SECTION II – Short Notes 1. Approach to a patient with Proteinuria
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Searching PubMed
proteinuria evaluation management guidelines
I now have comprehensive, authoritative content from multiple sources. Let me compose the detailed short note.
Approach to a Patient with Proteinuria
Definition
Proteinuria is defined as the abnormal excretion of protein in urine. Normal urine protein excretion is less than 150 mg/24 hours, composed of ~20-30 mg albumin, 10-20 mg low-molecular-weight proteins, and 40-60 mg secreted proteins (e.g., Tamm-Horsfall protein, IgA). Proteinuria is both a cardinal manifestation of glomerular injury and a pathogenetic factor driving progression of renal dysfunction.
- Comprehensive Clinical Nephrology, 7th Edition, Chapter 16
Classification of Proteinuria
1. By Mechanism
| Type | Mechanism | Examples |
|---|---|---|
| Glomerular | Increased permeability of the glomerular filtration barrier | Nephrotic syndrome, GN, diabetic nephropathy |
| Tubular | Impaired reabsorption of normally filtered low-molecular-weight proteins | Tubulointerstitial nephritis, Fanconi syndrome, ATN |
| Overflow | Overproduction of low-MW proteins exceeding tubular reabsorption | Multiple myeloma (Bence Jones proteins), hemoglobinuria, myoglobinuria |
| Secretory | Abnormal secretion of proteins into tubular lumen | UTI, tubular inflammation |
2. By Quantity
| Category | 24-hour Excretion | Albumin/Creatinine Ratio |
|---|---|---|
| Normal | < 150 mg/day | < 30 mg/g |
| Microalbuminuria (low-grade) | 30-300 mg albumin/day | 30-300 mg/g |
| Nonnephrotic proteinuria | 300 mg - 3.5 g/day | - |
| Nephrotic-range proteinuria | > 3.5 g/day | > 3 g/g |
- Harrison's Principles of Internal Medicine 22e, Table 326-1
- Comprehensive Clinical Nephrology, 7th Edition
3. By Duration/Pattern
- Transient/Functional: Fever, vigorous exercise, emotional stress, obesity, sleep apnea, congestive heart failure. Generally < 1 g/24 h, non-sustained. Benign.
- Orthostatic (Postural): Protein appears only in urine collected when upright; absent in recumbent (first-morning) specimen. Most common cause of isolated proteinuria in adolescents and young adults. Excellent prognosis.
- Persistent/Fixed: Present in upright and supine samples. More likely to indicate significant underlying renal disease.
Causes of Proteinuria
Glomerular Diseases
- Primary: Minimal change disease (MCD), focal segmental glomerulosclerosis (FSGS), membranous nephropathy, membranoproliferative GN (MPGN), IgA nephropathy
- Secondary: Diabetic nephropathy, lupus nephritis, amyloidosis, hypertensive nephropathy, post-infectious GN
Tubulointerstitial Diseases
