Pathophysiology of IBD both CD and UC in a single flow chart not a paragraph of every single one of the causes there is. Like a flow chart that covers overall and every important step
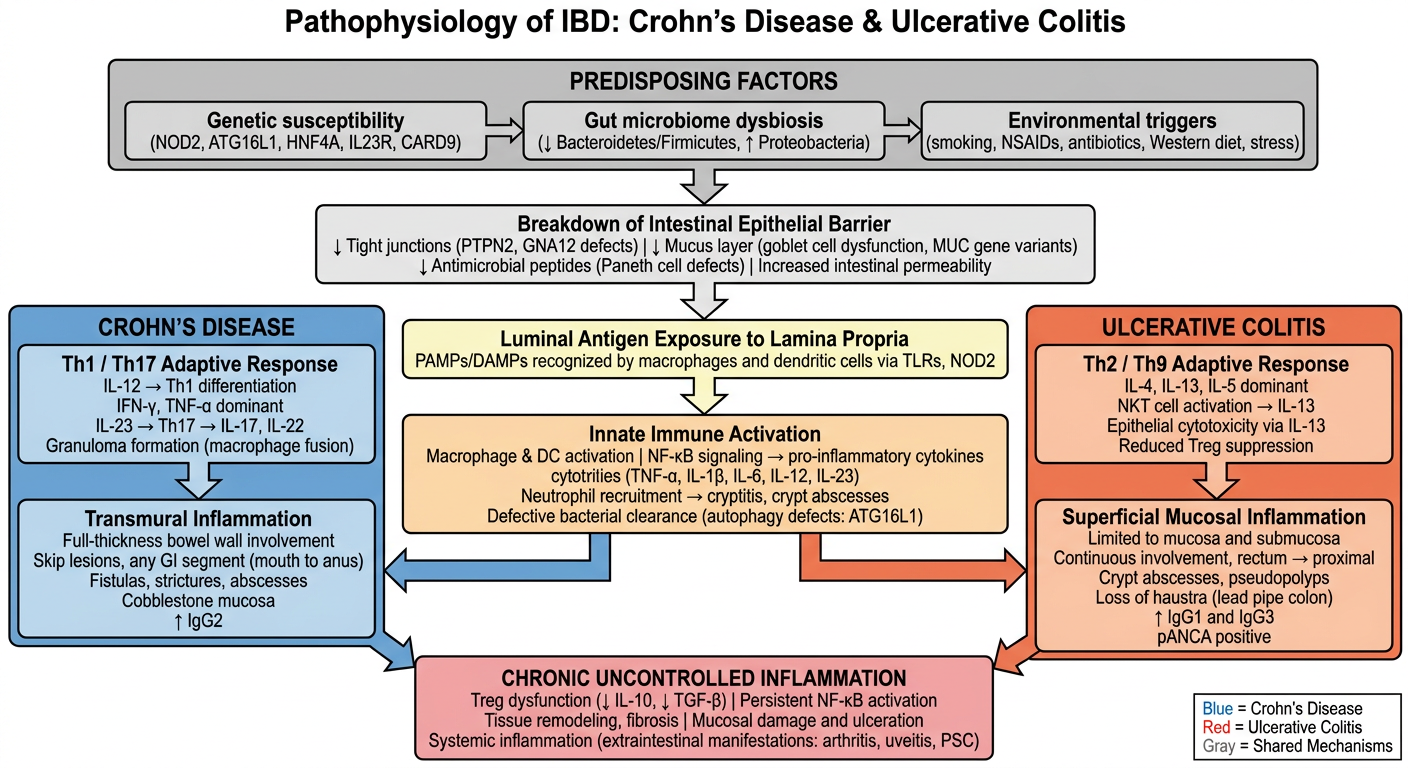
A clean, detailed medical pathophysiology flowchart titled "Pathophysiology of IBD: Crohn's Disease & Ulcerative Colitis" on a white background. The chart flows top to bottom with clearly labeled boxes and arrows. Use a structured layout with two color-coded diverging branches (blue for Crohn's Disease, orange/red for Ulcerative Colitis) and a shared central trunk for common mechanisms. STRUCTURE (top to bottom): TOP LEVEL (shared, gray box): "PREDISPOSING FACTORS" Three boxes side-by-side below it connected by arrows: - "Genetic susceptibility (NOD2, ATG16L1, HNF4A, IL23R, CARD9)" - "Gut microbiome dysbiosis (↓ Bacteroidetes/Firmicutes, ↑ Proteobacteria)" - "Environmental triggers (smoking, NSAIDs, antibiotics, Western diet, stress)" SECOND LEVEL (shared, light gray): Arrow down to: "Breakdown of Intestinal Epithelial Barrier" Sub-bullets inside box: "↓ Tight junctions (PTPN2, GNA12 defects) | ↓ Mucus layer (goblet cell dysfunction, MUC gene variants) | ↓ Antimicrobial peptides (Paneth cell defects) | Increased intestinal permeability" THIRD LEVEL (shared, light yellow): Arrow down to: "Luminal Antigen Exposure to Lamina Propria" Sub-text: "PAMPs/DAMPs recognized by macrophages and dendritic cells via TLRs, NOD2" FOURTH LEVEL (shared, light orange): Arrow down to: "Innate Immune Activation" Sub-bullets: "Macrophage & DC activation | NF-κB signaling → pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-12, IL-23) | Neutrophil recruitment → cryptitis, crypt abscesses | Defective bacterial clearance (autophagy defects: ATG16L1)" FIFTH LEVEL: Arrow down splits into TWO BRANCHES LEFT BRANCH (blue, Crohn's Disease): Title: "CROHN'S DISEASE" Box: "Th1 / Th17 Adaptive Response" Sub-bullets: "IL-12 → Th1 differentiation | IFN-γ, TNF-α dominant | IL-23 → Th17 → IL-17, IL-22 | Granuloma formation (macrophage fusion)" Arrow down to: "Transmural Inflammation" Sub-bullets: "Full-thickness bowel wall involvement | Skip lesions, any GI segment (mouth to