Superior mesenteric artery detailed explanation and anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information and excellent anatomy diagrams. Let me compile the full detailed answer.
Superior Mesenteric Artery (SMA) - Detailed Anatomy
Overview
The superior mesenteric artery is the second unpaired anterior branch of the abdominal aorta and the principal blood supply to the midgut - embryologically, this includes everything from the lower duodenum to the proximal two-thirds of the transverse colon.
- Gray's Anatomy for Students
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Origin and Vertebral Level
The SMA arises from the anterior surface of the abdominal aorta at the level of vertebra L1 (lower part), immediately below the celiac trunk. It originates posterior to the neck of the pancreas and the splenic vein.
Relations (Anatomical Relationships)
Understanding what surrounds the SMA is clinically important:
| Direction | Structures |
|---|---|
| Anterior | Splenic vein, neck of the pancreas |
| Posterior | Left renal vein, uncinate process of the pancreas, inferior part of the duodenum (3rd part) |
| Right | Superior mesenteric vein (runs alongside) |
The SMA and superior mesenteric vein (SMV) together form a "vascular pedicle" that crosses anterior to the 3rd part of the duodenum - this relationship is the anatomical basis of SMA syndrome (compression of the duodenum).
Fig. 4.127 - Initial Branching and Relationships
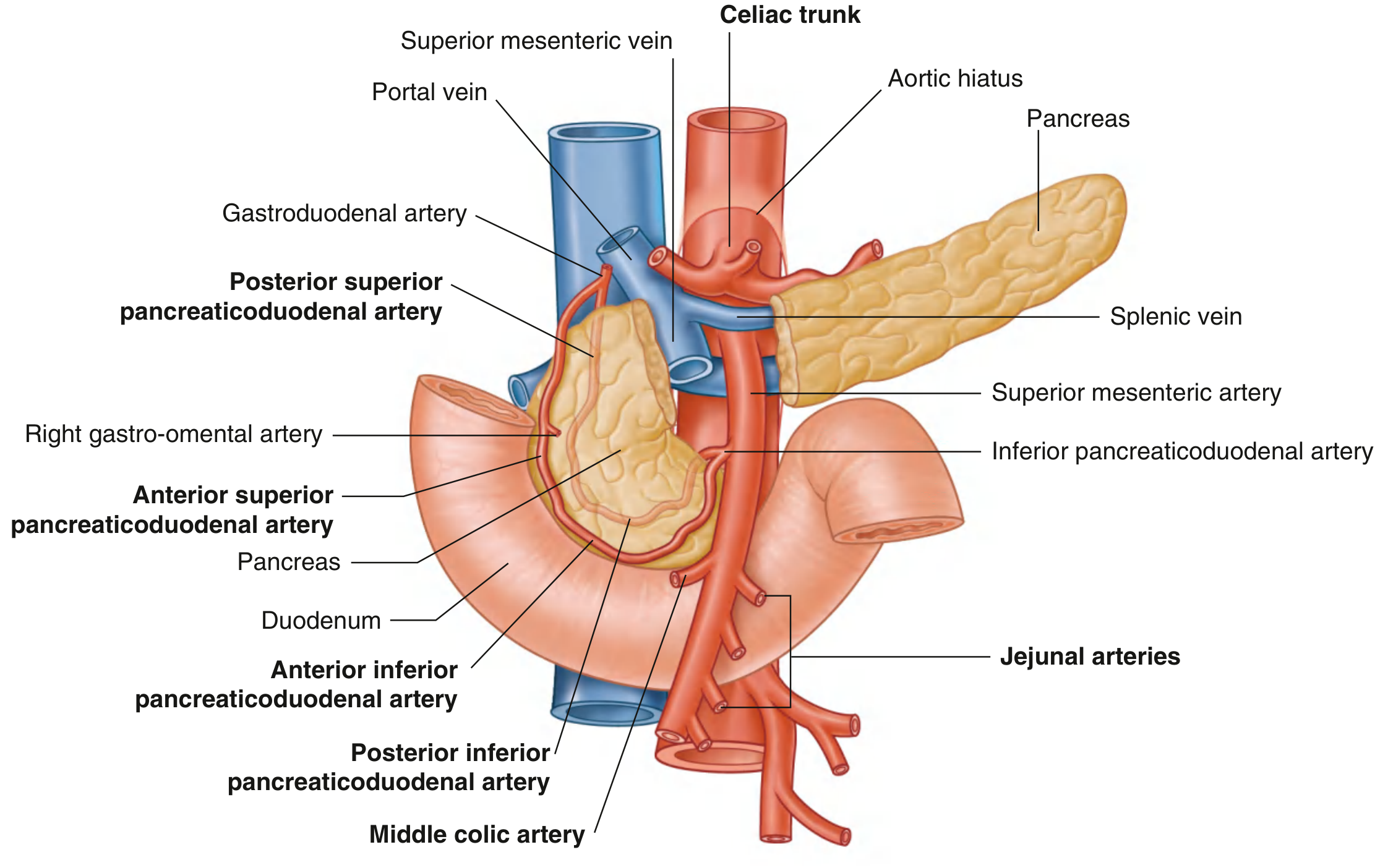
Initial branching of the SMA showing its relationship to the celiac trunk, pancreas, splenic vein, portal vein, and the pancreaticoduodenal anastomotic network.
