Discuss from basics to advance and all strategies, algorithms and recommendations from Latest ASRA Guidelines important for Anaesthesiology consultants worldwide
Reading File
Finding Sources
Searching PubMed
ASRA guidelines regional anesthesia anticoagulation
Searching the Web
ASRA 2022 guidelines regional anesthesia anticoagulation neuraxial peripheral nerve blocks key recommendations anesthesiology
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
ASRA regional anesthesia guidelines anticoagulants DOAC neuraxial
Reading Web Page
https://asra.com/news-publications/asra-updates/blog-landing…
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
regional anesthesia anticoagulation guidelines spinal epidural hematoma prevention
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://history.mayoclinic.org/wp-content/uploads/2024/05/RE…
Searching PubMed
ASRA checklist ultrasound guided regional anesthesia complications prevention
Loading Image
ASRA Guidelines: Comprehensive Review for Anaesthesiology Consultants
Sources: Miller's Anesthesia 10e, Morgan & Mikhail's Clinical Anesthesiology 7e, Barash's Clinical Anesthesia 9e, Sabiston Textbook of Surgery, ASRA 4th Edition Guidelines (Horlocker et al.), ASRA 2025 Update (ASRA.com), NYSORA, Mayo Clinic PDF
1. Background and Context
The American Society of Regional Anesthesia and Pain Medicine (ASRA) publishes evidence-based guidelines covering four primary domains:
- Anticoagulation and regional anesthesia (the most widely cited, with editions in 1998, 2003, 2010, 2018/4th edition, and 2022/2025 updates)
- Local anesthetic systemic toxicity (LAST) prevention and treatment
- Infection control in regional anesthesia
- Ultrasound guidance and patient safety
The 1993 introduction of LMWH in North America was accompanied by a cluster of spinal hematoma cases, prompting the FDA health advisory of December 1997 and the first ASRA consensus conference. Since then, ASRA guidelines have become the global benchmark for safe neuraxial and peripheral nerve block practice in anticoagulated patients.
Core principle: Timing of needle/catheter insertion and removal must reflect the pharmacokinetic properties of the specific anticoagulant - not a one-size-fits-all rule.
2. Fundamental Concepts: Why These Guidelines Exist
2.1 Risk of Spinal Epidural Hematoma (SEH)
- Incidence: approximately 1:150,000 epidurals and 1:220,000 spinal anesthetics in the general population
- In anticoagulated patients, incidence climbs dramatically
- SEH causes cord ischemia; outcomes depend on time to surgical decompression
- Neurological recovery is time-critical - laminectomy within 6-8 hours of symptom onset is the standard recommendation
Risk factors for SEH:
- Anticoagulant or antiplatelet therapy
- Multiple attempts at needle placement / traumatic or bloody tap
- Indwelling epidural catheter during anticoagulation
- Female sex, older age
- Renal impairment (affects DOAC clearance)
- Anatomic abnormality of the spine
2.2 Procedure Risk Stratification
ASRA classifies procedures into three hemorrhagic risk categories - a concept expanded in the 2018/4th Edition:
| Risk Category | Examples |
|---|---|
| High risk | Neuraxial blocks (epidural, spinal, combined spinal-epidural), deep plexus blocks (lumbar plexus/psoas compartment, paravertebral), celiac plexus, neurolytic blocks |
| Intermediate risk | Interscalene, femoral, sciatic, infraclavicular, popliteal |
| Low risk | Superficial/compressible blocks: TAP, ilioinguinal, supraclavicular, digital, PECS |
Key principle: Deep, non-compressible blocks should be managed with the same caution as neuraxial procedures regarding anticoagulation.
