Find images for fenestrated subtotal cholecystectomy and reconstituted subtotal cholecystectomy.
Reading File
Searching Images
fenestrated subtotal cholecystectomy
Searching Images
reconstituting subtotal cholecystectomy
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Here are the images organized by subtype, with contextual descriptions.
Fenestrated Subtotal Cholecystectomy
In this technique, the gallbladder is opened and the body/fundus removed, but the infundibulum/neck is left open (not closed). The cystic duct orifice is plugged with a purse-string suture or left to drain. It carries a higher risk of postoperative bile leak/biliary fistula compared to the reconstituting type.
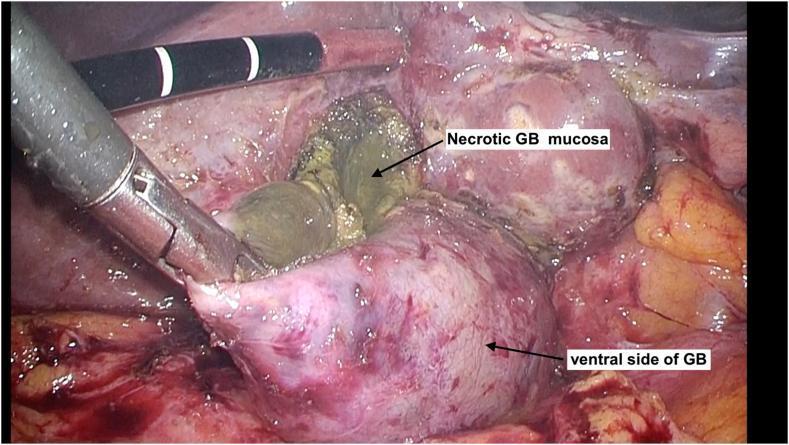
Image 1 — Laparoscopic fenestrating subtotal cholecystectomy (dome-down approach)
The gallbladder has been opened, exposing necrotic mucosa internally — the classic indication for choosing a fenestrating approach when CVS cannot be achieved.
Reconstituted (Reconstituting) Subtotal Cholecystectomy
In this technique, the gallbladder remnant/infundibular cuff is closed — sutured or stapled shut — leaving a small closed pouch. This reduces bile leak risk but carries a small risk of stone reformation and recurrent symptoms. Reintervention rates: ~26% vs ~32% for fenestrating.
Image 2 — Robotic-assisted reconstituting subtotal cholecystectomy
The infundibular cuff is being sutured internally with a V-Loc barbed suture using a MEGA SUTURECUT needle driver, creating a closed reconstituted remnant.
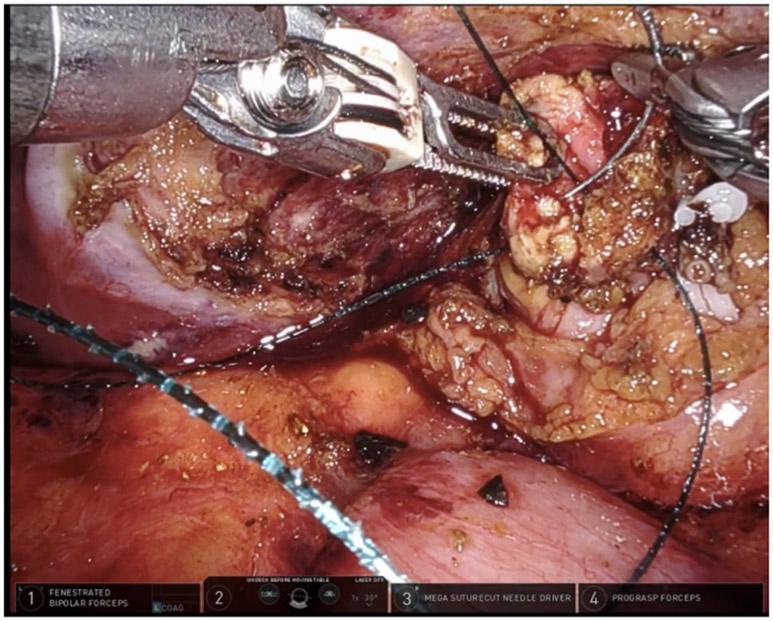
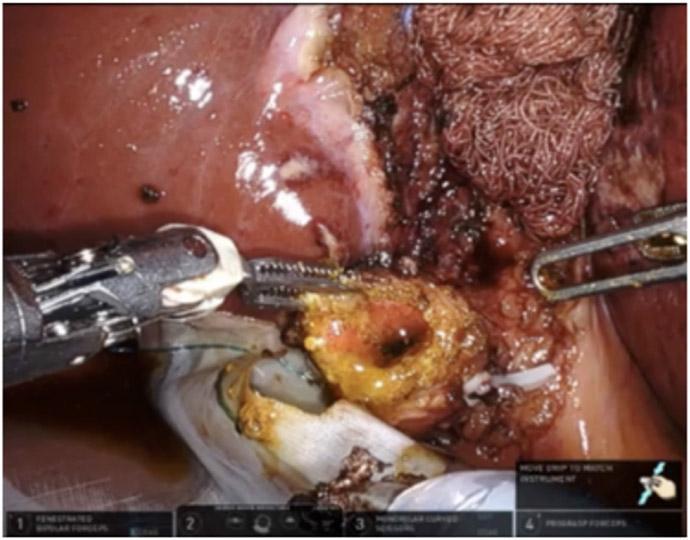
Image 3 — Robotic-assisted subtotal cholecystectomy (reconstituting phase)
Gallbladder infundibulum opened, revealing stones and bile at the cystic duct orifice; sutures at the periphery show the reconstituting closure being performed.