- Reflux nephropathy, obstructive uropathy, interstitial nephritis, pyelonephritis, polycystic kidney disease, proximal tubulopathy
Overflow States
- Multiple myeloma (light chains/Bence Jones protein), hemolysis (hemoglobinuria), rhabdomyolysis (myoglobinuria), lysozymuria (monocytic leukemia)
Other
- Preeclampsia/eclampsia, heart failure, fever, exercise, hypertension
Clinical Presentation
Patients often do NOT know they have proteinuria unless they develop:
- Frothy/foamy urine (heavy proteinuria)
- Edema (hypoalbuminemia in nephrotic syndrome)
- Incidental finding on urine dipstick
Nephrotic syndrome pentad: Massive proteinuria (>3.5 g/day) + hypoalbuminemia + edema + hyperlipidemia + lipiduria
Nephritic syndrome: Proteinuria 1-2 g/24 h + hematuria with RBC casts + hypertension + oliguria + rising creatinine
- Harrison's Principles of Internal Medicine 22e
History
- Duration and severity of edema, frothy urine
- History of diabetes mellitus or hypertension (most common systemic causes)
- Recurrent UTIs, kidney stones, flank pain
- Drug history: NSAIDs, gold, penicillamine, heroin, captopril (rarely)
- Family history of kidney disease (Alport syndrome, FSGS)
- Recent URTI (post-streptococcal GN), skin infections, hepatitis B/C exposure (membranous nephropathy, MPGN)
- Symptoms of systemic disease: joint pain, rash, oral ulcers (SLE), weight loss (malignancy/myeloma)
- Recent vigorous exercise, fever (to exclude functional causes)
Physical Examination
- Vital signs: Blood pressure (hypertension suggests glomerular disease)
- Edema: Periorbital (early, especially in children), dependent, anasarca
- Skin: Malar rash (SLE), purpura (vasculitis, HSP), skin thickening (amyloid)
- Eyes: Diabetic retinopathy, Kayser-Fleischer rings
- Abdomen: Ascites, flank masses (polycystic kidneys)
- Signs of chronic liver disease: If secondary to hepatic disease
Investigations
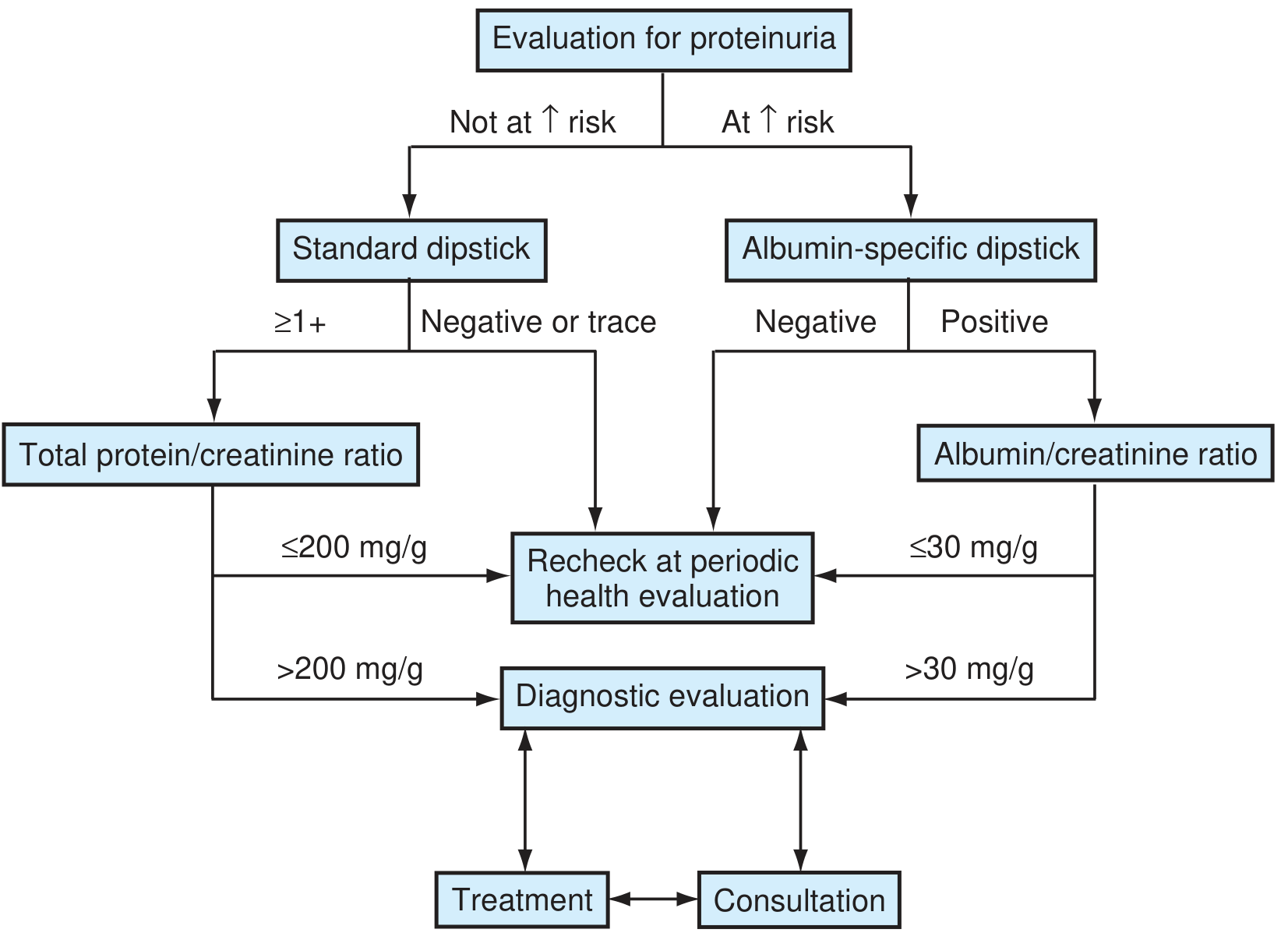
Step 1: Urine Dipstick
- Minimum 1+ if specific gravity ≤ 1.015; 2+ if SG > 1.015 is considered significant
- Detects albumin only - may miss Bence Jones proteins (use sulfosalicylic acid test for total protein)
- Positive result needs confirmation on repeat testing
Step 2: Quantification - Spot Urine Protein/Creatinine Ratio (UPr:UCr)
- Preferred to 24-hour collection in clinical practice
- Excellent correlation with 24-hour excretion
- Adults: > 0.2 is abnormal (equivalent to > 200 mg/g); > 3.0 = nephrotic range
- If at risk (DM, HTN): use albumin-specific dipstick then albumin/creatinine ratio (UACR); > 30 mg/g warrants further evaluation
24-hour collection is reserved for: suspected discordance with spot ratio, low or very high muscle mass, research purposes.
