As m1 receptors present in the brain then when we use the scopalamine it can block the receptors does this produce dementia
Reading File
Finding Sources
Finding Sources
Searching PubMed
scopolamine muscarinic M1 receptor cognitive dementia
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Searching PubMed
anticholinergic drugs dementia risk cognitive impairment
Excellent - I now have all the information needed for a thorough answer. Here is the full synthesis:
Scopolamine, M1 Receptors, and Dementia - A Full Explanation
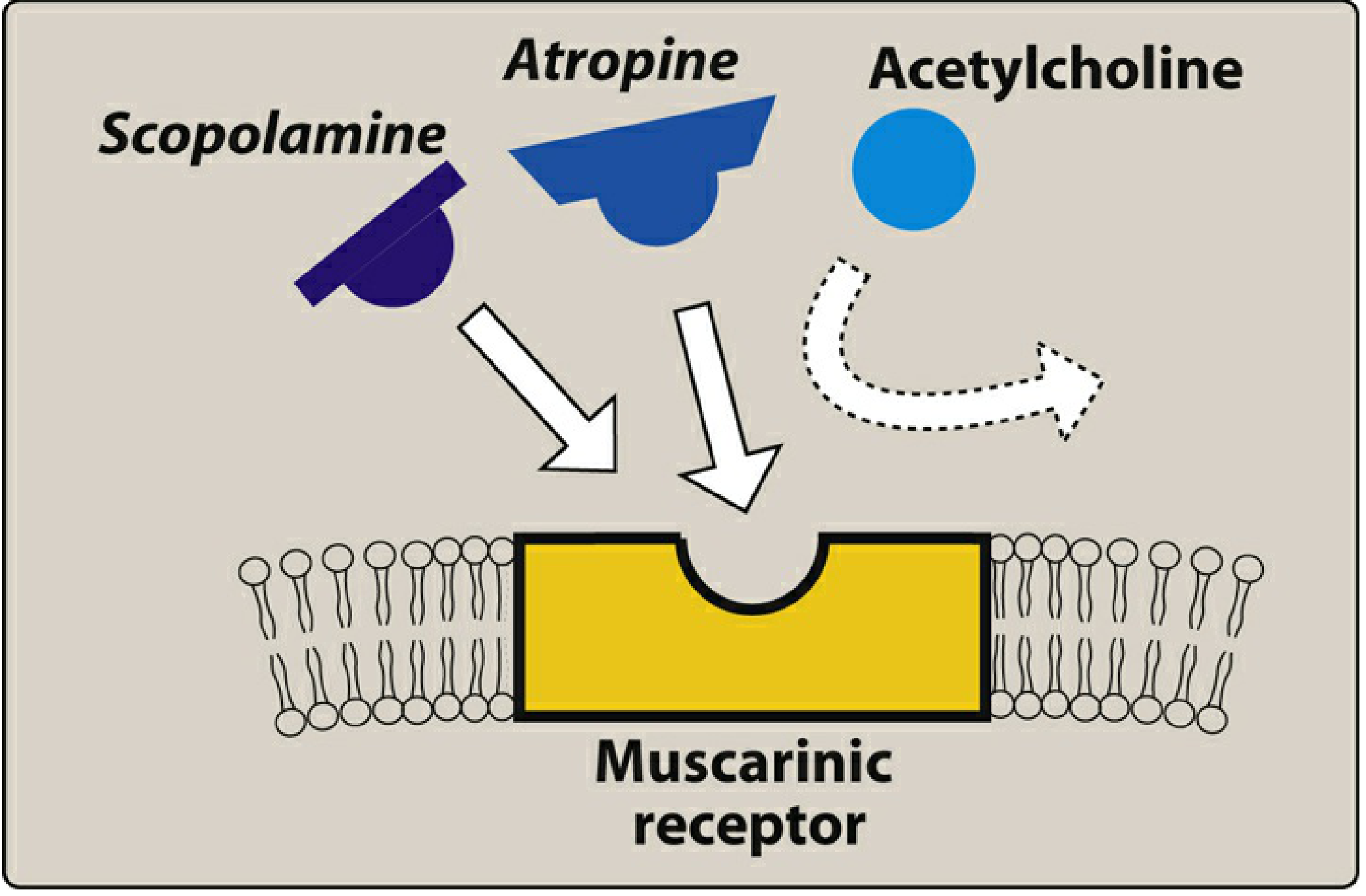
Figure: Scopolamine and atropine block the muscarinic receptor competitively, preventing acetylcholine from binding (Lippincott Pharmacology)
1. What Are M1 Receptors and Where Are They in the Brain?
Muscarinic receptors have five subtypes (M1-M5). M1 receptors are the dominant subtype in the cerebral cortex, hippocampus, and basal ganglia. Their intracellular mechanism works via Gq protein activation → phospholipase C → IP3 + DAG → intracellular Ca2+ release. This signaling pathway is central to memory encoding, attention, and higher cognitive processing.
