Appendix embryology, surgical anatomy arrey veins and lymphatics nerves, types of conditions in acute and chronic, , investigation, pre op thing and post op complications, incisions and other things from Bailey and love
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from Bailey & Love. Let me compile the complete answer.
The Vermiform Appendix - Bailey & Love's Short Practice of Surgery (28th Ed.), Chapter 76
EMBRYOLOGY
The appendix is a derivative of the midgut. The caecum and appendix develop from the caecal bud, which appears in the fifth week of gestation as a swelling on the antimesenteric border of the midgut loop. As the caecum grows, the appendix is left behind as a narrow diverticulum at its apex. The appendix first appears in the eighth week and is recognizable by the third month. Because of differential growth of the caecum, the appendix in the fetus lies at the apex but in later life comes to lie posteromedially.
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 76
SURGICAL ANATOMY
Position of the Base
The base of the appendix is attached to the posteromedial wall of the caecum, where the three taeniae coli converge - this convergence is the key to locating the appendix at surgery. The base lies approximately 2 cm below the ileocaecal valve.
Positions of the Tip (Frequency)
The appendix tip may lie in six positions (order of frequency):
- Retrocaecal / retroileal - most common (~65%)
- Pelvic / descending - 2nd most common (~31%)
- Subcaecal / preileal
- Pre-ileal
- Right paracolic (extraperitoneal)
- Left-sided (in situs inversus or malrotation)
Arteries
The appendicular artery is a branch of the lower division of the ileocolic artery (itself from the superior mesenteric artery). It passes behind the terminal ileum to enter the mesoappendix a short distance from the base, then runs in the free border of the mesoappendix.
Key point: the appendicular artery is essentially an end-artery - thrombosis results in gangrenous appendicitis (infarction/necrosis of the appendix).
An accessory appendicular artery may occasionally be present.
Veins
Venous drainage follows the arterial supply - the appendicular vein drains into the ileocolic vein, then into the superior mesenteric vein, then the portal vein. This is why gangrenous appendicitis can cause portal pyaemia (pylephlebitis) - septicaemia in the portal venous system with resultant intrahepatic abscesses.
Lymphatics