Step 3: Urine Microscopy
- RBC casts / dysmorphic RBCs: Glomerulonephritis
- WBC casts: Pyelonephritis, interstitial nephritis
- Granular casts: Non-specific, suggests parenchymal disease
- Oval fat bodies / lipid droplets: Nephrotic syndrome
- Free RBCs alone: May suggest urologic source
Step 4: Confirm Persistence
- Repeat dipstick on 2-3 occasions over weeks
- Most proteinuria in children (and some adults) is transient
Step 5: Orthostatic Testing
- Collect first-morning void (recumbent sample) and daytime (upright) sample separately
- Absence of proteinuria in morning sample = orthostatic proteinuria (benign)
- Confirmed by split 24-hour urine collection
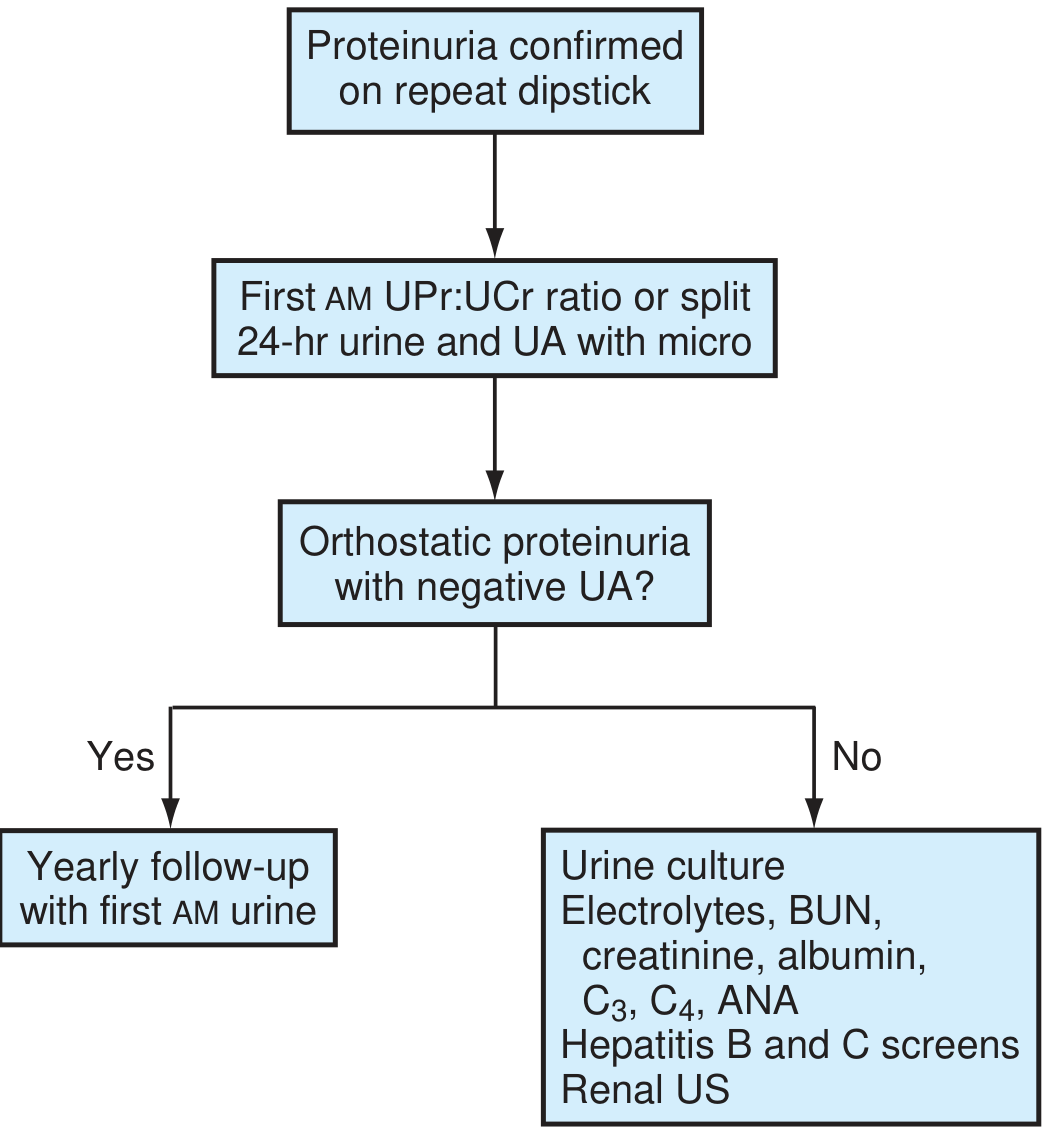
Step 6: Blood Tests
| Test | Purpose |
|---|---|
| Serum creatinine, BUN, eGFR | Renal function |
| Serum albumin | Hypoalbuminemia (nephrotic syndrome) |
| Serum electrolytes | Electrolyte imbalance |
| FBS / HbA1c | Diabetic nephropathy |
| Lipid profile | Hyperlipidemia (nephrotic syndrome) |
| CBC | Anemia of CKD, thrombocytopenia (TTP/HUS, SLE) |
| ANA, anti-dsDNA, C3, C4 | SLE, lupus nephritis |
| ANCA | Vasculitis |
| Hepatitis B and C serology | Secondary membranous nephropathy, MPGN |
| Serum/urine protein electrophoresis (SPEP/UPEP) | Myeloma, light chain disease |
| Serum complement (C3, C4, CH50) | Immune complex GN |
| Anti-GBM antibody | Goodpasture syndrome |
| ASO titer | Post-streptococcal GN |
Step 7: Imaging
- Renal ultrasound: Kidney size, echogenicity, cortical thickness, cysts, hydronephrosis, renal vein thrombosis (in nephrotic syndrome)
- Doppler for renal vein thrombosis (complication of nephrotic syndrome)
- CT/MRI: If structural anomaly or malignancy suspected
Step 8: Renal Biopsy
Indicated when:
- Nephrotic syndrome in adults without obvious cause
- Persistent nonnephrotic proteinuria (> 1-2 g/day) without explanation
- Suspected systemic disease with renal involvement
- Unexplained progressive renal failure with proteinuria
- Suspected rapidly progressive GN
Not routinely needed in:
- Children < 10 years with pure nephrotic syndrome (likely MCD - start steroids empirically)
- Orthostatic proteinuria (benign)
- Diabetic nephropathy with classic clinical picture and no atypical features
Age-Related Prevalence of Nephrotic Causes
| Cause | Children | Young Adults (White) | Middle/Old Age (White) |
