Diaphragmatic hernia general surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diaphragmatic hernia"[MeSH Terms] AND "surgical repair"[MeSH Terms]
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material from multiple authoritative surgical textbooks to compose a thorough answer. Let me compile the complete response.
Diaphragmatic Hernia - General Surgery
A diaphragmatic hernia is the protrusion of abdominal contents into the thoracic cavity through a defect in the diaphragm. There are three main categories: hiatal/paraesophageal, congenital, and traumatic.
Anatomy of the Diaphragm - Sites of Herniation
The diagram below shows the diaphragm viewed from below, with the numbered sites of potential herniation:
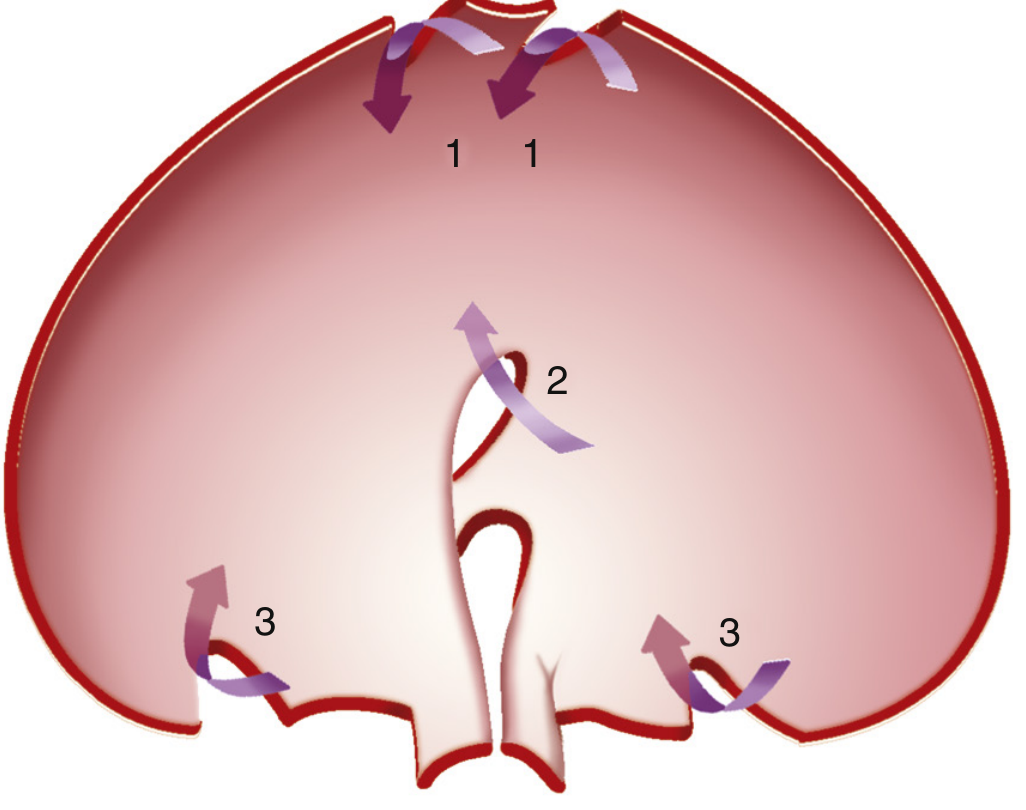
- 1 - Sternocostal foramen of Morgagni (anteriorly)
- 2 - Esophageal hiatus (centrally)
- 3 - Bochdalek foramina (posterolaterally)
1. Hiatal and Paraesophageal Hernias
These are the most common diaphragmatic hernias, all passing through the esophageal hiatus.
