I ask of microbiology now Explain me in conceptual manner
Asking for Preferences
Classify cestodes. Mention the general features of cestodes. Write in details about morphology, life cycle, pathogenesis and laboratory diagnosis of Echinococcus granulosus (hydatid disease/ hydatid worm).
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed for a comprehensive, well-illustrated answer. Let me compose it.
Cestodes - A Comprehensive Conceptual Guide
CLASSIFICATION OF CESTODES
Cestodes (tapeworms) belong to the phylum Platyhelminthes, class Cestoda. They are classified based on their intestinal vs. tissue-dwelling nature, and by the type of scolex/proglottid:
A. Intestinal Cestodes (adult worm lives in human intestine)
| Species | Common Name | Definitive Host | Intermediate Host |
|---|---|---|---|
| Taenia saginata | Beef tapeworm | Human | Cattle |
| Taenia solium | Pork tapeworm | Human | Pig (also human accidentally) |
| Diphyllobothrium latum | Fish/broad tapeworm | Human | Copepods + freshwater fish |
| Hymenolepis nana | Dwarf tapeworm | Human | Beetles (or direct) |
| Hymenolepis diminuta | Rat tapeworm | Human (accidental) | Beetles |
| Dipylidium caninum | Dog tapeworm | Dog/cat (human accidental) | Fleas |
B. Tissue/Larval Cestodes (larval stage lives in human tissues - humans are intermediate hosts)
| Species | Disease | Definitive Host | Larval Stage |
|---|---|---|---|
| Echinococcus granulosus | Cystic hydatid disease | Dogs/canids | Unilocular hydatid cyst |
| Echinococcus multilocularis | Alveolar hydatid disease | Foxes/canids | Multilocular cyst |
| Taenia solium (eggs) | Cysticercosis / neurocysticercosis | Humans (dead-end host) | Cysticercus cellulosae |
| Taenia multiceps | Coenurosis | Dogs | Coenurus cyst |
| Spirometra spp. | Sparganosis | Cats/dogs | Sparganum (plerocercoid) |
GENERAL FEATURES OF CESTODES
1. Body Plan
Cestodes are segmented flatworms (platyhelminths). The body has three distinct anatomic regions:
- Scolex (head) - the attachment organ; contains suckers, hooklets, or grooves (bothria) depending on the species
- Neck - the mitotically active zone; new proglottids continuously bud off from here (hence the neck is the growth center)
- Strobila (body) - the chain of proglottids (segments) that makes up the bulk of the worm
2. Proglottids
Proglottids are individual "segments" that develop from the neck. Each proglottid passes through stages:
- Immature - newly formed, reproductive organs not yet differentiated
- Mature - contains both male and female reproductive organs (cestodes are hermaphroditic)
- Gravid - uterus is packed with eggs; breaks off and is shed in feces
3. Scolex Anatomy
- Cyclophyllidean tapeworms (Taenia, Echinococcus, Hymenolepis): scolex has 4 sucking disks ± a rostellum (ring of hooklets). Armed = with hooks (e.g. T. solium, Echinococcus); Unarmed = without hooks (e.g. T. saginata)