3. Anticoagulants: Drug-by-Drug ASRA Recommendations
Sites of action of anticoagulant drugs:
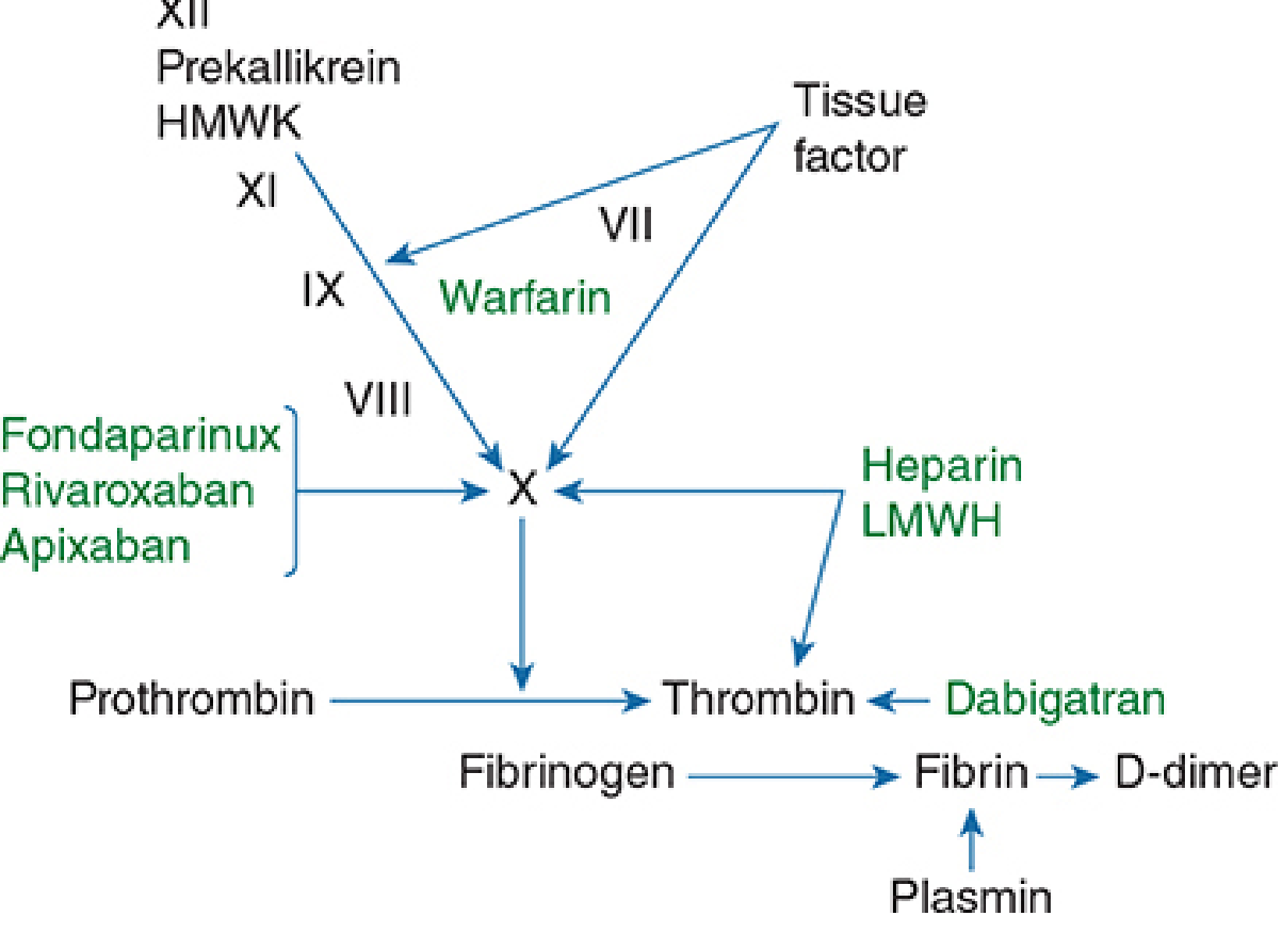
3.1 Warfarin (Vitamin K Antagonist)
Mechanism: Reduces factors VII, IX, X, and prothrombin
ASRA Recommendations:
- Stop warfarin 4-5 days before neuraxial procedure
- Confirm INR is normal (≤1.4 by ASRA; ≤1.4-1.5 by ESA) before proceeding
- If only a single dose of warfarin has been given, INR is typically normal and neuraxial block may be performed
- With an indwelling neuraxial catheter: check INR daily; remove catheter when INR ≤1.5
- When INR is 1.5-3.0, catheter can be maintained with caution; neurological monitoring mandatory
- When INR >3.0: hold or reduce warfarin; do not remove catheter until INR falls
- Restart: 12-24 hours post-procedure
Monitoring: PT/INR is the appropriate test
Note: ASRA (unlike ESA) does NOT permit warfarin to be administered with an indwelling neuraxial catheter in place
3.2 Unfractionated Heparin (UFH)
Mechanism: Potentiates antithrombin III to inhibit both thrombin (IIa) and Factor Xa
Subcutaneous Prophylactic UFH (5,000 units BID)
- No contraindication to neuraxial anesthesia
- Wait 4-6 hours from last dose before needle/catheter placement
- Catheter removal: 4-6 hours after last dose, 1 hour before next dose
- Administer first post-op dose no sooner than 1 hour after catheter removal
Subcutaneous Prophylactic UFH (TID - three times daily, >20,000 U/day)
- 2025 update: ASRA now recommends against neuraxial procedures in patients on a thrice-daily regimen pending further data (associated with spontaneous hematoma reports)
- If essential, assess coagulation status; recommend aPTT or anti-Xa monitoring
Intraoperative IV UFH (e.g., vascular surgery)
- Delay heparin at least 1 hour after needle/catheter placement
- Remove catheter 2-4 hours after last heparin dose, 1 hour before next dose
- Monitor aPTT or ACT
- Avoid neuraxial block in patients with pre-existing coagulopathy
- A traumatic/bloody tap: inform surgeon; consider delaying heparinization 24 hours
High-dose therapeutic UFH (>10,000 U SC per dose or >20,000 U/day)