Classification
| Type | Name | Description |
|---|---|---|
| Type I | Sliding hiatal hernia | GEJ and portion of stomach displaced above diaphragm; axis unchanged. Most common (~90-95%) |
| Type II | True paraesophageal hernia | Stomach protrudes alongside the esophagus; GEJ remains in normal position |
| Type III | Mixed hernia | Combined sliding + paraesophageal component (most common "paraesophageal" type in practice) |
| Type IV | Complex paraesophageal | Other viscera (omentum, colon, spleen) also herniate through the hiatus |
Etiology and Pathophysiology
- Type I: Age-related deterioration of the phrenoesophageal membrane, combined with positive intra-abdominal pressure and traction from esophageal shortening during swallowing
- Paraesophageal types: Posterior phrenoesophageal ligament preserved in pure Type II (GEJ stays put); entire stomach can herniate in severe cases
Epidemiology
- Prevalence 14-84% depending on population and diagnostic method
- More frequent in GERD patients
- Symptomatic paraesophageal hernias most common in middle-aged to older adults
Clinical Features
- Type I (sliding): Often asymptomatic; main significance is association with GERD. Symptoms: heartburn, regurgitation, dysphagia
- Type II-IV (paraesophageal): Postprandial chest/epigastric pain, dysphagia, early satiety, dyspnoea. Can cause anaemia (Cameron ulcers from mucosal ischaemia at the diaphragmatic ring)
- Complications: Gastric volvulus (organoaxial or mesenteroaxial), incarceration, strangulation, perforation, acute bleeding
Diagnosis
- Barium UGI study: First-line for diagnosing type and anatomy
- CT scan: Preferred for Type IV (reveals colon/pancreas that barium may miss); key questions: Is GEJ above hiatus? Is stomach above GEJ?
- Endoscopy (EGD): Dynamic assessment, retroflex view confirms hernia
Management
Type I (sliding): Treat the underlying GERD medically (PPIs). Surgery only if medically refractory - laparoscopic Nissen fundoplication (360°) or Toupet (270°).
Types II-IV (paraesophageal): Elective surgical repair is indicated for symptomatic patients; emergency repair for volvulus/strangulation.
Surgical principles (laparoscopic approach preferred):
- Reduce herniated contents from chest back into abdomen
- Excise/reduce the hernia sac
- Close the hiatal defect with non-absorbable sutures (cruroplasty); biological mesh reinforcement for large defects
- Fundoplication (Nissen or Dor) to restore LES competence and prevent recurrence
- Gastropexy or gastrostomy tube (as pexy) for 2 weeks to allow stomach to mature to abdominal wall - reduces recurrence
- Collis-Nissen procedure when esophageal shortening is present (a stapler creates a neo-esophagus from proximal stomach, parallel to esophagus over a bougie)
- In obese patients (BMI >35 kg/m²), Roux-en-Y gastric bypass may be favored
Complications of repair: Esophageal/gastric perforation, pneumothorax, liver laceration; long-term: dysphagia (tight wrap), recurrent GERD (fundoplication breakdown), radiographic recurrence 15-25%
2. Congenital Diaphragmatic Hernia (CDH)
