Gastritis
Reading File
Finding Sources
Searching PubMed
"gastritis"[MeSH Terms] AND ("Helicobacter pylori"[MeSH Terms] OR "autoimmune gastritis"[MeSH Terms])
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive data. Let me compile the full answer:
Gastritis
Gastritis is defined as histologically documented inflammation of the gastric mucosa. It is not synonymous with endoscopic erythema or with "dyspepsia." The correlation between histologic findings, symptoms, and endoscopic appearance is poor, so there is no single "typical" clinical picture. - Harrison's Principles of Internal Medicine 22E, p. 2581
Classification
Gastritis is classified by time course, histologic features, anatomic distribution, and proposed pathogenic mechanism:
I. Acute Gastritis
- Acute H. pylori infection
- Other infectious: bacterial (phlegmonous), H. heilmannii, mycobacterial, syphilitic, viral (HSV, CMV), parasitic, fungal
II. Chronic Atrophic Gastritis
- Type A (autoimmune, body-predominant)
- Type B (H. pylori-related, antral-predominant)
- Indeterminate (mixed/pangastritis)
III. Uncommon Forms
- Lymphocytic (varioliform), eosinophilic, Crohn's-related, sarcoidosis, isolated granulomatous, Russell body gastritis, immune checkpoint inhibitor-induced
Topographic Patterns
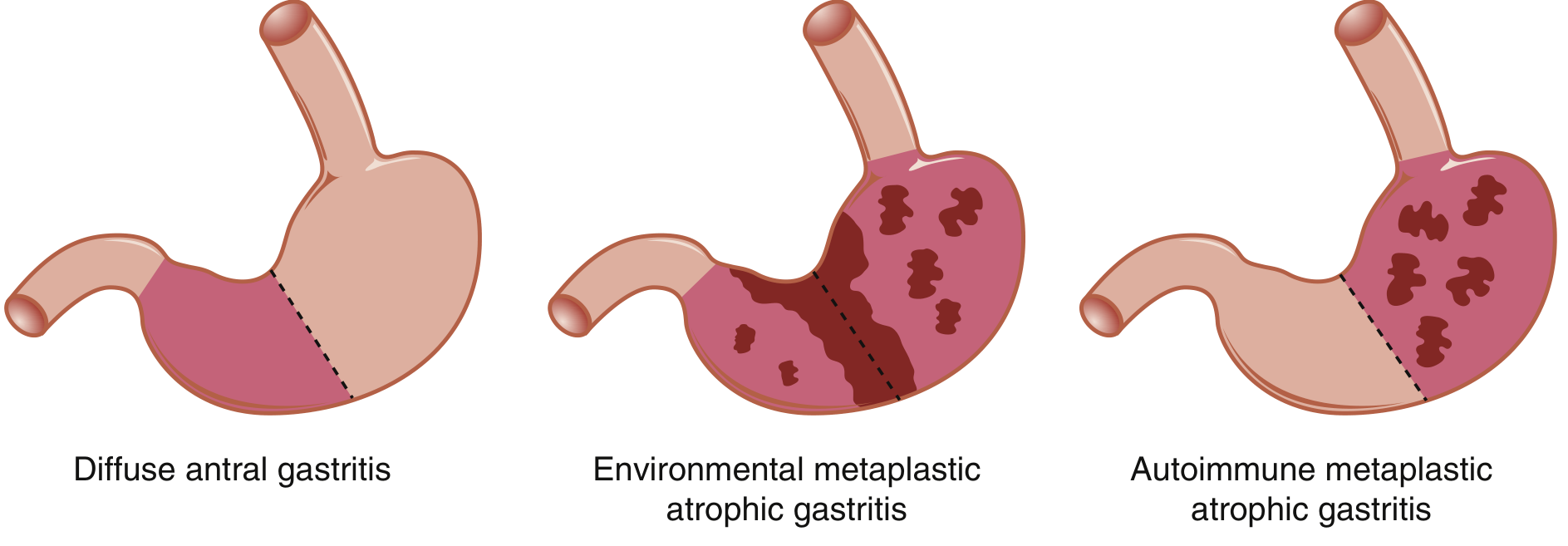
Diffuse antral gastritis (H. pylori), Environmental metaplastic atrophic gastritis, and Autoimmune metaplastic atrophic gastritis - Sleisenger & Fordtran's, Fig. 52.2
Etiology & Pathogenesis
H. pylori Gastritis (Most Common)
- H. pylori is a gram-negative, helical/spiral-shaped, flagellated bacterium - the most common chronic bacterial infection in humans
- Over 50% of the world's population is infected (70-80% in developing nations)
- Key risk factor: low socioeconomic status in childhood; infection commonly acquired before age 10 in developing countries
- Infection triggers a persistent acute inflammatory infiltrate (neutrophils, lymphocytes, plasma cells, macrophages); despite robust host immune response, bacteria persist in most infected individuals
- Typically affects the antrum (diffuse antral gastritis), associated with increased gastric acid production
- Over time, the body/corpus can become involved (pangastritis), leading to glandular atrophy and mildly reduced acid secretion
- Host immune responses and bacterial virulence factors (e.g., CagA, VacA) determine whether infection stays antral or progresses to pangastritis and atrophy
- Induces MALT (mucosa-associated lymphoid tissue) that can give rise to B-cell MALTomas (lymphoma)
Autoimmune Gastritis (Type A)
- After H. pylori and NSAIDs, this is the third most common cause of chronic gastritis
- Involves primarily the fundus and body (oxyntic glands), with antral sparing
- Results in: glandular atrophy, decreased acid production, antral G-cell hyperplasia (due to loss of acid feedback), and vitamin B12 deficiency (due to loss of intrinsic factor)
- Anti-parietal cell antibodies directed against H+,K+-ATPase are present in >90% of pernicious anemia patients and ~50% of Type A gastritis patients
- Anti-intrinsic factor antibodies are more specific for Type A gastritis
- Strong autoimmune association: ~50% of pernicious anemia patients have thyroid antibodies; ~30% of thyroid disease patients have anti-parietal cell antibodies; also linked to vitiligo and Addison's disease