- Neuraxial block 24 hours after last dose
- Assess coagulation status before proceeding (Grade 2C)
3.3 Low Molecular Weight Heparin (LMWH)
The drug class that originally triggered the ASRA guidelines. LMWH preferentially inhibits Factor Xa over thrombin.
Golden rule: "The smallest effective dose of LMWH should be administered."
| Dose | Pre-procedure interval | Post-procedure / catheter removal interval |
|---|---|---|
| Prophylactic (e.g., enoxaparin 40mg OD or 30mg BID) | 12 hours | First post-op dose ≥12 hours after single-injection spinal; ≥24 hours ideally |
| Therapeutic (e.g., enoxaparin 1 mg/kg BID or 1.5 mg/kg OD) | 24 hours | Catheter removal 24 hours after last dose; next dose 4 hours after catheter removal |
Important caveats:
- Anti-Xa level is NOT predictive of bleeding risk and should NOT be used to adjust timing
- Single-dose spinal anesthetic is the safest neuraxial technique in patients receiving perioperative LMWH
- Twice-daily LMWH in the presence of an indwelling epidural catheter is not recommended
- Postoperative LMWH administration should be delayed as long as possible (minimum 12 hours, ideally 24 hours after surgery)
- Assess platelet count if LMWH >4 days (HIT risk); hold LMWH if platelets <100,000
3.4 Fondaparinux (Indirect Factor Xa Inhibitor)
ASRA 4th Edition: Actually recommends against neuraxial procedures in patients on fondaparinux due to its irreversible binding, long half-life (~17-21 hours), and lack of reversal agent at the time of initial guideline publication.
- If neuraxial block is considered essential: wait ≥36-42 hours after last dose (2.5 mg OD)
- European guidelines: 36 hours pre-procedure, 6-12 hours post-procedure before restarting
- ASRA: if a neuraxial procedure is performed at day 5 post-fondaparinux, a platelet function test is recommended
3.5 Direct Oral Anticoagulants (DOACs) - The Most Updated Section
DOACs are now the most common anticoagulants encountered. The 2022 ASRA update and 2025 ASRA update introduced major refinements compared to earlier editions, including differentiation by dose, renal function, and laboratory thresholds.