|---|---|---|---|
| Minimal Change Disease | 78% | 23% | 21% |
| FSGS | 8% | 19% | 13% |
| Membranous Nephropathy | 2% | 24% | 37% |
| MPGN | 6% | 13% | 4% |
| Amyloid | 0% | 5% | 13% |
- Comprehensive Clinical Nephrology, 7th Edition, Table 16.3
Management Principles
General (before specific diagnosis)
- Treat underlying cause
- BP control: Target < 130/80 mmHg; ACE inhibitors or ARBs are first-line (antiproteinuric effect via reducing intraglomerular pressure + podocyte protection)
- Dietary protein restriction: 0.8 g/kg/day in CKD (avoid excessive restriction)
- Sodium restriction and diuretics: For edema
- Statin therapy: For hyperlipidemia in nephrotic syndrome
- Anticoagulation: Consider in nephrotic syndrome if serum albumin < 2.5 g/dL (high risk of thromboembolism)
- Infection prophylaxis: Pneumococcal vaccine (impaired opsonization in nephrotic syndrome)
Specific
- MCD: Corticosteroids (prednisone 1 mg/kg/day) - excellent response rate
- Lupus nephritis: Hydroxychloroquine ± immunosuppression depending on class
- Diabetic nephropathy: Optimize glycemia, BP control with RAAS blockade, SGLT-2 inhibitors (renoprotective)
- Membranous nephropathy: Observation for spontaneous remission vs. rituximab/cyclophosphamide/cyclosporine
Follow-up of Persistent Isolated Proteinuria
- Yearly assessment: BP, serum creatinine, serum albumin, urine microscopy, UPr:UCr ratio
- Orthostatic proteinuria: Annual first-morning urine check, reassurance
- Non-orthostatic isolated proteinuria persisting > 1 year: Renal biopsy may be indicated
Summary Algorithm
- Dipstick screening (risk-stratified: standard vs. albumin-specific)
- Confirm on repeat testing (exclude transient causes)
- Quantify with spot UPr:UCr ratio (or UACR)
- Orthostatic test - first-morning urine
- Urine microscopy - look for casts, dysmorphic RBCs
- Blood tests - renal function, albumin, glucose, immunology panel
- Imaging - renal ultrasound
- Renal biopsy - if indicated
Sources: Textbook of Family Medicine 9e; Comprehensive Clinical Nephrology, 7th Edition; Harrison's Principles of Internal Medicine 22e; Brenner and Rector's The Kidney, 2-Volume Set
Tell me the examination of pulse practicals in detail
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative sources. Let me compile the complete, detailed answer.