- Pseudophyllidean tapeworms (Diphyllobothrium): scolex has two elongated sucking grooves (bothria) instead of suckers
4. Key Biological Features
- No digestive tract - cestodes lack a gut entirely. They absorb all nutrients through the tegument (specialized surface layer)
- Hermaphroditic - each mature proglottid contains both male and female reproductive organs; self-fertilization or cross-fertilization can occur
- No circulatory or respiratory system - anaerobic/aerobic energy metabolism through the tegument
- Eggs - typically embryonated, with a hexacanth embryo (oncosphere = 6-hooked larva) enclosed in a thick shell
- Host specificity - the adult tapeworm lives in the definitive host (usually carnivore or human); the larval stage lives in the intermediate host (herbivore or humans in aberrant infections)
- Longevity - adult tapeworms can live for many years in the host intestine
5. Life Cycle Pattern (General)
Egg (in feces) → Ingestion by intermediate host → Oncosphere hatches → Larval stage develops in intermediate host tissues → Ingestion by definitive host → Adult worm in intestine → Eggs passed in feces
ECHINOCOCCUS GRANULOSUS - HYDATID DISEASE
Sources: Medical Microbiology 9e; Sherris & Ryan's Medical Microbiology 8e; Jawetz Melnick & Adelberg's Medical Microbiology 28e
1. MORPHOLOGY
Adult Worm:
- One of the smallest tapeworms known, measuring only 3 to 6 mm in length
- Located in the small intestine of canines (definitive hosts)
- The scolex is Taenia-like with 4 sucking disks and a double row of hooklets (armed)
- The strobila contains only 3 proglottids:
- 1 immature
- 1 mature
- 1 gravid
- Adult worms survive for about 12 months in the canine intestine
Eggs:
- Released when the gravid proglottid splits open, either before or after passage in dog feces
- Morphologically identical to Taenia saginata and T. solium eggs - cannot be distinguished microscopically
- Spherical, thick-walled, embryonated, containing a hexacanth oncosphere
Hydatid Cyst (Larval Stage - in intermediate hosts including humans):
The larval stage is the unilocular hydatid cyst. It is a complex, fluid-filled structure with distinct layers:
| Layer | Name | Function |
|---|---|---|
| Outermost (host-derived) | Pericyst (adventitia) | Fibrous layer formed by host reaction; contains blood vessels and bile ducts |
| Middle | Ectocyst (laminated/cuticle layer) | Thick white, laminated, acellular layer; produced by the parasite |
| Inner | Endocyst (germinal/brood layer) | Single-cell thick; the only living part of the cyst; produces brood capsules, protoscolices, daughter cysts |
Contents of the cyst:
- Brood capsules - arise from the germinal layer; contain developing protoscolices
- Protoscolices - invaginated scolices representing future tapeworm heads (thousands of them)