Four, six or more lymphatic channels traverse the mesoappendix and empty into the ileocaecal lymph nodes. The submucosa of the appendix wall also contains numerous lymphatic aggregations (follicles). The prominence of submucosal lymphoid tissue in young adults is thought to be important in the aetiology of appendicitis - lymphoid hyperplasia can obstruct the lumen.
Nerves
Afferent pain fibres from the appendix travel with the sympathetic nerves at the level of T10. This explains why the initial pain of appendicitis is perceived as central, periumbilical (referred visceral pain via T10 dermatome). As inflammation progresses and involves the parietal peritoneum, somatic pain via the local spinal nerves localises to the right iliac fossa (RIF).
Microscopic Anatomy
- Average length: 7.5-10 cm; lumen is irregular with longitudinal folds
- Mucosa: columnar cell intestinal epithelium of colonic type with crypts
- Base of crypts: argentaffin (Kulchitsky) cells - precursors of neuroendocrine tumours (NETs)
- Submucosa: rich in lymphatic follicles
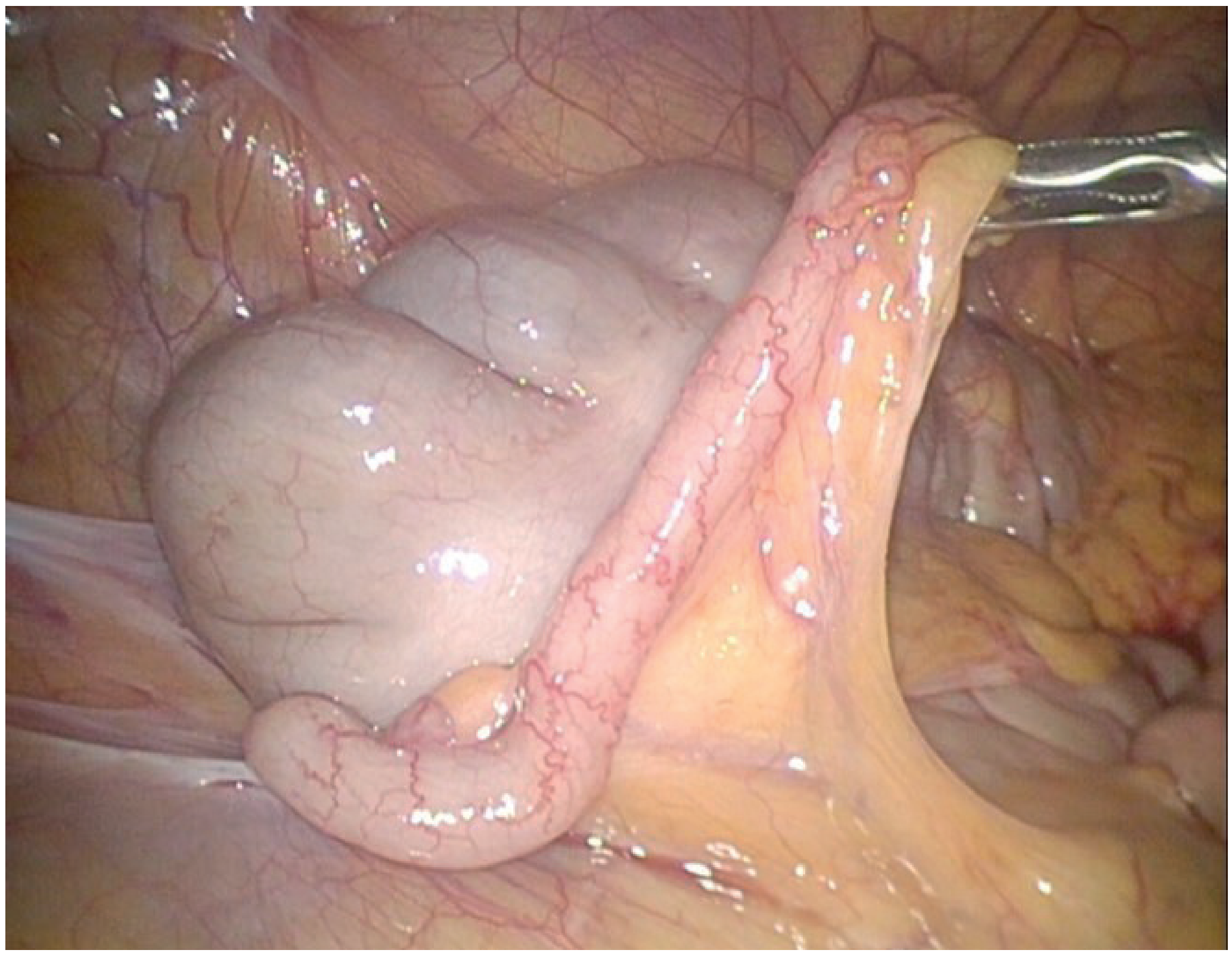
Figure 76.3 - Laparoscopic view of a normal appendix with mesoappendix displaying the appendicular artery (Bailey & Love)
ACUTE APPENDICITIS
Epidemiology
- Most common cause of the acute abdomen in young adults
- Lifetime risk: 8.6% males, 6.7% females
- Peak incidence: teens and early 20s
- M:F ratio rises to 3:2 at age 25
- Relatively rare in infants; also less common after middle age
Aetiology
- No single unifying hypothesis; mixed aerobic and anaerobic bacterial proliferation
- Luminal obstruction is the main initiating event - by:
- Faecolith (appendicolith) - most common
- Lymphoid hyperplasia (especially in young adults after viral/GI infection)
- Stricture, foreign body, rarely tumour
- Low dietary fibre / high refined carbohydrate diet is associated
Pathological Sequence
- Obstruction → increased intraluminal pressure → mucosal ulceration
- Bacterial invasion of wall → acute appendicitis (congestion, oedema, polymorphonuclear infiltrate)
- Venous and lymphatic obstruction → ischaemia → gangrenous appendicitis
- Full-thickness necrosis → perforation → local or generalised peritonitis
Risk Factors for Perforation
- Extremes of age (very young, elderly)
- Retrocaecal position (delayed diagnosis - "silent appendix")
- Faecolith obstruction
- Delay in presentation / diagnosis
Symptoms
- Central / periumbilical colicky pain - initial (visceral, T10 referred)
- Migration to RIF - somatic as parietal peritoneum is involved (hours later)
- Anorexia (almost invariable)
