VEGF-A antibody biopolymer conjugate | DAZZLE | Phase 3 (extended durability goal) |
| OPT-302 (Opthea) | Anti-VEGF-C/D | ShORe/COAST | Phase 3 (combination with ranibizumab) |
| Conbercept (Kanghong) | VEGF-A/B + PlGF trap | PANDA-1/2 | Phase 3 (global) |
Geographic Atrophy - Pipeline Beyond Syfovre/Izervay
| Drug | Mechanism | Trial | Stage |
|---|---|---|---|
| ANX007 (Annexon) | Anti-C1q (classical pathway) | SIGLEC | Phase 2/3; early data: 80% patients had VA gains at 3mo |
| Zimura (avacincaptad pegol) | Anti-C5 | GATHER2 | Approved Aug 2023 |
| Emixustat (Acucela) | Visual cycle modulator (RPE65 inhibitor) | Phase 3 SAGA (oral) | Ongoing |
| CT1812 (Cognition) | Sigma-2 receptor inhibitor (oral) | Phase 2 (104wk) | Ongoing |
| GT005 (Gyroscope) | CFI gene delivery (AAV) | FOCUS study | Phase 2 |
| RG6179 (Roche/Genentech) | Anti-HTRA1 antibody | GALLEGO study | Phase 2 |
🧬 SLIDE 16 - Multi-Omics & Genetics (Cutting Edge, 2026)
A 2026 systematic review (Castro-Fernández et al., Survey of Ophthalmology, PMID 41643859) synthesized multi-omics findings in AMD:
Genomics
- Over 50 independent genetic loci associated with AMD risk (GWAS meta-analyses)
- Top associations: CFH (Y402H variant), ARMS2/HTRA1 (chromosome 10q26), C3, C2/CFB, VEGFA, CETP, ABCA1
- Polygenic risk scores can identify individuals in the top 10% of genetic risk - potentially useful for screening
Transcriptomics / Proteomics
- Single-cell RNA sequencing of the human macula identified distinct RPE cell states in AMD
- Upregulation of complement genes, downregulation of RPE signature genes (BEST1, RPE65)
- Plasma proteomics: complement fragments C3d, Ba, Bb elevated even in early AMD
Metabolomics / Lipidomics
- Sphingolipid and ceramide dysregulation in AMD RPE
- Plasma DHA (docosahexaenoic acid) levels inversely correlate with AMD risk
Microbiome
- Gut microbiome dysbiosis (reduced Lactobacillus, increased Prevotella) associated with higher AMD risk - the gut-retina axis
🔭 SLIDE 17 - Visual Rehabilitation & Low Vision
When AMD is advanced and untreatable, vision rehabilitation remains critical.
AREDS Role in Management
AREDS2 supplements only work for intermediate AMD or advanced AMD in one eye - they do not benefit early AMD or those without AMD.
Low Vision Aids
- Optical magnifiers, stand magnifiers, electronic video magnifiers
- Screen-reading software, large-print materials
- Eccentric viewing training - teaches patients to use a preferred retinal locus (PRL) adjacent to the scotoma
- Contrast enhancement filters
Implantable Miniature Telescope (IMT - VisionCare Ophthalmic Technologies)
- Provides 2.2-2.7x magnification of the central visual field
- FDA approved for end-stage AMD (bilateral central GA or stable disciform scar)
- Requires pre-trial of external telescope to confirm benefit
- Monocular implant (one eye for central, fellow eye for peripheral vision)
- Phase 3 trial (21 participants, age 55+): 2/3 of participants gained 2+ lines of vision
📊 SLIDE 18 - Summary: Treatment Algorithm
DIAGNOSIS OF AMD
│
▼
STAGE?
┌────────────────────────────────────────────────────┐
│ │
Early/Intermediate AMD Advanced AMD
│ │
▼ ├── Neovascular (Wet)
AREDS2 Supplements │ │
Monitor q6-12mo with OCT │ ▼
Lifestyle modification │ Anti-VEGF Intravitreal
(quit smoking, diet) │ (Faricimab, Aflibercept 8mg,
│ Ranibizumab, Bevacizumab)
│ Treat-and-Extend Protocol
│
└── Geographic Atrophy (Dry)
│
▼
Pegcetacoplan (Syfovre) or
Avacincaptad pegol (Izervay)
[Monthly or EOMonth injections]
AREDS2 supplements
Low Vision Rehabilitation
Clinical Trial enrollment
🌟 SLIDE 19 - Key Recent Advances Summary (2023-2026)
| Year | Milestone |
|---|---|
| 2022 | Faricimab (bispecific anti-VEGF/Ang2) approved - first new nAMD MOA in a decade |
| 2023 | Pegcetacoplan (Syfovre) - first-ever GA treatment approved (Feb 2023) |
| 2023 | Avacincaptad pegol (Izervay) - second GA treatment approved (Aug 2023) |
| 2023 | Aflibercept 8mg (Eylea HD) approved - q16wk dosing option |
| 2023 | Susvimo (Port Delivery System) re-approved after redesign |
| 2024-2026 | Gene therapy trials (RGX-314, ADVM-022, 4D-150) showing multi-year sustained VEGF suppression |
| 2024-2026 | Multi-omics: gut-retina axis, polygenic risk scores, single-cell transcriptomics in AMD |
| 2025 | Persistence of retinal fluid despite anti-VEGF remains a key challenge (Meta-analysis, PMID 39842717) |
| 2026 | Multi-omics AMD systematic review published (PMID 41643859) |
📚 SLIDE 20 - Key References
- Seddon JM, Sobrin L, Davoudi S. Epidemiology and Risk Factors for AMD. In: Ryan's Retina, 7th ed. Chapter 64.
- Curcio CA. Pathogenesis of AMD. In: Ryan's Retina, 7th ed. Chapter 65.
- Rosenfeld PJ et al. Neovascular AMD. In: Ryan's Retina, 7th ed. Chapter 67.
- Bhisitkul RB. Pharmacotherapy of AMD. In: Ryan's Retina, 7th ed. Chapter 68.
- CATT Research Group. Ranibizumab and Bevacizumab for Neovascular AMD. NEJM 2011.
- Hanson RLW et al. OCT imaging biomarkers in nAMD: systematic review. Eye 2023. [PMID 36526863]
- Vision Loss Expert Group. Global estimates of AMD blindness. Eye 2024. [PMID 38965321]
- Yap DWT et al. Persistence of retinal fluid after anti-VEGF in nAMD. Ophthalmol Retina 2025. [PMID 39842717]
- Castro-Fernández DC et al. Multi-omics in AMD: systematic review. Surv Ophthalmol 2026. [PMID 41643859]
- AAO EyeWiki - Age-Related Macular Degeneration
This presentation covers AMD from basic anatomy through advanced molecular mechanisms, landmark clinical trials, the 2023 GA treatment breakthrough, and the current pipeline through 2026 - based on the AMD textbook chapters provided and supplemented with the latest published evidence.
Create an infographic poster of AMD progression and treatment timeline
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.