- Molecular mimicry between H. pylori LPS and H+,K+-ATPase is proposed as a possible trigger in some cases
NSAIDs and Alcohol
- Interfere with gastric mucosal protective mechanisms (prostaglandin synthesis, mucous layer, bicarbonate secretion)
- Cause acute mucosal injury; NSAIDs are a leading cause of chronic gastric damage with long-term use
Histologic Progression of Chronic Gastritis
- Superficial gastritis - inflammatory infiltrate limited to lamina propria of surface mucosa; edema separates intact glands
- Atrophic gastritis - infiltrate extends deeper, with progressive distortion and destruction of glands
- Gastric atrophy - glandular structures are lost; paucity of inflammatory infiltrates; thinned mucosa with visible submucosal vessels on endoscopy
- Intestinal metaplasia - gastric glands convert to small intestinal phenotype with goblet cells; a significant precancerous lesion (risk factor for gastric adenocarcinoma)
Acute Gastritis - Special Forms
Phlegmonous (Suppurative) Gastritis
- Infection of the submucosa and muscularis propria, often sparing the mucosa
- Causative organisms: gram-negative bacilli, anaerobes, gram-positive cocci (Group A streptococci), fungi (mucormycosis)
- Risk factors: alcoholism, immunocompromised states (AIDS, liver transplant), recent surgery, respiratory tract infection
- Presentation: septic appearance, acute upper abdominal pain, peritonitis, purulent ascites, fever, hypotension
Emphysematous Gastritis
- Severe form caused by gas-producing organisms: Clostridium perfringens, E. coli, S. aureus
- CT/plain films show gas in the gastric wall and portal venous system
- Can progress to gastric gangrene; potentially fatal
- Treatment: broad-spectrum antibiotics; may require gastrectomy if antibiotics fail
Complications
| Complication | Mechanism |
|---|---|
| Peptic ulcer disease | H. pylori-induced gastritis + hyperchlorhydria → duodenal/gastric ulcers |
| Gastric adenocarcinoma | Intestinal metaplasia from chronic atrophic gastritis |
| MALT lymphoma (MALToma) | H. pylori-induced mucosal lymphoid tissue proliferation |
| Pernicious anemia | Autoimmune destruction of parietal cells → intrinsic factor loss → B12 deficiency |
| Ménétrier disease | Excessive TGF-α secretion → diffuse foveolar hyperplasia → protein-losing enteropathy |
| Zollinger-Ellison syndrome | Gastrin-secreting tumor → parietal cell hyperplasia, acid hypersecretion; 60-90% of gastrinomas are malignant |
Uncommon Forms
- Lymphocytic (varioliform) gastritis - intense T-cell infiltration of surface epithelium; associated with celiac sprue; endoscopically shows thickened folds with central erosions; steroids/sodium cromoglycate with unclear results
- Eosinophilic gastritis - eosinophilic infiltration of any gastric layer; often with peripheral eosinophilia and systemic allergy; antrum predominantly involved, can cause outlet obstruction; treatment is glucocorticoids
- Granulomatous gastritis - seen in Crohn's disease, sarcoidosis, histoplasmosis, candidiasis, syphilis, TB; may require full-thickness surgical biopsy to exclude malignancy
- Russell body gastritis - mucosal lesion with pseudotumoral appearance; plasma cells with Russell bodies; strongly associated with H. pylori; resolves with H. pylori eradication