Examination of the Pulse - Practical Guide
Introduction
The pulse is the rhythmic expansion of an arterial wall caused by the pressure wave generated by ventricular systole. It is one of the most important clinical signs, reflecting the cardiovascular status of a patient. Examination of the pulse provides information about heart rate, rhythm, cardiac output, and the presence of valvular or vascular disease.
"The pulse gives a good indication of the cardiovascular condition of the patient. Abnormalities of the heart and vascular system, e.g., hypertension and hypotension, are also revealed in the pulse. Shock, fever and thyrotoxicosis are a few conditions which are well reflected in the pulse."
- S Das, A Manual on Clinical Surgery, 13th Edition
Sites of Pulse Examination
The pulse can be palpated at any accessible artery. The commonly examined sites are:
| Site | Artery | Clinical Use |
|---|---|---|
| Radial (most common) | Radial artery | Routine examination - rate, rhythm |
| Brachial | Brachial artery | Volume, character; when neck/radial inaccessible |
| Carotid | Common carotid | Best for character/contour assessment |
| Femoral | Femoral artery | Radio-femoral delay (coarctation) |
| Popliteal | Popliteal artery | Lower limb vascular disease |
| Dorsalis pedis | Dorsal foot artery | Peripheral vascular disease |
| Posterior tibial | Behind medial malleolus | Peripheral vascular disease |
| Temporal | Superficial temporal | Temporal arteritis |
The carotid and brachial arteries are preferred for assessing character and contour of the pulse because they are closer to the heart and the waveform is less distorted.
Practical Technique of Pulse Examination
Patient Position
- Patient relaxed, preferably supine or sitting
- Arm resting comfortably at the level of the heart
- Avoid examining immediately after exertion
Examiner's Position
- Stand to the patient's right side
- For radial pulse: hold the patient's wrist with your right hand, using 2nd, 3rd, and 4th finger pads placed on the lateral aspect of the volar wrist (never use the thumb - it has its own pulsation)
- Apply moderate, steady pressure - too light misses it; too heavy obliterates it
Parameters to Assess (RRTVC + W)
1. Rate
Count the number of beats per minute.
- Normal: 60-100 bpm
- Bradycardia: < 60 bpm
- Causes: Athletes, vagal stimulation, hypothyroidism, complete heart block, beta-blockers, inferior MI
- Tachycardia: > 100 bpm
- Causes: Fever (each 1°F rise ~ +10 bpm), pain, anxiety, anemia, thyrotoxicosis, heart failure, shock, SVT/VT
How to count: Count for a full 60 seconds if irregular; count for 15 seconds x4 if regular.
2. Rhythm
Assess whether beats occur at regular or irregular intervals.
| Type | Description | Examples |
|---|---|---|
| Regular | Equal intervals between beats | Normal sinus rhythm |
| Regularly irregular | Repeating pattern of irregularity | Sinus arrhythmia, 2nd degree heart block (Wenckebach), bigeminy |
| Irregularly irregular | No pattern to irregularity | Atrial fibrillation (AF), multiple ectopics, atrial flutter with variable block |
Sinus arrhythmia - pulse speeds up with inspiration and slows with expiration; normal in young patients, disappears when breath is held.
Atrial fibrillation - completely irregular with no pattern. Check for a pulse deficit (difference between apical rate by auscultation and radial rate) - present in AF due to some beats not producing enough stroke volume to reach periphery.
3. Tension (Compressibility)
Correlates with the diastolic blood pressure.
- Press on the artery proximal to your palpating fingers until the pulse is obliterated
- Increased tension = high diastolic pressure (hypertension)
- Decreased tension = low diastolic pressure (shock, aortic regurgitation)
4. Volume (Amplitude)
Reflects pulse pressure (systolic BP minus diastolic BP) and indirectly stroke volume.
| Volume | Description | Causes |
|---|---|---|
| Normal | Full, moderate amplitude | Normal cardiac output |
| High volume (bounding) | Easily felt, wide excursion | Aortic regurgitation, thyrotoxicosis, fever, pregnancy, anemia, exercise |
| Low volume (weak/thready) | Barely palpable, narrow excursion | Shock, heart failure, severe aortic stenosis, cardiac tamponade, severe hypovolemia |
5. Character (Waveform Contour)
Best assessed at the carotid or brachial artery. Reflects pressure changes during systole and diastole.