- Nausea and vomiting (after pain onset - contrast with gastroenteritis where vomiting precedes pain)
- Low-grade fever
Clinical Signs
- McBurney's point tenderness - point of maximum tenderness located 1/3 of the way along a line from ASIS to umbilicus
- Guarding and rigidity in RIF
- Rebound tenderness (Blumberg's sign) - peritoneal irritation
- Rovsing's sign - palpation of the left iliac fossa causes pain in the RIF (indicates peritoneal irritation)
- Psoas sign - pain on hyperextension of right hip (retrocaecal appendix on psoas)
- Obturator sign (Zachary Cope) - pain in hypogastrium when right hip is flexed and internally rotated (pelvic appendix)
- Low-grade fever (37.2-37.7°C typically); higher suggests perforation
- Pointing sign - patient locates maximal tenderness with one finger
Summary: Signs to Elicit
- Pointing sign
- Rovsing's sign
- Psoas sign
- Obturator sign
Position-Specific Features
| Position | Features |
|---|---|
| Retrocaecal | Rigidity often absent ("silent appendix" - gas-filled caecum prevents pressure reaching it); deep loin tenderness; psoas spasm; hip flexion |
| Pelvic | No abdominal rigidity, no RIF tenderness; rectal tenderness on right side in rectovesical pouch / pouch of Douglas; frequency of micturition (bladder contact); early diarrhoea (rectal contact) |
| Pre-ileal / post-ileal | May cause diarrhoea, early vomiting |
CONDITIONS: ACUTE AND CHRONIC
Acute Appendicitis
Simple, complicated (perforated), gangrenous - as above.
Appendix Mass (Phlegmon)
Develops when the perforated appendix is walled off by adherent omentum and loops of bowel (usually 3-5 days after symptom onset). Presents as a palpable, tender mass in the RIF.
Management - Ochsner-Sherren Conservative Regime:
- Based on premise that inflammation is already localised; surgery is difficult and dangerous
- IV antibiotics, fluid balance monitoring, 4-hourly pulse and temperature
- Mark limits of mass with skin pencil; contrast-enhanced CT
- Radiological drainage if abscess present
- Approximately 90% resolve without surgery
Criteria to STOP conservative treatment (operate):
- Rising pulse rate
- Increasing or spreading abdominal pain
- Increasing size of the mass
Interval appendicectomy: debated; at least follow-up CT/MRI and colonoscopy. In patients over 40, up to 29% may have underlying appendiceal neoplasm (particularly LAMNs); interval appendicectomy recommended.
Appendix Abscess
A walled-off collection of pus around the appendix. Can be drained radiologically (percutaneously under CT or USS guidance).