Acceptable Laboratory Thresholds (NEW - 2025 ASRA):
Before proceeding with neuraxial or deep plexus/peripheral block despite not meeting time criteria:
- Residual DOAC level <30 ng/mL (calibrated drug-specific assay) OR
- Anti-Xa activity ≤0.1 IU/mL (for Xa inhibitors, calibrated to specific drug)
- For dabigatran: Thrombin time (TT) or dilute thrombin time (dTT) - PT/INR/aPTT are unreliable
- Reversal agents (andexanet alfa, idarucizumab, PCC) are NOT recommended for routine reversal prior to elective neuraxial procedures in the 2025 guidelines
3.5.1 Rivaroxaban (Factor Xa Inhibitor, once daily)
| Dose | Hold interval | Restart (after catheter removal) |
|---|---|---|
| Low dose (10 mg OD, CrCl >15 mL/min) | 24 hours (30 hrs if CrCl 15-30 mL/min) | 6 hours after catheter removal |
| High dose (15-20 mg OD) | 72 hours (3 days) | 6 hours after catheter removal |
| Inadvertent dosing with catheter in situ | - | 22-26 hours before catheter removal OR check anti-Xa |
3.5.2 Apixaban (Factor Xa Inhibitor, twice daily)
| Dose | Hold interval | Restart |
|---|---|---|
| Low dose (2.5 mg BID) | 36 hours | 6 hours post-catheter removal |
| High dose (5 mg BID, or 2.5 mg BID in patients <60 kg or significantly reduced CrCl) | 72 hours | 6 hours post-catheter removal |
| Inadvertent dosing with catheter in situ | - | 26-30 hours before removal OR check anti-Xa |
3.5.3 Edoxaban (Factor Xa Inhibitor)
| Dose | Hold interval | Restart |
|---|---|---|
| Standard (30-60 mg OD) | 72 hours | 6 hours post-catheter removal |
| Inadvertent dosing with catheter in situ | - | 20-28 hours before removal OR check anti-Xa |
| No low-dose edoxaban guidelines (unlike rivaroxaban/apixaban) | - | - |
3.5.4 Dabigatran (Direct Thrombin Inhibitor)
Renal function is critical as dabigatran is 80% renally cleared.
| CrCl (mL/min) | Hold interval before neuraxial block |
|---|---|
| >80 | 72 hours |
| 50-79 | 96 hours (4 days) |
| 30-49 | 120 hours (5 days) |
| <30 | Neuraxial anesthesia NOT recommended |
| Additional risk factors (age >65, HTN, antiplatelet co-therapy) | Use longer intervals and/or laboratory confirmation |
- Catheter removal: 6 hours before first post-op dose
- Inadvertent dose with catheter in situ: wait 34-36 hours before catheter removal
- Monitoring: TT and dTT (NOT PT, INR, or aPTT - unreliable)
General DOAC principle (4th Edition): In the absence of laboratory testing, 5 half-lives of clearance (97% drug elimination) applies to therapeutic dosing; 2 half-lives applies for prophylactic dosing.
3.6 Antiplatelet Agents
Aspirin and NSAIDs
- Alone: Do NOT increase risk of spinal hematoma in patients with normal coagulation
- Neuraxial block may proceed without interruption if the only antiplatelet agent
- The ASRA guidelines do not mandate discontinuation of aspirin for neuraxial procedures in patients without other coagulopathies
P2Y12 Receptor Antagonists
| Drug | Hold before neuraxial block | Notes |
|---|---|---|
| Clopidogrel | 5-7 days | Most common encountered |
| Prasugrel | 7-10 days | More potent than clopidogrel |
| Ticlopidine | 10 days | Largely replaced; longest hold |
| Ticagrelor | 5-7 days | Reversible; still 5-7 days |
| Cangrelor (IV) | 3 hours | Short half-life (~3-5 min); held 3 h |
Restart after catheter removal: A non-loading dose can be given immediately. If loading dose not given, catheter should only be maintained 1-2 days post-operatively.