Additional Reference Images
Image 4 — Laparoscopic subtotal cholecystectomy with barbed suture closure (Panel A: gallbladder stump pre-closure; Panel B: stump closed with 0-0 barbed suture)
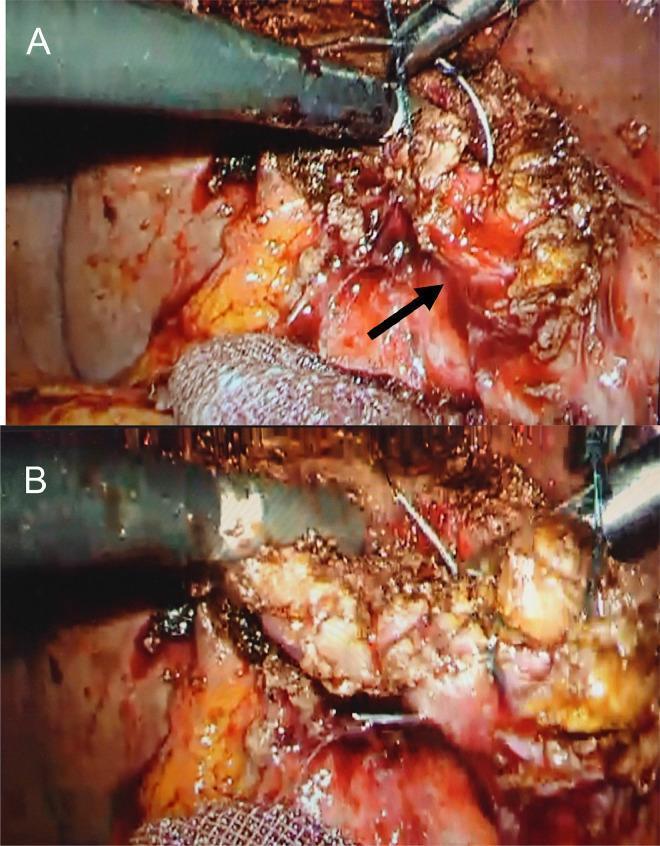
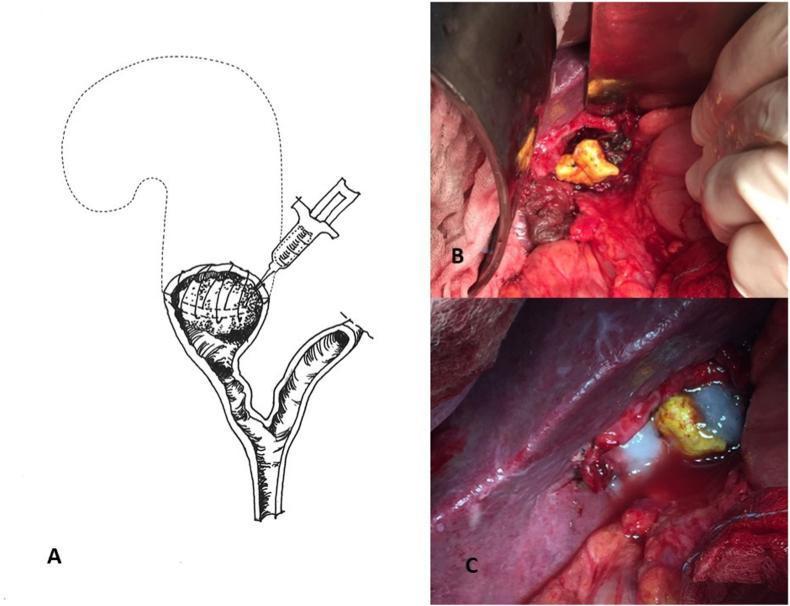
Image 5 — Subtotal cholecystectomy for Mirizzi Syndrome (Panel A: schematic of infundibular remnant with sealant; Panel B & C: intraoperative views with TachoSil® and fibrin glue burial technique)
Key distinction summary (from Mulholland & Greenfield's Surgery, 7e):
| Feature | Fenestrating | Reconstituting |
|---|---|---|
| Remnant closure | Open (purse-string at cystic duct) | Sutured/stapled shut |
| Main risk | Bile leak / biliary fistula | Stone reformation, recurrent symptoms |
| Reintervention rate | ~32% | ~26% |
| Completion cholecystectomy needed | ~9% | ~4% |
When should we prefer this surgery over total cholecystectomy?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
"subtotal cholecystectomy" indications outcomes
Here is a comprehensive answer drawn from multiple surgical textbooks.