Recurrent / Chronic Appendicitis
- Rare; characterised by recurrent episodes of lower abdominal pain
- Arises from incomplete, self-limiting obstruction of the appendix lumen
- Attacks every few months; majority ultimately culminate in severe acute appendicitis
- Appendix is thickened with fibrosis from previous inflammation
- Many patients with acute appendicitis recall prior milder similar episodes
Appendicitis in Pregnancy
- Incidence: 0.5-1 per 1000 pregnancies; slightly more common in second trimester
- More likely to be complicated (perforated) when compared with non-pregnant
- Diagnosis difficult: early symptoms attributed to pregnancy; right lower quadrant pain remains the most common presentation (the classical upward displacement of the appendix is less dramatic than once thought)
- Requires surgical treatment regardless of trimester; laparoscopy is appropriate in first and second trimesters
Appendicitis in Special Groups
- Children: higher perforation rate; mesenteric adenitis and gastroenteritis are common differentials
- Elderly: higher perforation and complication rates; diagnose diverticulitis, malignancy
- Immunocompromised: atypical presentation, higher complication rates
DIFFERENTIAL DIAGNOSIS (Table 76.1)
| Children | Adults | Adult Female | Elderly |
|---|---|---|---|
| Gastroenteritis | Regional enteritis (Crohn's) | Mittelschmerz | Diverticulitis |
| Mesenteric adenitis | Ureteric colic | Pelvic inflammatory disease | Intestinal obstruction |
| Meckel's diverticulitis | Perforated peptic ulcer | Pyelonephritis | Caecal carcinoma |
| Intussusception | - | Ectopic pregnancy | - |
INVESTIGATIONS
Preoperative Investigations (Summary Box 76.5)
Routine:
- Full blood count (leukocytosis with neutrophilia - WCC usually 11,000-17,000)
- Urinalysis (exclude UTI; note: a few RBCs/WBCs may be present with retrocaecal appendicitis)
Selective:
- Pregnancy test (all females of reproductive age)
- Urea and electrolytes
- C-reactive protein (CRP) - raised; a normal CRP AND normal WCC makes appendicitis unlikely
- Supine abdominal radiograph - limited value but may show faecolith, loss of psoas shadow, sentinel loop
- Ultrasound abdomen/pelvis - useful, especially in children and women; non-compressible appendix >6 mm diameter; sensitivity ~75-85%
- Contrast-enhanced CT abdomen/pelvis - gold standard for diagnosis; use low-dose protocol in young adults; sensitivity ~94-98%; also excludes other pathology
Alvarado (MANTRELS) Score - Table 76.2