GP IIb/IIIa Inhibitors
- Abciximab: 24-48 hours (long recovery of platelet function)
- Eptifibatide / Tirofiban: 4-8 hours
- These agents are contraindicated with neuraxial procedures - if administered, neuraxial catheter management requires immediate consultation
3.7 Fibrinolytic / Thrombolytic Therapy
- Neuraxial block should NOT be performed in patients receiving fibrinolytic or thrombolytic therapy (streptokinase, tPA) except in highly unusual circumstances
- No established safe interval between discontinuation and neuraxial technique
- If accidentally exposed: monitor fibrinogen levels; neurological monitoring every 2 hours
- If epidural catheter was in place when thrombolytics were given (European approach): leave in place until lytic effect fully resolved; use dilute local anesthetic infusion to facilitate neurological monitoring
4. Summary Drug Timing Table
| Drug | Hold BEFORE neuraxial | Catheter REMOVAL interval from last dose | Resume AFTER procedure/removal |
|---|---|---|---|
| Warfarin | 4-5 days, INR ≤1.4 | When INR ≤1.5 | 12-24 hours |
| UFH SC prophylactic BID | 4-6 hours | 4-6 hours | 1 hour after removal |
| UFH SC prophylactic TID | Avoid if possible | - | - |
| UFH IV intraoperative | 1 hour after needle | 2-4 hours | 1 hour after removal |
| UFH IV therapeutic | 4-6 hours, aPTT normal | 2-4 hours | 1 hour after removal |
| LMWH prophylactic | 12 hours | 12 hours | ≥12-24 hours post-op |
| LMWH therapeutic | 24 hours | 24 hours | 4 hours after removal |
| Fondaparinux | 36-42 hours | - | 6-12 hours |
| Rivaroxaban (low) | 24 hours | 6 hours | 6 hours |
| Rivaroxaban (high) | 72 hours | 6 hours | 6 hours |
| Apixaban (low) | 36 hours | 6 hours | 6 hours |
| Apixaban (high) | 72 hours | 6 hours | 6 hours |
| Edoxaban | 72 hours | 6 hours | 6 hours |
| Dabigatran (CrCl >80) | 72 hours | 6 hours | 6 hours |
| Dabigatran (CrCl 50-79) | 96 hours | 6 hours | 6 hours |
| Dabigatran (CrCl 30-49) | 120 hours | 6 hours | 6 hours |
| Clopidogrel | 5-7 days | - | Immediately (non-loading) |
| Prasugrel | 7-10 days | - | Immediately |
| Ticagrelor | 5-7 days | - | Immediately |
| Ticlopidine | 10 days | - | 24 hours |
| Cangrelor (IV) | 3 hours | - | Immediately |
| Abciximab | 24-48 hours | - | - |
| Eptifibatide/tirofiban | 4-8 hours | - | - |
5. Obstetric Patients - Special Considerations
The obstetric population presents unique challenges because anticoagulation decisions are time-sensitive and labor cannot always be delayed.
ASRA + SOAP (Society for Obstetric Anesthesia and Perinatology) Consensus Statement key points:
- Low-dose prophylactic SC UFH (5,000 units BID): neuraxial block is acceptable; check for prolonged aPTT if >5 days of therapy
- Intermediate-dose UFH (e.g., 7,500-10,000 units BID): a 12-hour hold and normal aPTT before neuraxial block
- High-dose/therapeutic UFH (>10,000 U/dose or >20,000 U/day): 24-hour hold and documented normal aPTT
- Prophylactic LMWH: minimum 12 hours before neuraxial (same as general population)
- Therapeutic LMWH (twice-daily therapeutic dosing): 24 hours before neuraxial
- Decision trees (SOAP flowcharts) are incorporated into many obstetric anesthesia protocols globally
6. Deep vs. Superficial Peripheral Nerve Blocks
One of the most practically important clarifications in recent ASRA guidelines:
- Deep, non-compressible blocks (lumbar plexus/psoas compartment, paravertebral, deep cervical plexus, celiac plexus): managed as if neuraxial - same time intervals apply
- Superficial/compressible blocks (interscalene, supraclavicular, axillary, TAP, femoral, popliteal): clinical discretion applies; lower risk but still requires individualized assessment
- The vascularity and compressibility of the anatomical site dictate risk more than the block name
Evidence base: Ultrasound guidance reduces but does not eliminate vascular puncture risk; even with US, time intervals for deep blocks remain mandatory.
