Morel lavelle lesion
Reading File
Finding Sources
Searching PubMed
"Morel-Lavallee" lesion
Searching the Web
Morel-Lavallee lesion pathophysiology diagnosis management 2024
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Morel-Lavallée Lesion
Definition and History
A Morel-Lavallée lesion (MLL) is a closed internal degloving injury first described by French surgeon Victor Auguste François Morel-Lavallée in 1863. It results from shearing forces that separate the skin and subcutaneous tissue from the underlying deep fascia, creating a potential space that fills with blood, lymph, necrotic fat, and debris.
Pathophysiology
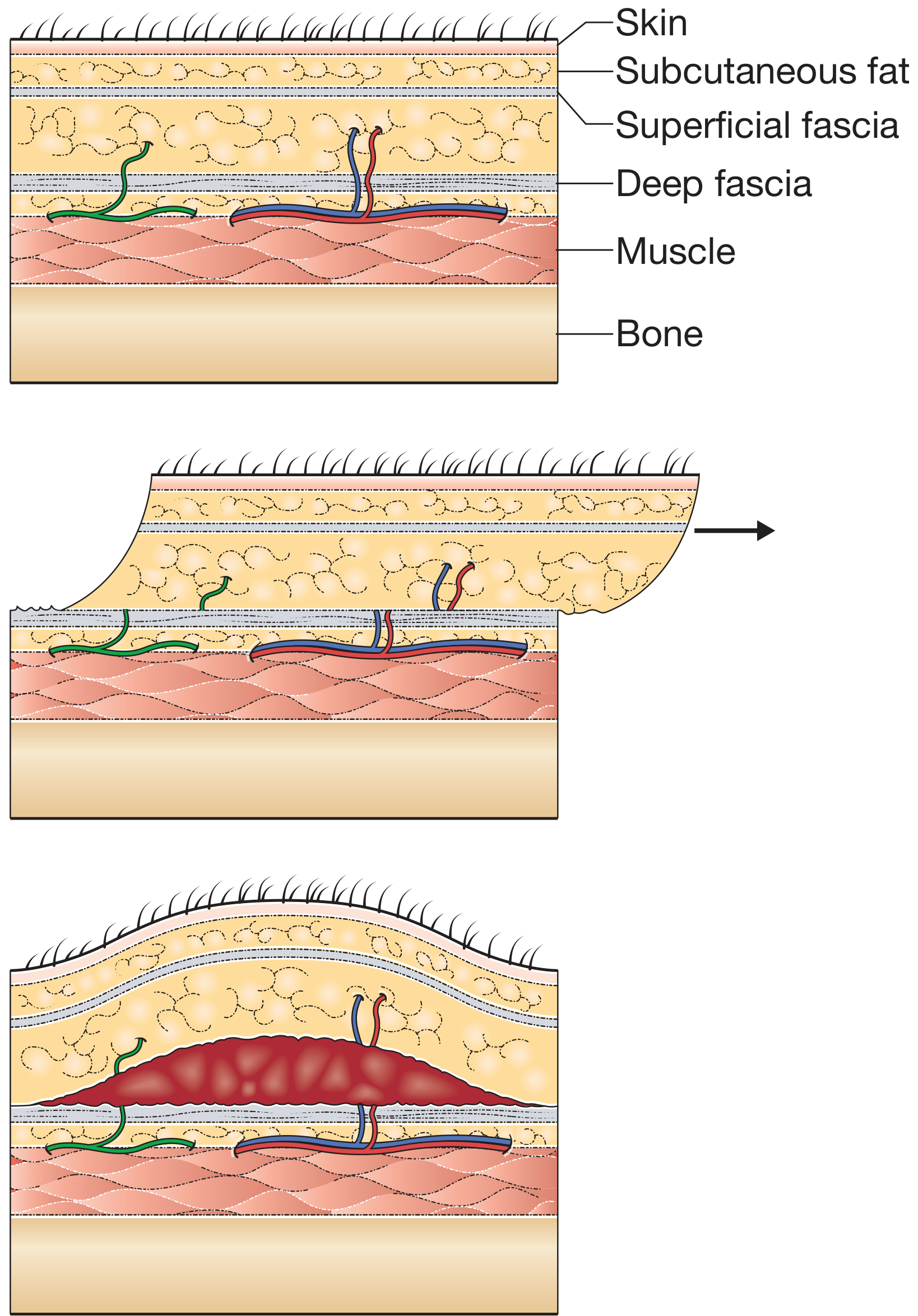
Figure: The shearing force displaces the mobile subcutaneous fat relative to the fixed deep fascia, tearing perforating arteries (red), veins (blue), and lymphatics (green), creating a haemolymphatic collection in the potential space between the superficial and deep fascial layers.
The injury occurs in regions where overlying skin is mobile and the underlying fascia is tough - classically the quadriceps fascia (superior to knee) and fascia lata (proximal lateral thigh). The shearing disrupts:
- Lymphatic vessels
- Locules of subdermal fat
- Transaponeurotic capillaries
The resulting cavity fills with a mix of haemolymphatic fluid and necrotic fat. With time, a fibrous pseudocapsule may form. Importantly, up to 46% of "closed" lesions are culture-positive at initial debridement, making infection a major concern.