- Immune checkpoint inhibitor-induced gastritis - recognized complication of cancer immunotherapy; requires glucocorticoids and potentially IL-6 receptor blockers
Diagnosis
- Histology (endoscopic biopsy) is the gold standard - gastritis cannot be diagnosed from endoscopy alone
- H. pylori testing: urea breath test, stool antigen (non-invasive, preferred for confirmation of eradication); rapid urease test and histology on biopsy (invasive)
- Serology: anti-parietal cell and anti-intrinsic factor antibodies for autoimmune gastritis
- Serum markers: Pepsinogen I/II ratio, gastrin-17, and anti-H. pylori serology are used as non-invasive markers of gastric atrophy severity
- Imaging (CT): useful for emphysematous/phlegmonous gastritis (showing gas in gastric wall and portal venous system)
Treatment
H. pylori Eradication
Target eradication rate: 85-90% for first-line therapy
No single agent is effective; combination therapy for 14 days is most effective.
| Regimen | Drugs | Notes |
|---|---|---|
| Clarithromycin triple therapy | PPI (bid) + amoxicillin + clarithromycin | Only if no prior macrolide exposure and local resistance <15% |
| Bismuth quadruple | Bismuth + metronidazole + tetracycline + PPI | Preferred in areas of high clarithromycin resistance |
| Concomitant (non-bismuth quadruple) | PPI + amoxicillin + clarithromycin + metronidazole | Alternative first-line |
| Levofloxacin triple | PPI + amoxicillin + levofloxacin | Salvage therapy |
Key considerations:
- Rising clarithromycin and metronidazole resistance is significantly impacting eradication success
- Antibiotic susceptibility testing/culture-guided therapy is increasingly recommended
- H. pylori eradication before long-term NSAID use reduces risk of GI bleeding
- Eradication is recommended in: PUD, MALT lymphoma, early gastric cancer resection, unexplained iron-deficiency anemia, immune thrombocytopenic purpura, first-degree relatives of gastric cancer patients, patients with severe atrophic gastritis
Autoimmune/Chronic Gastritis
- Treatment is aimed at sequelae, not the underlying inflammation
- Pernicious anemia requires parenteral vitamin B12 supplementation (long-term)
- Endoscopic surveillance is recommended in atrophic gastritis (risk of adenocarcinoma)
Eosinophilic/Lymphocytic Gastritis
- Glucocorticoids are the primary treatment for eosinophilic gastritis (usually effective)
- Lymphocytic gastritis: H. pylori eradication if positive; glucocorticoids/sodium cromoglycate for others
Recent Evidence (2024-2026)
A 2026 Asian Pacific Association of Gastroenterology task force guideline (PMID 41057234, published in Gut) provides updated recommendations on surveillance for H. pylori-associated gastric premalignant conditions. A 2025 meta-analysis (PMID 39920638) found folic acid supplementation beneficial in chronic atrophic gastritis with H. pylori infection. A 2025 systematic review (PMID 40822578) examined H. pylori-gut microbiome interactions and their clinical outcomes.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 720 | Harrison's Principles of Internal Medicine 22E, p. 2581 | Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 52
This is a shared conversation. Sign in to Orris to start your own chat.