7. Local Anesthetic Systemic Toxicity (LAST) - ASRA Practice Advisory
The ASRA Practice Advisory on LAST (2012, updated 2017) is the other major pillar alongside anticoagulation guidelines.
7.1 Risk Factors for LAST
- Extremes of age (infants, elderly)
- Low lean body mass
- Pre-existing cardiac or liver disease
- High block site vascularity (intercostal > caudal > epidural > brachial plexus > sciatic/femoral)
- Intravenous injection (most common cause)
7.2 Clinical Presentation
CNS toxicity (appears first at lower plasma levels):
- Early: metallic taste, circumoral numbness, tinnitus, lightheadedness, visual disturbance
- Moderate: muscle twitching, altered mental status
- Severe: seizures, loss of consciousness, coma
Cardiovascular toxicity (at higher plasma levels):
- Conduction delays (widened QRS)
- Ventricular dysrhythmias (VF is classic with bupivacaine)
- Cardiovascular collapse
CRITICAL: The biphasic presentation may be absent - especially with large IV boluses, cardiovascular collapse can occur without preceding CNS warning signs.
7.3 ASRA LAST Treatment Algorithm (Step-by-Step)
Step 1 - Get help immediately
- Call for help; note the time; don't leave the patient
Step 2 - Airway management
- 100% oxygen; early intubation if needed
- Avoid hyperventilation (hypercarbia worsens toxicity; however, acidosis also worsens it - maintain normal pH)
Step 3 - Treat seizures
- Benzodiazepines are first-line (midazolam, lorazepam)
- Avoid propofol in large doses (cardiac depressant; small doses acceptable)
- Succinylcholine for status epilepticus (to facilitate intubation, not an anticonvulsant)
Step 4 - Cardiovascular management (ACLS with modifications)
- Epinephrine: limit to <1 mcg/kg (smaller than ACLS doses - to avoid triggering malignant arrhythmia)
- AVOID: vasopressin, calcium channel blockers, beta blockers, lidocaine for arrhythmias, other sodium/calcium channel blockers
- Amiodarone is acceptable for ventricular arrhythmias
- If refractory VF: initiate cardiopulmonary bypass preparations
Step 5 - Lipid Emulsion Therapy (20% Intralipid)
| Administration | Dose |
|---|---|
| Bolus | 1.5 mL/kg ideal body weight over 1 minute |
| Infusion | 0.25 mL/kg/min; can double to 0.5 mL/kg/min if no improvement |
| Maximum | ~10 mL/kg over first 30 minutes; can repeat bolus once if no response |
| Duration | Continue infusion for at least 10 minutes after cardiovascular stability |
- Timing: Start at the first sign of dysrhythmia - do not wait for cardiovascular collapse
- Mechanism: "lipid sink" hypothesis + direct cardiotonic effect
- Lipid emulsion works for all lipid-soluble local anesthetics (bupivacaine, ropivacaine, lidocaine)
Post-event: Report to lipidrescue.org; observe at least 2 hours for recurrence
8. Infection Prevention in Regional Anesthesia - ASRA Practice Advisory
Key recommendations:
- Chlorhexidine in alcohol is the preferred skin antiseptic (superior to povidone-iodine)
- Allow chlorhexidine to fully dry before needle insertion
- Sterile gloves, mask, and aseptic technique for all neuraxial blocks
- Cap and sterile drape for all epidural catheter insertions
- Do not use multidose vials in the procedure area
- Epidural catheters: routine replacement at ≤5 days or per institutional protocol
- Tunnel epidural catheters when duration >3 days (reduces infection risk, especially via caudal route)
- Daily inspection of catheter insertion site
- Epidural abscess signs: back pain + fever + neurologic symptoms = MRI immediately
9. Ultrasound-Guided Regional Anesthesia - ASRA Recommendations
Why ultrasound?