| Feature | Score |
|---|---|
| Migratory RIF pain | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| Tenderness in RIF | 2 |
| Rebound tenderness | 1 |
| Elevated temperature | 1 |
| Leukocytosis | 2 |
| Shift to left (neutrophilia) | 1 |
| Total | 10 |
Score interpretation: ≤4 = unlikely; 5-6 = possible; 7-8 = probable; 9-10 = very likely. Score ≥7 generally warrants surgery or further imaging.
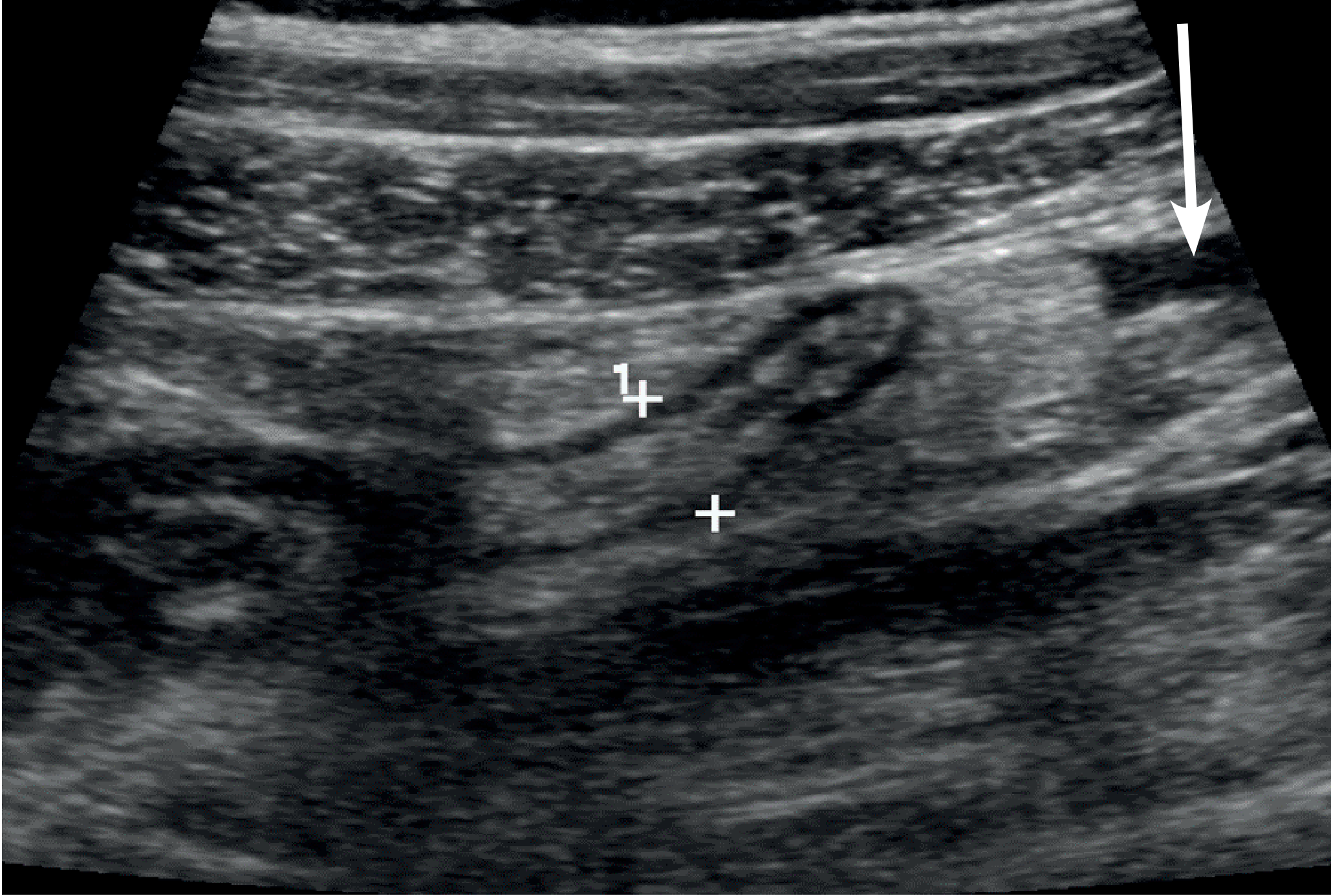
Figure 76.8 - USS showing mildly enlarged appendix (8 mm), consistent with acute appendicitis (Bailey & Love)
PREOPERATIVE MANAGEMENT
- IV access, IV fluids (correct dehydration)
- IV antibiotics (prophylactic or therapeutic depending on severity) - typically metronidazole + a cephalosporin/co-amoxiclav
- DVT prophylaxis assessment
- Bladder must be empty before laparoscopic approach (ensure patient has voided)
- Palpate RIF for mass before draping - if mass is palpable, consider conservative approach
- Consent: laparoscopic or open; possibility of conversion; stoma (very rare)
- Mark the abdomen to plan incision
SURGICAL TECHNIQUE AND INCISIONS
Open / Conventional Appendicectomy
1. Gridiron Incision (McArthur)
- Made at right angles to a line joining the ASIS to the umbilicus
- Centred at McBurney's point (junction of lateral 1/3 and medial 2/3 of this line)
- Muscles split in direction of their fibres (external oblique, internal oblique, transversus abdominis)
- Can be extended to Rutherford Morison incision by cutting the internal oblique and transversus in the line of the incision (not in the direction of their fibres) - useful for retrocaecal appendix or when wider access is needed
2. Lanz Incision (Transverse / Skin Crease)
- Now more popular: better cosmesis, better healing, easier extension
- Made approximately 2 cm below the umbilicus, centred on the midclavicular-midinguinal line
- Can be extended medially with retraction or division of rectus abdominis
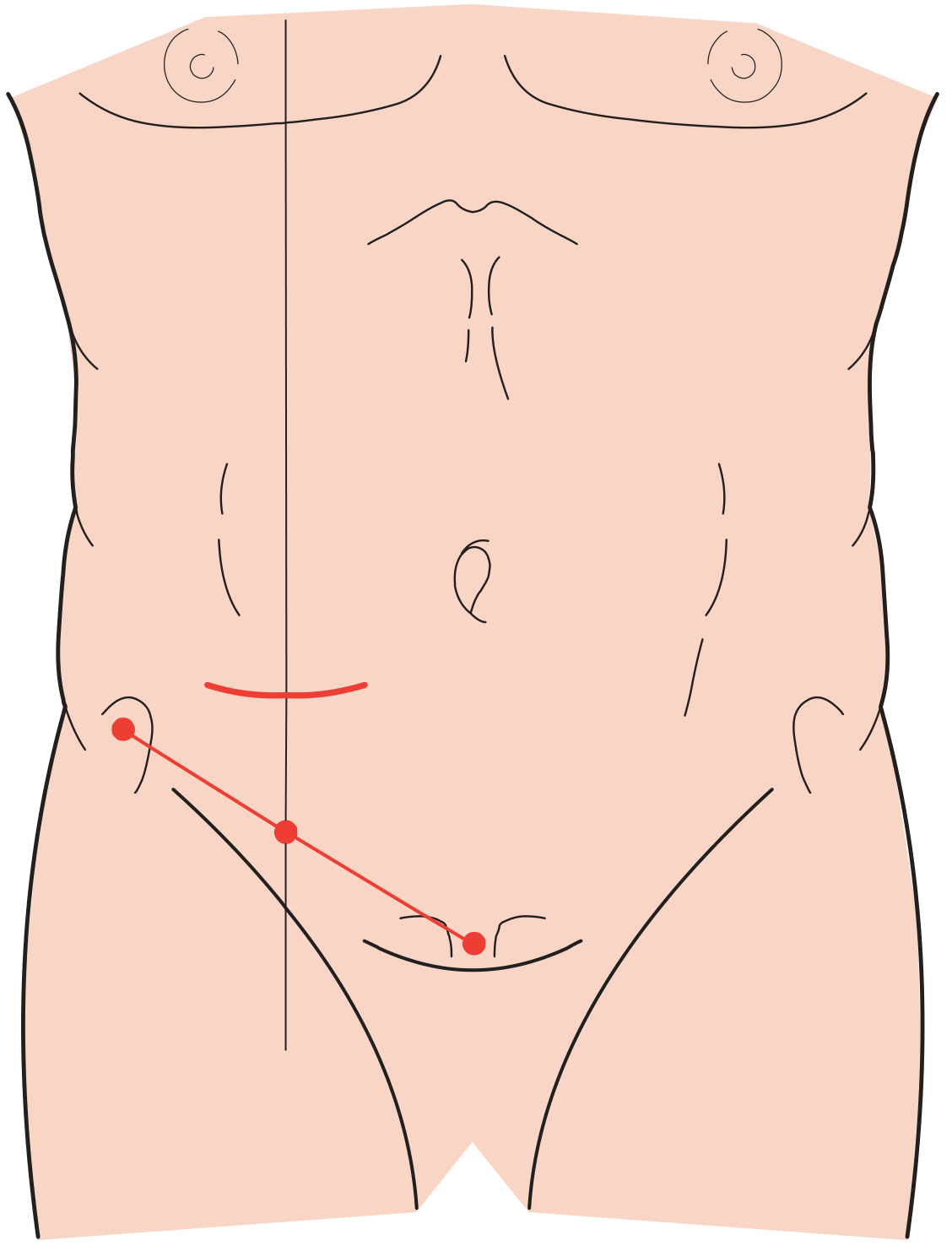
Figure 76.11 - Lanz (transverse skin crease) incision for appendicectomy (Bailey & Love)
3. Lower Midline Incision
- When diagnosis is in doubt, especially if intestinal obstruction is suspected
- Preferred over right lower paramedian (which is difficult to extend, close, and provides poor pelvic access)
4. Rutherford Morison Incision
- Useful when appendix is difficult to locate (e.g. retrocaecal)
Operative Steps (Open)
- Enter peritoneum; identify caecum (follow the anterior taenia coli to the base of the appendix)