- Daughter cysts - secondary cysts that arise within or outside the main mother cyst; each has its own germinal layer
- Hydatid sand - sediment of degenerated protoscolices and germinal membranes at the cyst bottom (pathognomonic finding)
- Hydatid fluid - clear, colorless fluid under pressure; highly antigenic and potentially anaphylactogenic
Size: typically ~5 cm diameter, but may reach 10 to 20 cm (containing up to 2 liters of fluid) after years of growth.
2. LIFE CYCLE
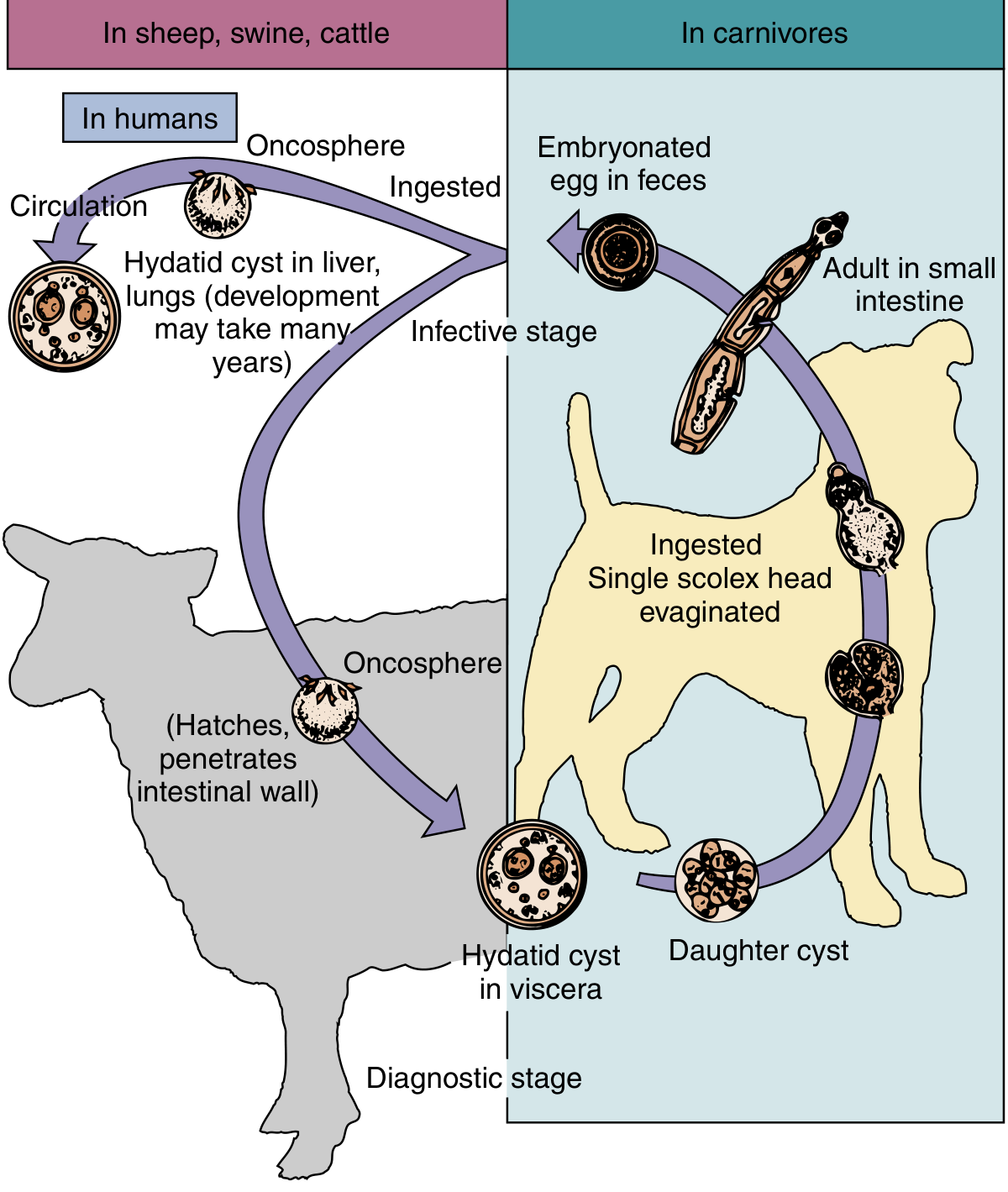
Fig. - Life cycle of Echinococcus granulosus (Medical Microbiology 9e)
Step-by-step:
1. Adult tapeworm in the definitive host (dog)
- Adult E. granulosus lives in the small intestine of dogs (also wolves, foxes, coyotes, jackals)
- Gravid proglottids release eggs that pass out in feces
2. Egg ingestion by intermediate host
- Sheep, cattle, camels, deer, and humans (accidentally) ingest eggs via contaminated vegetation, water, or hand-to-mouth contact with dog feces/fur
- Humans are dead-end intermediate hosts - the cycle cannot naturally complete in humans
3. Oncosphere hatches and migrates
- In the small intestine, the egg hatches releasing the six-hooked oncosphere
- The oncosphere penetrates the intestinal mucosa and enters the portal circulation
- Carried via blood to:
- Liver (most common, ~60-70%) - trapped in hepatic sinusoids
- Lungs (second, ~20-25%) - those passing through the liver
- Brain, heart, bone, kidneys, spleen - rare, via systemic circulation
- Many oncospheres are phagocytosed and destroyed by host immune cells
4. Hydatid cyst formation
- Surviving oncospheres form a cyst wall with:
- External laminated cuticle (ectocyst)
- Internal germinal membrane (endocyst)
- The cyst fills with fluid and slowly expands: ~1 cm in 5-6 months; may take 5 to 20 years to produce symptoms
- Brood capsules arise from the germinal layer → protoscolices develop within
- Daughter cysts form within the mother cyst
- Degenerated material settles as "hydatid sand"
5. Cycle completion in the dog
- When a dog ingests the hydatid-containing tissues of an infected sheep (e.g., farmer feeds raw offal to dogs), the ingested protoscolices evaginate in the dog's intestine
- They attach to the intestinal mucosa and develop into adult tapeworms in 32 to 80 days
- The cycle is maintained by dogs feeding on raw viscera of slaughtered sheep
Epidemiologic forms:
- Pastoral form: sheep-dog cycle; highest incidence in Australia, New Zealand, South America, Middle East, Central Europe, East Africa
- Sylvatic form: wolf/coyote + moose/caribou/deer cycle; found in Alaska, western Canada, California
3. PATHOGENESIS
The pathogenesis of hydatid disease is entirely mechanical - the adult tapeworm causes NO disease in the dog; ALL disease in humans is caused by the larval cyst.