Evidence from large systematic reviews shows US-guided regional anesthesia:
- Improves block success rate
- Decreases time to block onset
- Reduces minimum effective local anesthetic volume
- Reduces vascular puncture and hematoma formation
- Decreases LAST incidence
ASRA Statements on US-Guided Practice:
- US does not eliminate the need for anticoagulation time intervals for deep blocks
- US does lower bleeding risk enough to permit more liberal management of superficial/compressible blocks in anticoagulated patients
- Training and competency standards must be maintained (societies mandate structured training curricula)
- Nerve stimulation remains complementary for some deep blocks; US is primary
Safe US-Guided Regional Techniques:
- Aspiration before injection is mandatory - even with US, vascular puncture can occur
- Incremental injection with dose fractionation (3-5 mL aliquots with aspiration)
- Watch for injectate spread in real time - any resistance or lack of spread is a warning sign
- Avoid intraneural injection - "hydrodissection" appearance vs. nerve swelling
10. Enhanced Recovery After Surgery (ERAS) and Regional Anesthesia
ASRA actively supports integration of regional anesthesia into ERAS protocols. Key synergies:
- Epidural analgesia: reduces ileus after colorectal surgery, decreases pulmonary complications after thoracic surgery, reduces DVT after joint arthroplasty
- Peripheral nerve blocks: reduced opioid consumption, earlier mobilization, reduced PONV
- Rebound pain after block offset: educate patients pre-operatively; bridge with multimodal analgesia (acetaminophen, NSAIDs, gabapentinoids, dexamethasone)
- Adjuvants to prolong nerve block duration:
- Perineural dexamethasone (4-8 mg): extends duration by 6-8 hours, reduces rebound pain
- Perineural dexmedetomidine: similar effect
- Clonidine: mild extension, more hypotension risk
- Liposomal bupivacaine (Exparel): up to 72 hours in some blocks
11. Monitoring After Neuraxial Procedures
ASRA recommends:
- Neurological checks every 2 hours minimum while epidural infusion is running
- Use dilute local anesthetic concentrations (0.0625%-0.125% bupivacaine) to preserve motor function and allow ongoing neurological assessment
- Any new back pain, lower extremity weakness, sensory loss, or bladder/bowel dysfunction after neuraxial block = immediate investigation for epidural hematoma
- MRI is the gold standard diagnostic tool
- If SEH suspected: urgent surgical consultation; decompressive laminectomy within 6-8 hours of onset for best neurological outcome
12. Special Populations
Elderly Patients
- Renal function declines with age - DOAC hold intervals must be extended
- Anticoagulant peak levels may be higher and duration of action prolonged
- Assess CrCl using Cockcroft-Gault with actual (not ideal) body weight
Renal Impairment
- LMWH: use with caution if CrCl <30 mL/min; anti-Xa levels may be needed
- Dabigatran: contraindicated neuraxially if CrCl <30 mL/min
- Fondaparinux: avoid if CrCl <30 mL/min
Pediatric Patients (ASRA/ESRA Joint Advisory)
- Neuraxial and deep peripheral blocks are contraindicated if coagulation tests are abnormal
- LMWH: same half-life principles apply; timing adjusted to weight-based dosing
- Most pediatric blocks performed under general anesthesia (safe and accepted by large databases)
- LAST incidence in infants is higher (0.76:10,000 in PRAN registry) - caution with dosing
- Tunneled catheter preferred if caudal route used for >3 days
Patients with Pre-existing Neurological Disease
- Not an absolute contraindication to neuraxial anesthesia
- Document deficits thoroughly pre-operatively
- Informed consent discussion essential
- "Double-crush" vulnerability: an already-injured nerve may be more susceptible to further injury
13. Key Concepts: ESA vs. ASRA Comparison (For Global Consultants)
| Issue | ASRA | European Society of Anaesthesiology (ESA) |
|---|---|---|
| Warfarin INR threshold | Normal (≤1.4) | ≤1.4-1.5 acceptable |