- Divide and ligate the mesoappendix including appendicular artery
- Crush the base of the appendix with a haemostat; religate; transect
- Stump burial with a purse-string or Z-stitch into caecal wall (invagination of the stump)
- Irrigate if peritoneal contamination; close in layers
Laparoscopic Appendicectomy
- Bladder must be empty
- Three-port technique standard; umbilical camera port
- Mesoappendix divided using diathermy/stapler/clips; appendix base stapled or ligated with endoloops
- Superior for diagnosis in women of reproductive age (can inspect ovaries/tubes)
- Lower wound infection rate; earlier return to normal activities
- Slightly higher risk of intra-abdominal abscess post-op compared to open
Problems Encountered at Operation
- Normal appendix found: exclude terminal ileitis (Crohn's), Meckel's diverticulitis, gynaecological causes; remove appendix anyway if gridiron/Lanz incision used to avoid future diagnostic confusion (~1/4 of macroscopically normal appendices show microscopic inflammation)
- Cannot find appendix: mobilise caecum, trace taeniae coli to their confluence - the base of the appendix is always at this point
- Appendix mass at operation: may be safer to abandon (especially laparoscopically) - drain any abscess, give IV antibiotics, monitor
- Crohn's disease found: if caecal wall is healthy at base, appendicectomy is safe; if appendix itself involved, conservative management with corticosteroids/antibiotics
- Frankly necrotic appendix / extensive caecal necrosis: may require caecectomy or partial right hemicolectomy
POSTOPERATIVE COMPLICATIONS
Early
| Complication | Notes |
|---|---|
| Wound infection | Most common early complication; usually 5th-7th postoperative day; organisms - Gram-negative bacilli, Bacteroides, anaerobic streptococci; treatment: wound drainage + antibiotics |
| Intra-abdominal abscess | ~8% post appendicectomy; sites - pelvic, paracolic, subphrenic, interloop; presents with spiking fever, malaise, anorexia 5-7 days post-op (often after discharge); CT/USS for diagnosis; percutaneous drainage preferred |
| Ileus | Expected after gangrenous appendicitis; persistent ileus >4-5 days + fever = ongoing intra-abdominal sepsis; CT scan required. Early Richter's hernia at port site can mimic ileus |
| Portal pyaemia (pylephlebitis) | Rare but serious; gangrenous appendicitis → portal venous septicaemia → multiple intrahepatic abscesses; presents with high fever, rigors, jaundice; treat with systemic antibiotics and percutaneous hepatic drainage |