A. Space-occupying effect
The slowly expanding cyst acts like a benign tumor, compressing adjacent tissue:
- Liver (most common site): right lobe most often affected
- Bile duct compression → obstructive jaundice
- Portal vein compression → portal hypertension
- Hepatic parenchymal atrophy and cirrhosis
- Lung: cough, dyspnea, chest pain; cysts visible on chest X-ray as round opacities
- Brain: raised intracranial pressure, seizures, focal neurologic deficits
- Bone: erosion of medullary cavity; pathologic fractures
- Kidney: loin pain, hematuria
B. Cyst rupture (most feared complication)
Rupture occurs in ~20% of cases and may be spontaneous, traumatic, or iatrogenic:
- Allergic/anaphylactic reactions: hydatid fluid is intensely antigenic → urticaria, fever, eosinophilia, and potentially fatal anaphylactic shock
- Secondary seeding (dissemination): spilled protoscolices have germinative potential → can form new hydatid cysts at multiple sites throughout the peritoneum, pleura, or other organs
C. Immunologic responses
- Eosinophilia is common but not always present
- Serum IgE and specific IgG antibodies are elevated
- The cyst wall largely protects the parasite antigens from host immune surveillance during the latent phase
D. Latency
- A latent period of 5 to 20 years (occasionally up to 75 years) is typical between infection and symptoms
- Many cysts are found incidentally on imaging
- Cysts may spontaneously calcify and die over long periods
4. LABORATORY DIAGNOSIS
Diagnosis relies on a combination of imaging, serology, and (rarely) direct identification:
A. Imaging (First Line and Most Important)
- Ultrasound (USG) - method of choice; shows the cyst as a well-defined, echo-free mass with a double-layered wall; may show daughter cysts ("rosette" or "honeycomb" pattern), detached membranes, or hydatid sand settling at the bottom
- CT scan - superior for defining size, location, number of cysts, and calcification; also detects cysts in bone and brain
- X-ray (chest/abdomen) - may show a calcified ring shadow or rounded opacity in liver/lung
- MRI - particularly useful for brain and spinal hydatidosis
B. Serology (Supportive)
- ELISA (Enzyme-Linked Immunosorbent Assay) - most widely used; detects IgG against hydatid cyst fluid antigens; sensitivity ~85-90% for liver cysts
- Immunoelectrophoresis / Arc 5 (Pathognomonic precipitin band) - Arc 5 band against antigen 5 is specific for E. granulosus
- Indirect hemagglutination (IHA) - traditionally used
- Western blot - confirmatory; detects antibody to arc-5 antigen (8/1 kDa bands)
- Limitations: serology is negative in 10% to 40% of cases; less sensitive for pulmonary and calcified cysts; cross-reactivity with other helminth infections
- Seroconversion may occur after cyst rupture (useful indicator)
C. Casoni Skin Test (historical)
- Intradermal injection of sterile hydatid fluid; immediate hypersensitivity reaction = positive
- Poor specificity; largely abandoned in favor of serology
- False-positive in cysticercosis, fascioliasis, and other helminthiases
D. Direct Demonstration (risky - rarely done)
- Aspiration of cyst fluid demonstrates hydatid sand (protoscolices, hooklets, brood capsule fragments)
- Aspiration is generally CONTRAINDICATED due to the risk of anaphylaxis and dissemination
- In modern practice, aspiration is used only therapeutically under the PAIR protocol (Puncture, Aspiration, Injection of scolicidal agent, Re-aspiration), done with full anaphylaxis precautions
- Histopathology of surgically removed cyst: shows the characteristic laminated ectocyst membrane and protoscolices (see image below)
E. Laboratory Tests (non-specific)
- Eosinophilia - present in ~25% of cases; increases markedly after cyst rupture
- Elevated liver enzymes (if hepatic cyst)