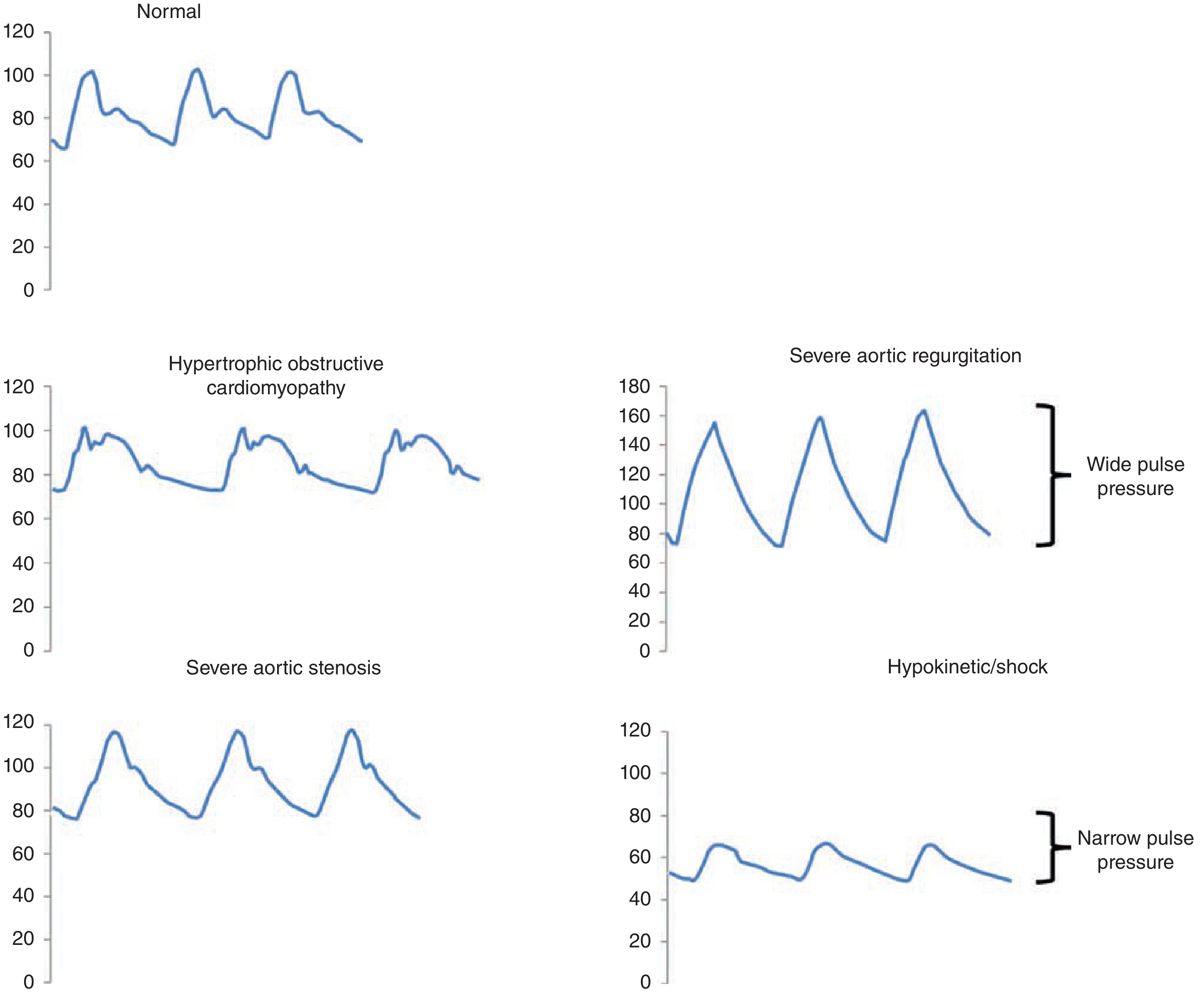
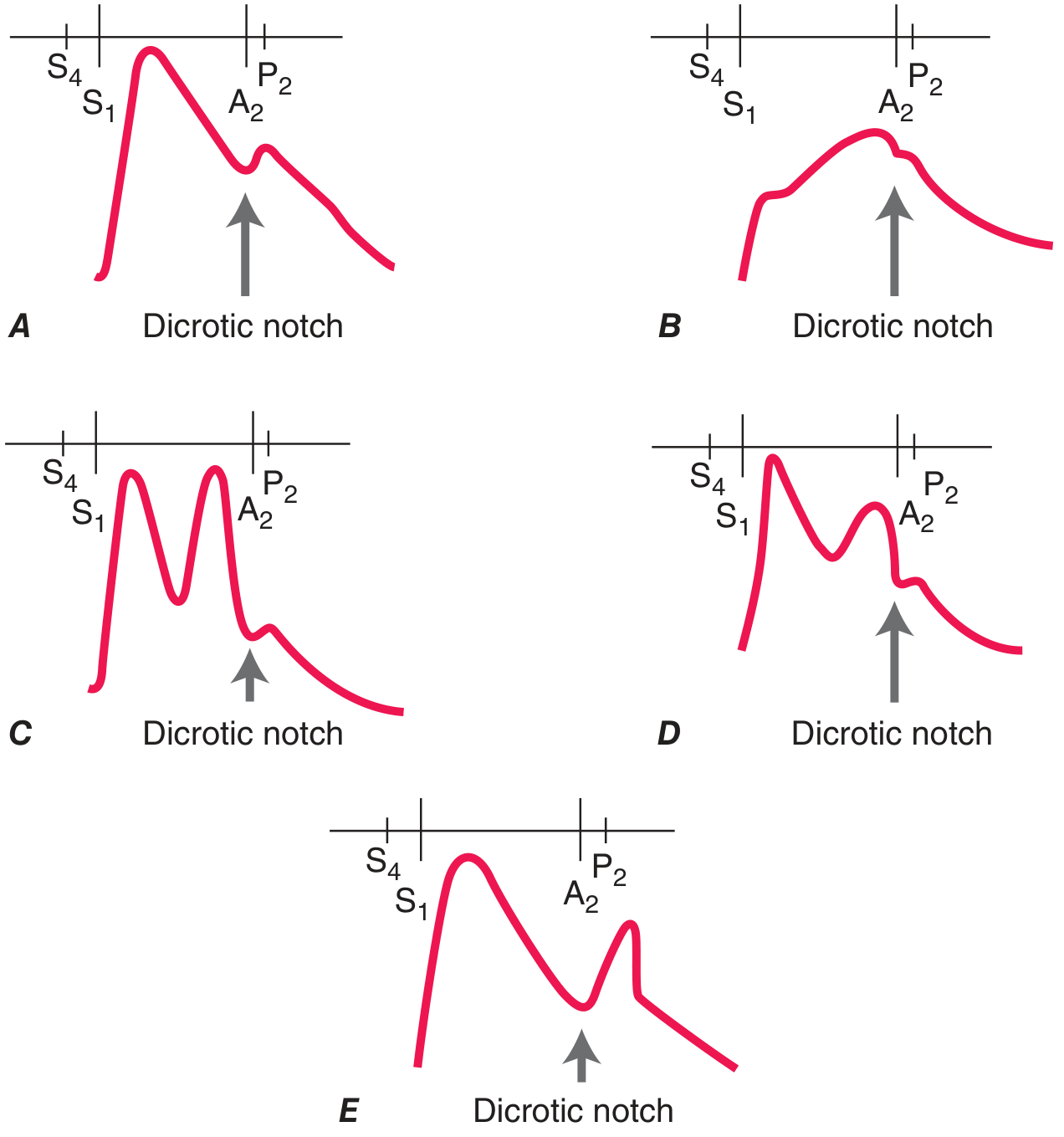
Normal Pulse Waveform
- Gradual smooth upstroke followed by a rounded peak and downstroke
- Dicrotic notch - small notch on the descending limb caused by aortic valve closure (only visible on waveform tracings, not palpable normally)
Abnormal Character - Named Pulses
A. Pulsus Parvus et Tardus (Small and Slow)
- Low amplitude + delayed, prolonged upstroke
- Cause: Severe aortic stenosis (fixed LV outflow obstruction slows ejection)
- May have an anacrotic notch (vibration felt on ascending limb = "anacrotic pulse")
B. Collapsing Pulse / Water Hammer Pulse (Corrigan's Pulse)
- Rapid forceful upstroke followed by an abrupt, sudden collapse
- High volume + wide pulse pressure
- Cause: Severe aortic regurgitation, also thyrotoxicosis, patent ductus arteriosus, severe anemia, arteriovenous fistula
- Clinical test: Elevate the patient's arm above the head - the collapsing quality becomes more dramatic; felt as a slapping sensation against the examiner's palm
C. Bisferiens Pulse (Double-Peak)
- Two distinct systolic peaks per heartbeat
- Causes:
- Mixed aortic valve disease (AR predominant) - two peaks in systole
- HOCM - first peak = percussion wave (early systole, before obstruction); second peak = tidal wave; "spike-and-dome" pattern
- Harrison's: "A bifid pulse is also described in patients with hypertrophic obstructive cardiomyopathy (HOCM), with inscription of percussion and tidal waves."
D. Dicrotic Pulse
- Two peaks - one systolic, one diastolic (exaggeration of dicrotic notch becomes palpable)
- Cause: Severe hypotension/shock, sepsis, severe peripheral vasoconstriction; also seen during intra-aortic balloon counterpulsation
E. Pulsus Alternans
- Beat-to-beat alternation in amplitude of pulse (alternating strong and weak beats)
- Regular rhythm (not respirophasic - distinguishes from pulsus paradoxus)
- Cause: Severe LV systolic dysfunction (e.g., advanced heart failure)
- Ominous sign of profound ventricular dysfunction
- Fuster and Hurst: "The presence of pulsus alternans is an ominous sign, suggesting very profound severe ventricular systolic dysfunction."