Branches of the SMA
The SMA gives off 5 major named branches, plus a series of intestinal branches:
1. Inferior Pancreaticoduodenal Artery (IPDA) - First Branch
- The very first branch of the SMA
- Immediately divides into anterior and posterior branches, which ascend on the corresponding sides of the head of the pancreas
- Anastomoses with the anterior and posterior superior pancreaticoduodenal arteries (branches of the gastroduodenal artery from the celiac trunk)
- This anastomosis is the major collateral pathway between the celiac trunk and the SMA
- Supplies: head and uncinate process of the pancreas + the duodenum
2. Jejunal and Ileal Arteries (Left-side branches)
- Arise from the left side of the main SMA trunk, distal to the IPDA
- Usually 15-18 in number (highly variable)
- Pass between the two layers of the mesentery
- Form anastomosing arches (arterial arcades) - the number of arcade tiers increases distally:
- Jejunum: 1-2 tiers of arcades; longer, closely spaced vasa recta forming narrow windows
- Ileum: up to 4-5 tiers of arcades; shorter, widely spaced vasa recta forming broader windows
- From the terminal arcade, vasa recta (straight arteries) arise to enter the intestinal wall directly - these have very limited collateral potential, making terminal ileum and jejunum susceptible to focal ischemia if cut
3. Middle Colic Artery (First right-side branch)
- Arises as the SMA emerges from beneath the pancreas (most proximal right-side branch)
- Enters the transverse mesocolon
- Divides into:
- Right branch → anastomoses with the right colic artery
- Left branch → anastomoses with the left colic artery (branch of the inferior mesenteric artery) at the splenic flexure - this junction is the marginal artery of Drummond / arc of Riolan
- Supplies: transverse colon (right two-thirds)
4. Right Colic Artery (Second right-side branch)
- An inconsistent branch (may be absent or arise from the ileocolic artery)
- Passes retroperitoneally to the right to reach the ascending colon
- Divides into:
- Ascending branch → anastomoses with the middle colic artery
- Descending branch → anastomoses with the ileocolic artery
- Supplies: ascending colon
5. Ileocolic Artery (Terminal / most distal right-side branch)
- The most constant branch of the SMA on the right side
- Passes downward and to the right toward the right iliac fossa
- Divides into superior and inferior branches:
Superior branch: ascends along the ascending colon → anastomoses with the right colic artery
Inferior branch subdivides further into:
- Colic branch - supplies the first part of the ascending colon
- Anterior and posterior cecal branches - supply the cecum