anus) | Fistulas, strictures, abscesses | Cobblestone mucosa | ↑ IgG2" RIGHT BRANCH (red/orange, Ulcerative Colitis): Title: "ULCERATIVE COLITIS" Box: "Th2 / Th9 Adaptive Response" Sub-bullets: "IL-4, IL-13, IL-5 dominant | NKT cell activation → IL-13 | Epithelial cytotoxicity via IL-13 | Reduced Treg suppression" Arrow down to: "Superficial Mucosal Inflammation" Sub-bullets: "Limited to mucosa and submucosa | Continuous involvement, rectum → proximal | Crypt abscesses, pseudopolyps | Loss of haustra (lead pipe colon) | ↑ IgG1 and IgG3 | pANCA positive" BOTTOM LEVEL (both branches merge, shared pink/red box): "CHRONIC UNCONTROLLED INFLAMMATION" Sub-bullets: "Treg dysfunction (↓ IL-10, ↓ TGF-β) | Persistent NF-κB activation | Tissue remodeling, fibrosis | Mucosal damage and ulceration | Systemic inflammation (extraintestinal manifestations: arthritis, uveitis, PSC)" Use professional medical diagram style, clear sans-serif fonts, neat arrows, color-coded boxes, and adequate spacing. Include a small legend in the bottom corner: Blue = Crohn's Disease, Red = Ulcerative Colitis, Gray = Shared Mechanisms.
-
Predisposing factors - genetic susceptibility (NOD2, ATG16L1, IL23R), gut microbiome dysbiosis, and environmental triggers all act together.
-
Epithelial barrier breakdown - tight junction defects, goblet cell/mucus layer dysfunction, impaired Paneth cell antimicrobial peptides → increased permeability.
-
Luminal antigen exposure - microbial PAMPs/DAMPs reach the lamina propria and are sensed by macrophages and dendritic cells via TLRs and NOD2.
-
Innate immune activation - NF-κB fires → TNF-α, IL-1β, IL-6, IL-12, IL-23 released; neutrophil recruitment causes cryptitis and crypt abscesses; autophagy defects (ATG16L1) impair bacterial clearance.
| Crohn's Disease | Ulcerative Colitis | |
|---|---|---|
| T-cell skew | Th1 / Th17 (IL-12 → IFN-γ; IL-23 → IL-17) | Th2 / Th9 (IL-4, IL-13, IL-5; NKT → IL-13) |
| Inflammation depth | Transmural, skip lesions, fistulas, granulomas | Mucosal/submucosal, continuous from rectum |
| Key Ig | ↑ IgG2 | ↑ IgG1 and IgG3; pANCA+ |
| Hallmark | Cobblestone mucosa, strictures, abscesses | Crypt abscesses, pseudopolyps, lead-pipe colon |