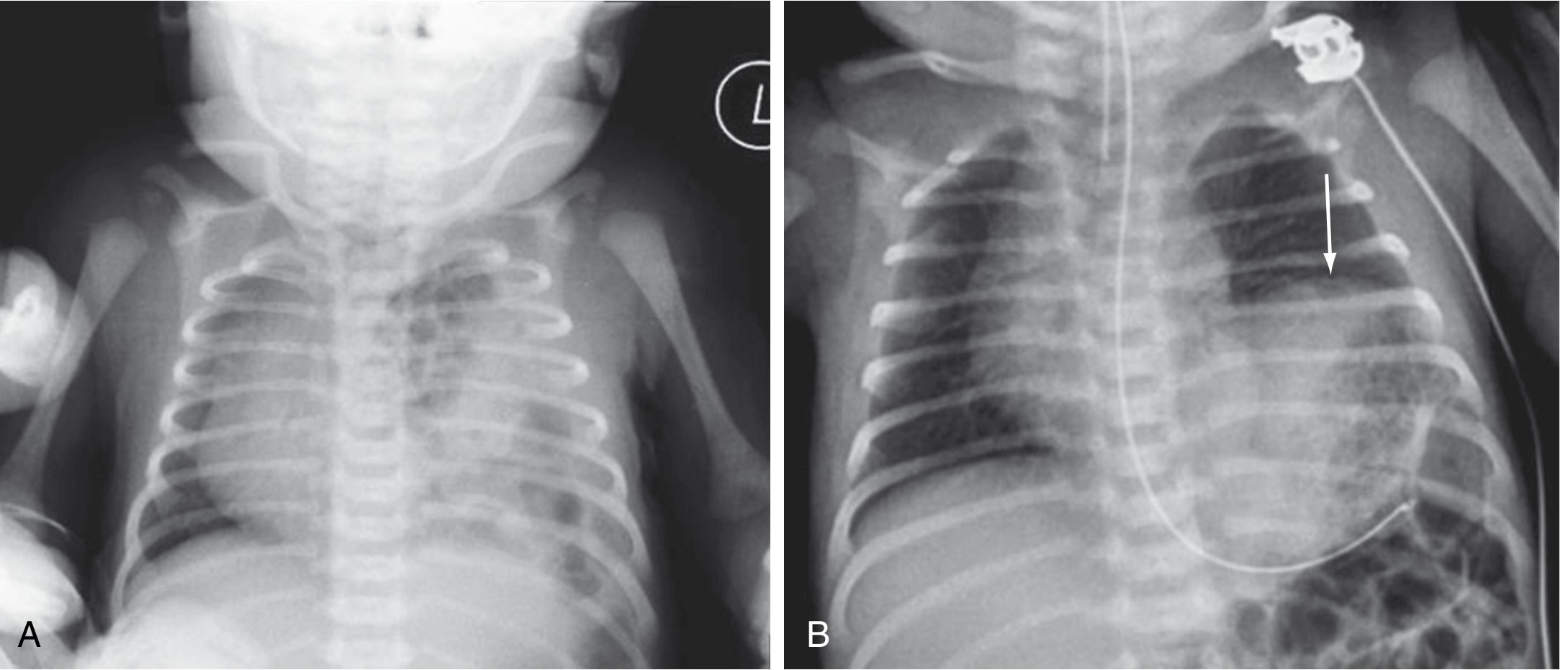
CXR: Left CDH showing multiple gas-filled bowel loops in left hemithorax with mediastinal shift to the right
Pathophysiology
CDH results from failure of fusion of the developmental components of the diaphragm (septum transversum, dorsal mesentery of the esophagus, pleuroperitoneal membranes, muscular ingrowth from body wall). Several genes are shared between diaphragmatic, pulmonary, cardiac, and foregut development (e.g., FOG2, GATA4), hence CDH is associated with:
- Pulmonary hypoplasia (mechanical compression + genetic causes)
- Persistent pulmonary hypertension (PPH)
- Cardiac defects
- Gastroesophageal reflux
- ~50% have additional anomalies
Anatomy
| Type | Location | Frequency |
|---|---|---|
| Bochdalek | Left posterolateral (most common; left in ~75-85%) | ~80-90% |
| Morgagni | Anterior, right-sided cardiophrenic angle | ~5-10% |
| Central/absent diaphragm | Rare | Rare |
Prenatal Diagnosis and Prognosis
- Diagnosed antenatally by ultrasound (hallmark: diaphragmatic defect with bowel in chest)
- Lung-to-head ratio (LHR): contralateral lung area/head circumference
- LHR <1: poor prognosis
- LHR >1.4: nearly 100% survival
- O/E LHR (observed-to-expected LHR): <25% = <20% survival
- Liver position ("liver up" in chest = worse prognosis)
- Total fetal lung volume by MRI is also used
Prenatal Intervention - Fetal Endoscopic Tracheal Occlusion (FETO)
- Tracheal occlusion causes accumulation of fetal lung fluid, stimulating lung growth
- TOTAL trials (randomized): For severe CDH (O/E LHR <25%) - FETO balloon placement at 27-29 weeks significantly improved survival (40% FETO vs. 15% expectant care); study stopped early for efficacy
- For moderate CDH - FETO showed no survival benefit at the tested gestational age
Neonatal Stabilization (Postnatal Management - Pre-repair)
Unlike traumatic hernias, urgently reducing bowel does NOT improve gas exchange in CDH. Stabilization first:
- Immediate intubation and mechanical ventilation (avoid bag-mask ventilation)
- Nasogastric tube decompression
- Gentle ventilation - permissive hypercapnia; goal: pH >7.2, pre-ductal SpO2 85-95%
- High-frequency oscillatory ventilation (HFOV) may help
- Treat pulmonary hypertension: inhaled nitric oxide, prostaglandin E1, milrinone, inotropes
- ECMO/ECLS for refractory cases (severe cardiac dysfunction)
- Repair offered only once pulmonary circulation stabilises
Surgical Repair
- Approach: transabdominal or transthoracic, open or minimally invasive (laparoscopic/thoracoscopic)
- Small defects: closed with non-absorbable sutures (primary closure)
- Large defects: require a conical Silastic or GOR-TEX patch (prosthetic)
- A hernia sac may be present and can be removed or plicated
Prognosis
- Survival has improved to 65-90% with modern management
- Ongoing morbidity: pulmonary hypertension, recurrent GERD, neurodevelopmental issues
3. Traumatic Diaphragmatic Hernia
Epidemiology
- Overall incidence ~0.46% (NTDB data)
- Penetrating trauma accounts for ~67% of injuries