| Warfarin + indwelling catheter | Not recommended | Not permitted |
| DOAC timing | 5 half-lives (therapeutic), 2 HL (prophylactic) | Generally similar, slightly shorter |
| Aspirin alone | Not a contraindication | Not a contraindication |
| Fondaparinux | Generally avoid | 36 h hold acceptable |
| UFH TID | Recommend against | Caution - some allowance |
14. Decision-Making Framework for the Consulting Anaesthesiologist
When evaluating a patient for regional anesthesia with anticoagulation:
- Identify all anticoagulants and antiplatelet agents - including OTC NSAIDs, herbal supplements (fish oil, ginger, ginkgo, garlic - modest antiplatelet effects)
- Classify the proposed block - high/intermediate/low hemorrhagic risk
- Apply drug-specific ASRA hold intervals accounting for renal function and dose level (high vs. low)
- Obtain relevant labs where indicated: INR (warfarin), aPTT or ACT (heparin), TT/dTT (dabigatran), calibrated anti-Xa (Xa inhibitors)
- Consider the thrombotic risk of holding anticoagulation - consult with prescribing physician; bridge therapy if necessary
- Document the risk-benefit discussion with the patient
- Plan catheter management - schedule removal at appropriate intervals
- Post-procedure monitoring - frequent neurological checks; low-concentration local anesthetic infusion
15. Recent Updates (2022-2025)
Based on the ASRA 2025 updated guidelines and published literature (PMID 41073233, Br J Anaesth 2025):
- Low-dose vs. high-dose DOAC distinction is now explicit - shorter intervals for prophylactic/low-dose regimens
- Calibrated anti-Xa assay and residual DOAC level <30 ng/mL as laboratory "pass" thresholds allow earlier procedures when time intervals are not met
- TT/dTT monitoring for dabigatran reinforced (not PT/INR/aPTT)
- Reversal agents (andexanet alfa, idarucizumab, PCC) are NOT recommended for routine neuraxial procedures - insufficient safety data and risk-benefit unfavorable
- UFH TID (thrice-daily) prophylaxis - recommendation against neuraxial procedures strengthened
- Interventional spine pain procedures follow similar but slightly more conservative intervals (e.g., IV heparin restart 24 hours, not just 1 hour post high-risk procedure)
- Ultrasound guidance recognized as a risk-mitigating tool specifically for superficial/compressible blocks in anticoagulated patients
Summary: The 10 Non-Negotiable Rules from ASRA
- Know your pharmacokinetics - every anticoagulant has a different half-life and clearance pathway
- Adjust for renal function especially with DOACs and LMWH
- Deep blocks = neuraxial rules - the compressibility principle governs risk
- Do not remove catheters while drug is active - apply the same hold intervals to catheter removal as to insertion
- LAST: start lipid emulsion early - at first dysrhythmia, not after cardiovascular collapse
- Aspirin alone is not a contraindication - but combinations of antiplatelet + anticoagulant multiply risk
- Warfarin needs documented normal INR - one dose of warfarin may be acceptable, ongoing therapy is not without INR confirmation
- Thrombotic risk must be balanced against hemorrhagic risk - always consult with the prescribing physician before stopping anticoagulation
- Neurological monitoring after neuraxial blocks is mandatory - especially in anticoagulated patients
- Guidelines are living documents - check ASRA.com for the most current updates before high-risk decisions
- Miller's Anesthesia, 10e (Elsevier, 2020), Chapters 58, 77
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Chapter 45
- Barash's Clinical Anesthesia, 9e, Chapter 22
- Sabiston Textbook of Surgery
- ASRA 4th Edition Guidelines: Horlocker TT et al., Reg Anesth Pain Med, 2018
- ASRA 2025 Update: asra.com
- Suleiman A, Sauer WJ, Eikermann M. DOAC management for neuraxial anaesthesia. Br J Anaesth. 2025 Dec [PMID: 41073233]
This is a shared conversation. Sign in to Orris to start your own chat.