When to Prefer Subtotal over Total Cholecystectomy
Subtotal cholecystectomy is a bailout ("damage control") procedure — it is not a first-line option but is chosen when completing a safe total cholecystectomy would put the patient at unacceptable risk, primarily of bile duct injury. The core principle is: "If in doubt, don't take it out completely."
Primary Indications
1. Inability to Achieve the Critical View of Safety (CVS)
The single most important trigger. When inflammation, fibrosis, or anatomical distortion makes it impossible to clearly identify the two-structure rule (only cystic duct + cystic artery connecting the gallbladder to the hepatoduodenal ligament), subtotal cholecystectomy is preferred over risking misidentification and transecting the common bile duct.
"Several strategies for mitigating the risk of bile duct injury have been proposed including obtaining the 'critical view of safety'... and various forms of subtotal cholecystectomy." — Mulholland & Greenfield's Surgery, 7e
2. Severe Acute or Gangrenous Cholecystitis
When the gallbladder is gangrenous, the tissue is often too friable for safe dissection. The infundibulum is divided high, stones removed, and the remnant managed based on tissue quality. Note: in gangrenous tissue, the infundibulum may be too friable even for suture closure (favouring the fenestrating subtype).
"If the cystic structures cannot be safely dissected from the portal structures but the gallbladder is no longer intact or is gangrenous, a partial/subtotal cholecystectomy can be performed." — Current Surgical Therapy, 14e
3. Severe Inflammatory Adhesions / Frozen Hepatocystic Triangle
Dense adhesions from repeated episodes of cholecystitis, previous surgery, or penetrating peptic ulcer can obliterate tissue planes around Calot's triangle, making safe dissection impossible.
4. Impacted Stone at the Cystic Duct / Mirizzi Syndrome
A large stone impacted at the infundibulum or cystic duct — especially in Mirizzi syndrome — can fuse the gallbladder neck to the common bile/hepatic duct. Attempting total removal risks direct bile duct injury. The infundibular remnant (with stone buried or sealed) is left in situ.
5. Portal Hypertension / Cirrhosis
Dilated collateral veins on the gallbladder wall in portal hypertension make total cholecystectomy hazardous due to uncontrollable bleeding. Subtotal cholecystectomy with stone retrieval avoids the vascular bed.
"If varices are found on the gallbladder wall intraoperatively, subtotal cholecystectomy and stone retrieval is an option to avoid bleeding." — Mulholland & Greenfield's Surgery, 7e
6. Gallbladder Firmly Adherent to Liver with No Tissue Plane
When the posterior gallbladder wall is inseparable from the liver parenchyma and blunt dissection causes repeated hepatic parenchymal disruption (bleeding, bile leak risk), the back wall is left on the liver bed with extensive mucosa ablation by electrocautery.
Tokyo Guidelines Grading Context
| Grade | Severity | Surgical Implications |
|---|---|---|
| Grade I (mild) | Minimal inflammation | Total laparoscopic cholecystectomy feasible |
| Grade II (moderate) | Marked inflammation, hepatocystic triangle involvement | Subtotal cholecystectomy may be needed |
| Grade III (severe) | Organ dysfunction, frozen triangle | Bailout strongly favoured; cholecystostomy or subtotal cholecystectomy |
"As the grade of cholecystitis increases from I to II or III, a laparoscopic procedure becomes increasingly difficult to complete safely." — Sabiston Textbook of Surgery
Choosing Between Fenestrating and Reconstituting
| Scenario | Preferred Subtype |
|---|---|
| Tissue is pliable, cystic duct identifiable | Reconstituting (closed remnant — lower bile leak risk) |
| Gangrenous, friable tissue; suturing not feasible | Fenestrating (open; accept bile leak risk with drain) |
| Very obese or technically hostile field | Either; based on surgeon judgement |
Important Caveats
- Subtotal is not without consequences: reintervention rates reach 26–32%, and completion cholecystectomy may eventually be required (especially in younger, fit patients).
- A closed-suction drain must always be left in the gallbladder fossa given the high risk of postoperative bile leak.
- The residual gallbladder pouch carries risk of stone reformation, mucocele, and recurrent cholecystitis — long-term follow-up is warranted.
(Recent evidence: A 2026 meta-analysis [PMID 41365761] specifically examined indications, techniques, and outcomes of completion cholecystectomy after subtotal procedures — indicating ongoing refinement of when and how to manage these remnants.)
Sources: Mulholland & Greenfield's Surgery 7e | Sabiston Textbook of Surgery | Current Surgical Therapy 14e | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.