F. Pulsus Paradoxus
- Exaggerated fall in systolic BP > 10 mmHg during normal inspiration
- Measured with sphygmomanometer: note pressure at which Korotkoff sounds are first heard (expiration only) vs. heard every beat; difference > 10 mmHg = paradoxus
- Causes: Cardiac tamponade (most classic), massive pulmonary embolism, severe asthma/COPD, tension pneumothorax, hemorrhagic shock
- Mechanism: Inspiration expands right heart at the expense of LV (interventricular dependence) - tamponade exaggerates this
- Harrison's: "A pulsus paradoxus may be palpable at the brachial or femoral artery when the pressure difference exceeds 15 mmHg."
G. Bigeminal Pulse
- Alternating strong and weak beats, but the weak beat follows prematurely (not evenly spaced)
- Cause: Bigeminy (every normal beat followed by a PVC)
- Distinguished from pulsus alternans by the irregular rhythm
6. Wall Condition (Vessel Wall)
Roll the artery under your fingers after obliterating the pulsation.
- Normal: Soft, pliable, non-palpable wall
- Thickened/tortuous: Atherosclerosis ("pipe-stem" artery in severe disease)
- Hard, non-compressible: Calcified wall (Monckeberg's sclerosis)
Radio-Femoral Delay
Simultaneously palpate the radial pulse (right) and femoral pulse with both hands.
- Normally both are felt simultaneously
- Delay of femoral behind radial: Suggests coarctation of the aorta (narrowing distal to subclavian artery)
- Also check radio-radial inequality (unequal carotid-subclavian anatomy, aortic dissection, subclavian artery aneurysm/stenosis)
Radio-Radial Inequality
Palpate both radial pulses simultaneously.
- Causes of absent/reduced pulse on one side:
- Thoracic outlet syndrome
- Aortic dissection
- Subclavian artery stenosis / Takayasu's arteritis
- Previous arterial line / trauma
Special Maneuvers
Carotid Pulse Assessment
- Best for character - palpate medial to sternocleidomastoid at the mid-neck level
- Use one side at a time - never bilateral simultaneous (risk of carotid sinus stimulation causing syncope or arrhythmia, especially in elderly)
- Mobilize SCM laterally to palpate the artery properly
Hepatojugular Reflux
- Apply firm pressure over the right upper quadrant for 30 seconds while watching JVP
- Rise > 3 cm = raised venous pressure / right heart failure
Summary Table: Pulse Abnormalities at a Glance
| Pulse Type | Rate | Rhythm | Volume | Character | Condition |
|---|---|---|---|---|---|
| Normal | 60-100 | Regular | Moderate | Smooth up, gradual down | - |
| Pulsus parvus et tardus | - | Regular | Low | Slow upstroke, delayed peak | Severe AS |
| Collapsing / Water hammer | - | Regular | High | Rapid rise, sudden collapse | Severe AR, PDA, thyrotoxicosis |
| Bisferiens | - | Regular | Normal/high | Two systolic peaks | AR+AS, HOCM |
| Dicrotic | - | Regular | Low | Systolic + diastolic peaks | Shock, sepsis |
| Pulsus alternans | - | Regular | Varies beat-to-beat | Alternating strong/weak | Severe LV failure |
| Pulsus paradoxus | - | Regular | Drops with inspiration | Inspiratory drop >10 mmHg | Tamponade, severe asthma |
| Bigeminal | - | Irregularly regular | Strong then weak | Normal then premature weak beat | Bigeminy |
| Bradycardic | <60 | Variable | - | - | Heart block, hypothyroid |
| Tachycardic | >100 | Variable | - | - | Fever, sepsis, SVT |
| Thready | - | Regular | Very low | Barely palpable | Shock, tamponade |
Clinical Correlates to Always Remember
- AF = Irregularly irregular + pulse deficit (use apex-radial pulse difference)
- Complete heart block = Slow rate (~30-40 bpm), cannon 'a' waves in JVP
- Cardiac tamponade = Low volume + pulsus paradoxus + raised JVP (Beck's triad: raised JVP + muffled heart sounds + hypotension)
- Severe AR = Collapsing pulse + wide pulse pressure + low diastolic BP
- Severe AS = Pulsus parvus et tardus + narrow pulse pressure
- HOCM = Spike-and-dome bisferiens pulse + increases with Valsalva
- Coarctation = Radio-femoral delay + hypertension in arms + hypotension in legs
Sources: Fuster and Hurst's The Heart, 15th Edition; Harrison's Principles of Internal Medicine 22e; S Das, A Manual on Clinical Surgery, 13th Edition
This is a shared conversation. Sign in to Orris to start your own chat.