- Appendicular artery - runs in the free margin of the mesoappendix to supply the appendix (note: end-artery with limited collateral, important in appendicitis)
- Ileal branch - passes left and ascends to supply terminal ileum, anastomoses with the final jejunal/ileal branch of the SMA
Full Distribution Map
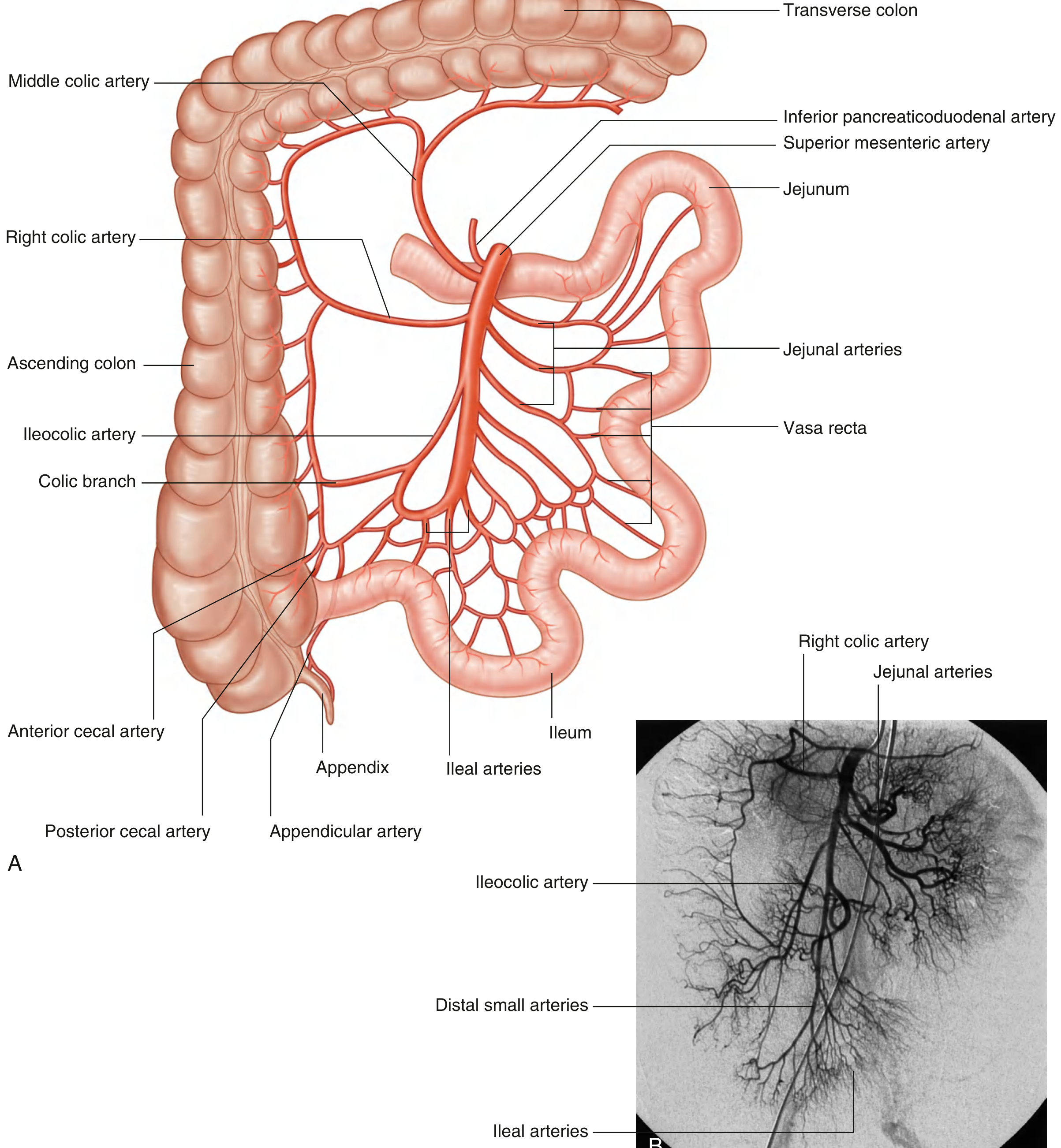
(A) Full distribution of the SMA showing all branches; (B) digital subtraction angiography (DSA) showing the living appearance of the SMA and its branches.
Territory Supplied
| Structure | SMA Branch |
|---|---|
| Lower duodenum (D3/D4) | Inferior pancreaticoduodenal artery |
| Head & uncinate process of pancreas | Inferior pancreaticoduodenal artery |
| Jejunum | Jejunal arteries |
| Ileum (most) | Ileal arteries |
| Terminal ileum | Ileocolic artery (ileal branch) |
| Cecum | Ileocolic artery (cecal branches) |
| Appendix | Appendicular artery |
| Ascending colon | Ileocolic + right colic arteries |
| Transverse colon (right 2/3) | Middle colic artery |
Collateral Circulation
The SMA has two important collateral networks:
-
Celiac-SMA anastomosis: Via pancreaticoduodenal arcade - superior pancreaticoduodenal (celiac side) ↔ inferior pancreaticoduodenal (SMA side). This is the major collateral if either vessel is occluded proximally.
-
SMA-IMA anastomosis: Via the marginal artery of Drummond (running along the inner margin of the colon) and the arc of Riolan (central anastomotic vessel in the mesocolon) - connects middle colic (SMA territory) with left colic (IMA territory) at the splenic flexure. The splenic flexure and sigmoid colon have limited anastomoses, making them vulnerable to ischemia ("watershed zones").
Clinical Relevance
- SMA Syndrome: The SMA-SMV pedicle compresses the 3rd part of the duodenum, causing intermittent obstruction - seen in rapid weight loss, prolonged bed rest, body casting
- Acute Mesenteric Ischemia: SMA embolism (most common at the origin or just distal to the middle colic take-off) causes catastrophic midgut infarction - accounts for ~25% of intestinal ischemia cases
- Vasa recta as end-arteries: Since vasa recta lack anastomoses, focal ischemia can occur even with partial occlusion of terminal branches
- Appendicular artery: Functionally an end-artery - appendicitis with thrombosis leads rapidly to gangrene
- SMA and pancreatic surgery: The SMA runs posterior to the neck of the pancreas - Whipple procedure (pancreaticoduodenectomy) requires careful SMA dissection; SMA involvement by pancreatic cancer is a key determinant of resectability
Sources: Gray's Anatomy for Students, pp. 411-413 | Sleisenger & Fordtran's Gastrointestinal and Liver Disease, p. 2390
This is a shared conversation. Sign in to Orris to start your own chat.