| Faecal fistula | Rare; leakage from appendicular stump - if encircling stitch placed too deeply or if caecal wall was oedematous/inflamed; also in Crohn's disease |
Late
| Complication | Notes |
|---|---|
| Adhesive intestinal obstruction | Most common late complication of appendicectomy; usually a single band adhesion at laparotomy |
| Chronic pain (adhesions) | Chronic RIF pain post-appendicectomy; laparoscopy confirms and treats adhesions |
| Venous thromboembolism | Rare; assess preoperatively and apply appropriate prophylaxis |
| Respiratory | Rare in absence of pre-existing lung disease; adequate analgesia + physiotherapy |
NEOPLASMS OF THE APPENDIX (Brief)
- Incidence up to 0.97 per 100,000
- NETs (neuroendocrine tumours, formerly carcinoids): ~30% of appendix neoplasms; arise from Kulchitsky (argentaffin) cells; most are benign if <2 cm; found incidentally at appendicectomy
- <2 cm: simple appendicectomy is curative
-
2 cm: right hemicolectomy
- Epithelial tumours (mucinous or non-mucinous): range from low-grade appendiceal mucinous neoplasm (LAMN) to invasive adenocarcinoma with signet-ring features; may cause pseudomyxoma peritonei (jelly-belly)
- Mesenchymal: lymphoma, GIST, Kaposi's sarcoma, granular cell tumour
Unexpected tumour at surgery: if tumour found in a patient undergoing appendicectomy, assessment of tumour size and histology guides further management (right hemicolectomy vs. observation).
SUMMARY TABLE
| Topic | Key Bailey & Love Points |
|---|---|
| Embryology | Midgut-derived; caecal bud; appendix at apex; posteromedial shift with growth |
| Artery | Branch of lower division ileocolic artery; end-artery; thrombosis = gangrene |
| Vein | Ileocolic → superior mesenteric → portal |
| Lymphatics | 4-6+ channels → ileocaecal nodes; submucosal follicles prominent in young |
| Nerve | Sympathetic T10 (central pain); parietal peritoneum → somatic (RIF pain) |
| Acute appendicitis | Luminal obstruction → bacterial proliferation → necrosis → perforation |
| Investigations | FBC, CRP, USS, CT; Alvarado score |
| Incisions | Gridiron (McArthur), Lanz (Lanz), Midline, Rutherford Morison |
| Post-op complications | Wound infection, intra-abdominal abscess, ileus, portal pyaemia, faecal fistula, adhesion obstruction |
- Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 76: The Vermiform Appendix
This is a shared conversation. Sign in to Orris to start your own chat.