- Campbell's Operative Orthopaedics 15th Ed 2026, Ch. 58
- Bailey and Love's Short Practice of Surgery 28th Ed
Common Locations
- Peritrochanteric / lateral hip and proximal thigh (most common)
- Greater trochanter region
- Buttock
- Knee and distal thigh
- Lumbar region
- Less common: chest wall, breast, scalp
Approximately 8% of patients sustaining a blow to the greater trochanter have a clinically significant MLL.
Associated Injuries
MLL is frequently missed because it coexists with distracting bony injuries:
- Pelvic fractures
- Acetabular fractures
- Proximal femur fractures
- High-energy extremity trauma
It is especially common in obese individuals where the shear component of injury is amplified.
Clinical Presentation

Figure: A and B - Large Morel-Lavallée lesion in the thigh after pelvic fracture. Note the extensive ecchymosis and soft-tissue swelling.
Signs and symptoms:
- Soft tissue swelling and ecchymosis over affected area
- Fluctuance and compressibility of the swelling (fluid wave)
- Hypermobility of overlying skin - a key diagnostic clue
- Pain (may be disproportionately mild given lesion size)
- Late presentations may include full-thickness skin necrosis
Imaging
MRI (modality of choice)
Signal characteristics evolve with lesion age:
| Phase | T1 | T2 |
|---|---|---|
| Acute (<1 week) | Hypointense | Hyperintense |
| Subacute (1-6 weeks) | Increasingly hyperintense | Hyperintense |
| Chronic (>6 weeks) | Heterogeneous (haemosiderin deposit) | Heterogeneous |
On MRI, the lesion appears as an elliptical/lobular mass in the deep subcutaneous fat, with:
- Low-signal rim (chronic haemorrhage / fibrous capsule)
- Heterogeneous internal contents (blood, fat, debris)
- Possible rim enhancement
- Fat-fluid levels
CT
- Useful when MRI is unavailable; shows a hypodense fluid collection in subcutaneous tissue
- The CT should be scrutinized in pelvic/acetabular fracture patients for any subcutaneous fluid collection
Ultrasound
- Subcutaneous hypo-/anechoic collection
- Point-of-care ultrasound (POCUS) is gaining traction for bedside diagnosis and drainage guidance
Grainger & Allison's Diagnostic Radiology; Pathologyoutlines.com
Differential Diagnosis
- Post-operative seroma
- Coagulopathy-related haematoma
- Post-traumatic fat necrosis
- Early myositis ossificans (with diffuse subcutaneous oedema)
- Abscess
Why It Matters Clinically: Surgical Site Infection
The presence of an MLL overlying a planned operative approach significantly increases postoperative infection risk:
- Infection rate reported as high as 12% with repeated debridement and secondary intention healing
- Culture positivity in 46% of closed lesions at initial debridement
- Lesions >50 mL are particularly high-risk (83% infection vs. 33% for <50 mL)
When planning acetabular/pelvic ORIF, the MLL should be treated before or at the time of fixation. Sometimes the anterior approach is chosen to avoid the affected lateral area.
- Campbell's Operative Orthopaedics 15th Ed 2026, Ch. 60 (Acetabulum)
Management
There is no universally accepted treatment algorithm. Management is individualized based on lesion size, chronicity, location, and planned surgery.
Conservative / Non-operative
- Compression bandaging: for small, acute lesions
- Observation: associated with relatively low infection rates (~19%)
- Best outcomes when managed acutely
Percutaneous Aspiration
- Suitable for small, acute lesions
- High recurrence rate
- Higher infection rate (~56%) compared to observation or excision - thus often insufficient alone
Percutaneous Drainage (Tseng & Tornetta Technique)
Recommended within 3 days of injury for good results:
- 2-cm incision over the distal aspect of the lesion
- Second 2-cm incision at the superior/posterior extent
- Determine lesion extent with suction tip; add incisions as needed
- Send fluid for culture & sensitivity
- Drain haematoma with suction
- Debride loose fat with plastic brush
- Pulsed lavage until fluid is clear
- Place closed suction drain (to wall suction until output <30 mL/24h - may take ~8 days)
- Close incisions tightly
- IV cephalosporin (or culture-directed) for 24h post-drain removal
Open Surgical Debridement
- Indicated for large lesions, chronic/infected lesions, or those overlying planned ORIF sites
- Debride to a bleeding edge; do NOT use tourniquet (skin viability cannot be assessed)
- Complications: massive wounds, risk of devascularizing overlying skin
Sclerotherapy
- Doxycycline or talc injected into the cavity to obliterate the space
- Used increasingly as a minimally invasive alternative
- Useful for chronic or recurrent lesions
Key decision threshold (Rockwood & Green 2025):
Collections >50 mL are best treated surgically rather than with aspiration alone.
- Campbell's Operative Orthopaedics 15th Ed 2026, Technique 58.1
- Rockwood and Green's Fractures in Adults 10th Ed 2025, Table 16-13
Key Clinical Pearls
- Frequently missed - always consider in pelvic/acetabular fracture patients, especially obese individuals
- Hypermobility of skin or a palpable fluid wave should raise suspicion
- Check CT for subcutaneous fluid in all high-energy pelvic trauma patients
- Treat before ORIF or choose an approach that avoids the lesion
- Percutaneous drainage with drain output <30 mL/day before ORIF is a validated strategy
- Delayed or misdiagnosed lesions have higher infection and skin necrosis risk
This is a shared conversation. Sign in to Orris to start your own chat.