- Costanzo Physiology, p. 72
2. How Does Scopolamine Work?
Scopolamine (hyoscine) is a belladonna alkaloid - a tertiary amine that readily crosses the blood-brain barrier. It competitively blocks all muscarinic receptor subtypes, but its CNS actions are driven mainly by M1 blockade in the brain.
Its established CNS effects are:
- Sedation
- Amnesia (especially anterograde - blocks new memory formation)
- Euphoria
- Confusion and disorientation (at higher doses)
- Delirium and hallucinations (toxic doses)
Peripheral effects from muscarinic blockade: dry mouth, mydriasis, tachycardia, urinary retention, reduced bowel motility.
- Barash Clinical Anesthesia, p. 947
3. Does It Produce Dementia?
This is where the distinction is important - yes and no, depending on what you mean:
A. Acute/Reversible Cognitive Syndrome (NOT true dementia)
Scopolamine does not cause permanent dementia with a single or short-term use. What it produces is a reversible anticholinergic syndrome - a transient, drug-induced confusional state that mimics dementia:
- Memory impairment
- Disorientation
- Attention deficits
This resolves once the drug is cleared. In fact, the "scopolamine model" is deliberately used in research labs to create a short-lived, reversible dementia-like state in healthy volunteers in order to test new pro-cognitive drugs. It is the classic pharmacological model of cholinergic deficiency.
B. The Cholinergic Hypothesis - Why This Matters
The reason scopolamine mimics dementia symptoms so convincingly is because it reproduces the same neurochemical deficit found in Alzheimer's disease (AD):
"The cholinergic hypothesis of dementia is based on observations of a massive decline of the cholinergic projections from the basal forebrain to the cortex; reductions in choline acetyltransferase activity; marked loss of cholinergic cell bodies in the nucleus basalis... and correlation of the cholinergic deficits with the decline in cognitive test performance."
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 13063
In AD, there is progressive degeneration of cholinergic neurons projecting from the nucleus basalis of Meynert → cortex and hippocampus. Scopolamine pharmacologically mimics this by blocking the remaining cholinergic input. This is why cholinesterase inhibitors (donepezil, rivastigmine, galantamine) are used to treat AD - they increase ACh availability to stimulate whatever M1 receptors remain.
C. Long-Term/Chronic Anticholinergic Use and Dementia Risk
Recent systematic reviews raise a concern about chronic use of anticholinergic drugs contributing to actual dementia risk over years. A 2025 systematic review and meta-analysis (PMID: 41066055) found increased dementia risk with anticholinergics used for overactive bladder. A 2026 systematic review (PMID: 41686541) also found associations between antimuscarinic drugs and cognitive decline. An umbrella review (PMID: 40707785) on systemic medications and dementia risk adds further support. The mechanism proposed is cumulative cholinergic blockade accelerating or unmasking underlying neurodegeneration.
4. Summary Table
| Feature | Scopolamine Effect |
|---|---|
| Receptor blocked | M1 (primarily), all muscarinic subtypes |
| CNS penetration | Yes (tertiary amine, crosses BBB) |
| Acute cognitive effect | Amnesia, confusion, sedation - reversible |
| Mimics | Cholinergic deficiency of Alzheimer's disease |
| Causes permanent dementia? | No with acute use; chronic anticholinergics may increase risk |
| Clinical use of this model | Scopolamine challenge test for pro-cognitive drug research |
Key Takeaway
Scopolamine blocks M1 receptors in the brain and acutely produces a reversible, dementia-like state - but this is not true dementia. It is a pharmacologically induced anticholinergic syndrome. It is clinically important because it demonstrates the role of the cholinergic system in memory and cognition, and directly mirrors the neurochemical basis of Alzheimer's disease. Chronic long-term anticholinergic use, however, may carry genuine dementia risk based on recent evidence.
But the oxybutynin and trospihm also blocking M1 but they r producing dementia
Finding Sources
Finding Sources
Searching PubMed
oxybutynin trospium CNS blood brain barrier cognitive
Reading File
Reading File
Searching PubMed
oxybutynin cognitive impairment dementia elderly anticholinergic
Now I have everything needed for a precise, well-sourced answer.
Oxybutynin vs. Trospium - Why They Differ From Scopolamine Despite All Blocking M1
Your observation is sharp, but the answer lies not in which receptor they block, but whether the drug physically reaches the brain.