- Complete blood count may show leukocytosis after rupture
F. Stool examination - NOT useful. Adults do NOT develop in humans, so no eggs are passed in human feces.
Histopathology Images
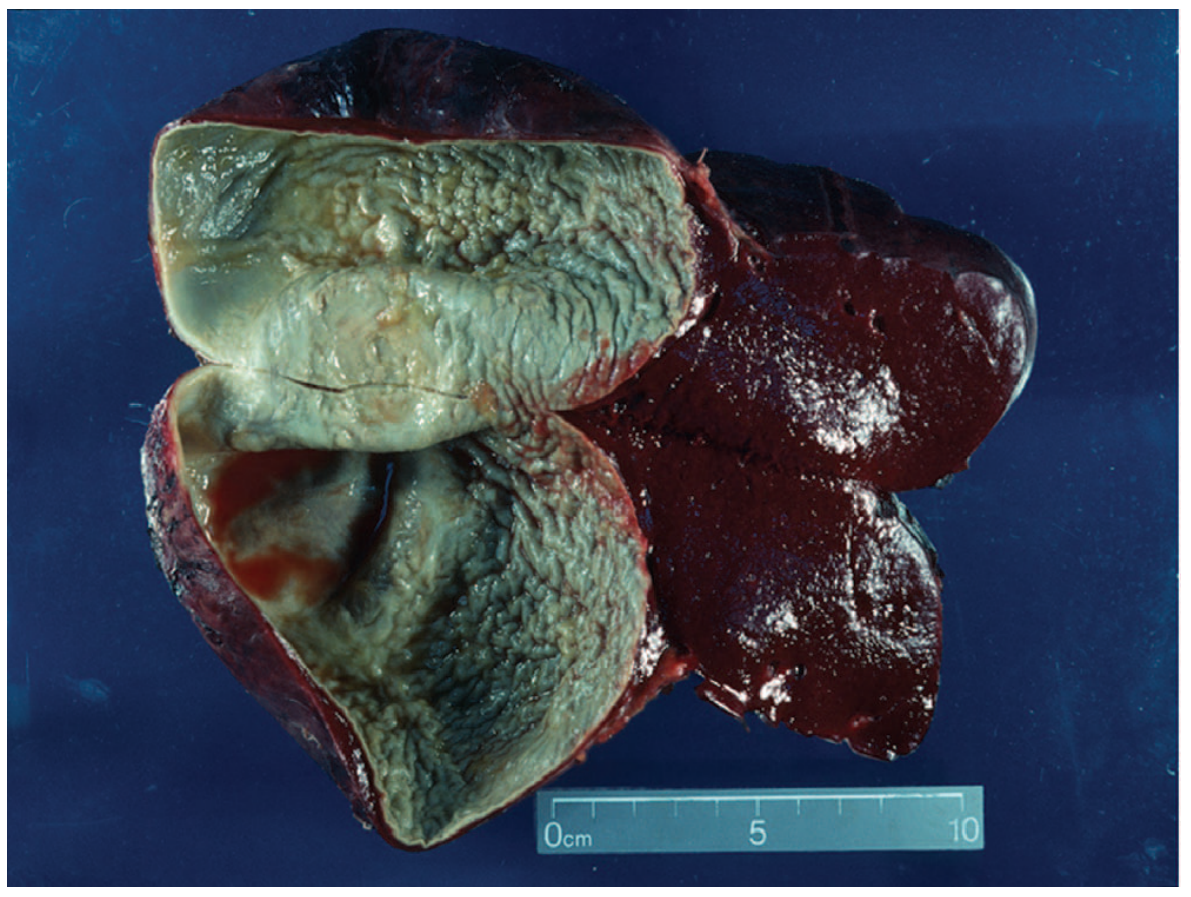
Large hydatid cyst (~14 cm) from spleen showing the characteristic white inner germinal membrane (Jawetz Medical Microbiology 28e)
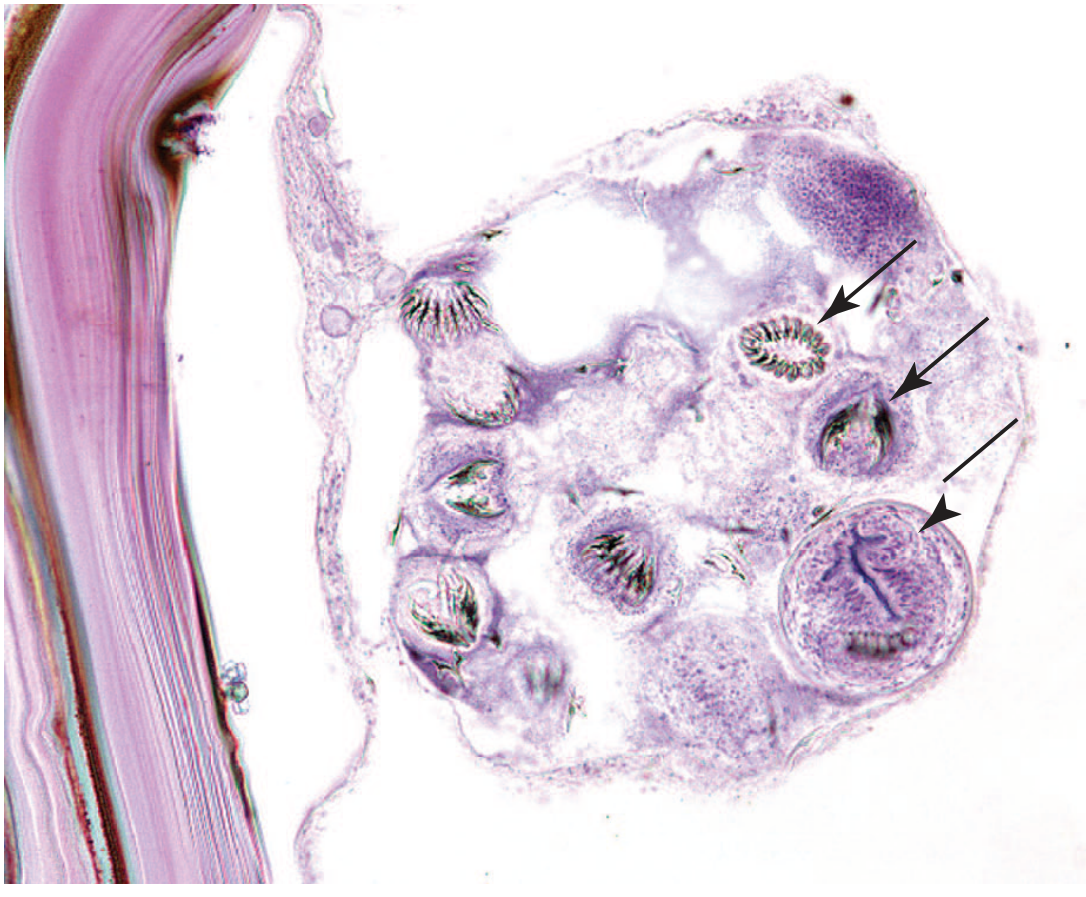
Histologic section: hydatid cyst showing brood capsule with multiple protoscolices (arrows), each with visible rostellar hooklets (Jawetz Medical Microbiology 28e)
Quick Summary Table
| Feature | Detail |
|---|---|
| Organism | Echinococcus granulosus |
| Disease | Cystic echinococcosis / hydatid disease |
| Definitive host | Dog, wolf, fox (canids) |
| Intermediate host | Sheep, cattle, camels, deer; humans (accidental) |
| Infective stage for humans | Embryonated egg |
| Route of infection | Feco-oral (dog feces → human hand/mouth) |
| Site of cyst | Liver (60-70%), Lung (20-25%), others (brain, bone, kidney) |
| Latent period | 5-20 years |
| Pathognomonic finding | Hydatid sand (protoscolices + hooklets in cyst fluid) |
| Best imaging | Ultrasound (first line), CT (most informative) |
| Best serologic test | ELISA + Arc 5 line |
| Contraindicated procedure | Blind cyst aspiration (risk of anaphylaxis + dissemination) |
| Treatment | Surgery (marsupialisation / PAIR); Albendazole for inoperable cases |
Sources: Medical Microbiology 9e (Murray et al.); Sherris & Ryan's Medical Microbiology 8e; Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Tietz Textbook of Laboratory Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.