- Blunt trauma (motor vehicle accidents, ~75% of blunt mechanism) causes higher mortality (19.8% vs. 8.8% for penetrating) due to severe associated injuries
- Left hemidiaphragm injured in ~75% of cases - liver protects the right
Mechanism
- Blunt: Rapid increase in intra-abdominal pressure causes a "blow-out" of diaphragmatic tissue
- Penetrating: Direct laceration by missile or knife
Natural History
If untreated: progressive enlargement with herniation of abdominal viscera into the chest; may present months to years after injury as giant diaphragmatic hernia.
AAST Grading
| Grade | Description |
|---|---|
| I | Contusion |
| II | Laceration <2 cm |
| III | Laceration 2-10 cm |
| IV | Laceration >10 cm with tissue loss <25 cm² |
| V | Laceration with tissue loss >25 cm² |
Diagnosis
- Chest X-ray: Intraabdominal viscera in chest (left-sided large defects); elevated or distorted hemidiaphragm; NGT in chest
- CT scan: Sensitivity up to 78%, specificity 72-100%; shows visceral herniation, diaphragm thickening/elevation/defect; still challenging for stab wounds
- Laparoscopy: Recommended diagnostic and therapeutic tool - particularly for penetrating thoracoabdominal trauma (reduces missed injuries vs. CT alone)
- VATS: Alternative for visualizing the diaphragm
Right hemidiaphragm penetrating injuries rarely present in a delayed fashion - may be considered for nonoperative management in stable patients without radiographic signs.
Surgical Repair
- Debride non-viable tissue at the injury site
- Primary closure with single layer of non-absorbable sutures (full-thickness diaphragm) - most defects can be approximated because of diaphragm redundancy/pliability
- Watch for significant bleeding from phrenic artery branches at tear edges
- Large tissue loss with inability to achieve primary closure: prosthetic mesh (non-absorbable synthetic in clean fields; avoid if contaminated)
- Peripheral detachment: re-attach diaphragm to thoracic wall
Summary Comparison Table
| Feature | Congenital (Bochdalek) | Hiatal (Type I-IV) | Traumatic |
|---|---|---|---|
| Age | Neonates | Middle-aged/elderly | Any age |
| Location | Left posterolateral | Esophageal hiatus | Left (75%) |
| Contents | Bowel, spleen, liver | Stomach, viscera | Bowel, spleen, omentum |
| Key finding | Pulmonary hypoplasia + PPH | GERD, volvulus | Viscera in chest post-trauma |
| Diagnosis | Antenatal USS, neonatal CXR | Barium study, CT | CXR, CT, laparoscopy |
| Repair | Delayed (stabilize first) | Elective (urgent if volvulus) | Urgent/semi-urgent |
| Approach | Open/MIS transabdominal | Laparoscopic (preferred) | Laparoscopic/open |
| Patch needed | Large defects | Large hiatal defects | Rare (tissue loss) |
Sources:
- Sabiston Textbook of Surgery, 21st ed. - Diaphragmatic Conditions (Chapter 117), Fetal Surgery (Chapter 118), Diaphragmatic Injuries (Chapter 36)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease - Chapter 27: Diaphragmatic Hernias
- Bailey and Love's Short Practice of Surgery, 28th ed. - Chapter 18
- Fischer's Mastery of Surgery, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.