The Core Principle: BBB Penetration
All three drugs (scopolamine, oxybutynin, trospium) block muscarinic receptors. But their ability to enter the CNS differs dramatically based on their chemical properties:
| Drug | Chemical Class | BBB Penetration | CNS/Cognitive Effect |
|---|---|---|---|
| Scopolamine | Tertiary amine, lipophilic | High | Strong - amnesia, sedation, delirium |
| Oxybutynin | Tertiary amine, small molecule, lipophilic | High | Significant - cognitive impairment, dementia risk |
| Trospium | Quaternary ammonium compound | Low/minimal | Minimal CNS effect |
| Glycopyrrolate | Quaternary ammonium | Does not cross | No CNS effect |
Oxybutynin - The Problem Drug
Oxybutynin is a tertiary amine with a small molecular size and high lipophilicity - two properties that together make it very good at crossing the blood-brain barrier:
"Oxybutynin in particular, because of its small molecular size and increased propensity to cross the blood-brain barrier, has consistently shown potential to elicit cognitive impairment in new users after a single high dose of this agent or at steady state, and should be avoided in elderly patients."
- Campbell-Walsh-Wein Urology, p. 3524
So oxybutynin does the same thing scopolamine does - it enters the brain and blocks M1 receptors in the cortex and hippocampus - causing:
- Memory impairment
- Confusion / disorientation
- In elderly patients with chronic use: increased risk of dementia
Trospium - Why It Is "Safer" for the Brain
Trospium is a quaternary ammonium compound. Quaternary amines carry a permanent positive charge, which means:
- They are poorly lipid-soluble
- They cannot easily cross the lipid bilayer of the BBB
- They are minimally absorbed from the gut (low bioavailability)
"Quaternary ammonium compounds, like propantheline and trospium, are not well absorbed, pass into the CNS to a limited extent, and have a low incidence of CNS side effects."
- Smith & Tanagho's General Urology, p. 3161
"Trospium chloride, which is a nonselective quaternary amine anti-muscarinic drug, crosses the blood-brain barrier to a limited extent only compared with other antimuscarinics. Clinically, it seems to have good efficacy with no cognitive effect."
- Campbell-Walsh-Wein Urology
So trospium still blocks M1, M2, M3 receptors - but mostly in the bladder and peripheral tissues, NOT in the brain. This is why it causes peripheral side effects (dry mouth, constipation, tachycardia) but spares cognition.
Why Does Chronic Oxybutynin Cause Dementia Risk (Not Just Reversible Confusion)?
This is the important clinical point. Several mechanisms are proposed:
-
Cumulative cholinergic blockade - Long-term blockade of M1 in the cortex and hippocampus may interfere with neuronal maintenance and synaptic plasticity, potentially accelerating neurodegeneration in vulnerable individuals.
-
Anticholinergic burden - Every drug with anticholinergic activity contributes to a cumulative "anticholinergic burden." Higher lifetime burden is associated with dementia risk, even if each individual drug seems mild.
-
Unmasking subclinical disease - In patients who already have early Alzheimer pathology (amyloid plaques, tau, cholinergic neuron loss), blocking residual cholinergic tone can unmask or accelerate clinically apparent dementia.
A 2021 systematic review (PMID: 34213600) confirmed that oxybutynin consistently shows the highest neurocognitive risk among OAB antimuscarinics. A 2024 RCT (PMID: 38402104) directly confirmed oxybutynin 5mg twice daily impairs cognition in elderly patients with mild cognitive impairment.
Clinical Bottom Line
| Situation | Preferred Drug |
|---|---|
| Young patient, no cognitive concern | Oxybutynin acceptable |
| Elderly patient, OAB | Trospium or mirabegron (beta-3 agonist, no anticholinergic effect at all) |
| Patient with existing MCI or dementia | Avoid all antimuscarinics; use mirabegron |
| Surgical premedication/motion sickness | Scopolamine (short-term, reversible effect) |
The real-world advice: the ACB (Anticholinergic Cognitive Burden) scale rates oxybutynin as a high-risk drug (score 3) for cognitive harm in older adults, while trospium carries a lower burden.
Summary: Oxybutynin causes dementia-like cognitive impairment because it crosses the BBB easily (tertiary amine, lipophilic, small). Trospium crosses the BBB minimally because it is a quaternary ammonium compound with permanent charge - so despite blocking M1, it stays mostly outside the brain. The receptor blocked is the same; the difference is where in the body that blockade occurs.
This is a shared conversation. Sign in to Orris to start your own chat.