Positive findings & PG level Physiotherapy assessment for Spinal cord injury & explain anatomy ,types & pathology of disease
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
spinal cord injury physiotherapy assessment positive findings PG level 2024
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Searching PubMed
"spinal cord injury" AND "physiotherapy" AND "assessment"
Loading Image
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK560721
I now have sufficient information from authoritative textbooks and evidence-based sources to deliver a comprehensive PG-level answer. Let me compile it.
Spinal Cord Injury (SCI): Anatomy, Types, Pathology & PG-Level Physiotherapy Assessment
1. ANATOMY OF THE SPINAL CORD
Vertebral Column & Cord Levels
The vertebral column consists of:
- Cervical (C1-C7), Thoracic (T1-T12), Lumbar (L1-L5), Sacrum, Coccyx
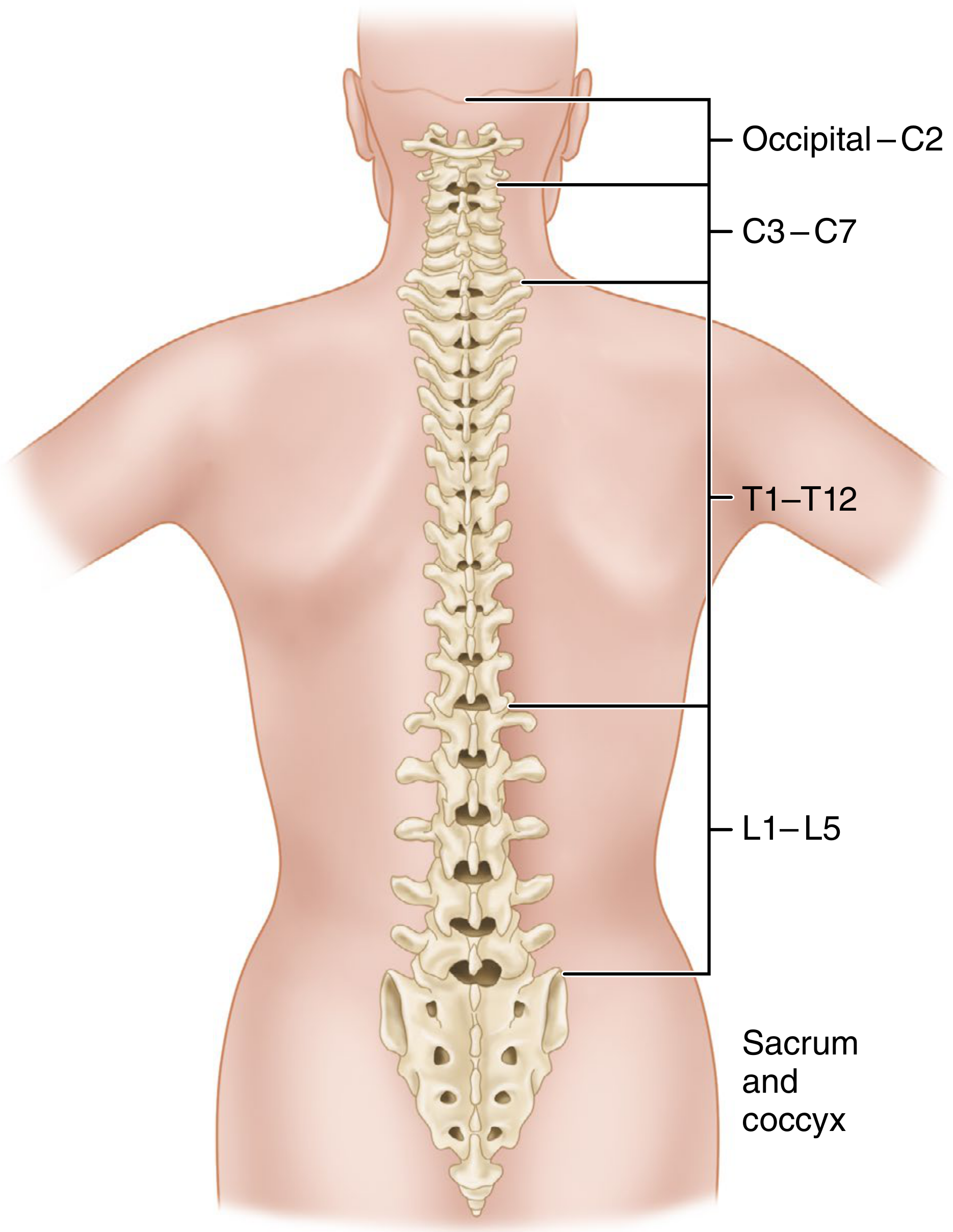
Key anatomical points:
- The spinal cord is shorter than the vertebral column, terminating as the conus medullaris at L2 in adults (L3 in neonates)
- Below the conus, the filum terminale (a fibrous cord) connects the cord to the first coccygeal segment
- The cord is enclosed in three meninges: pia, arachnoid, and dura mater; the subarachnoid space contains CSF
- The cord has cervical and lumbar enlargements corresponding to the brachial plexus and lumbar plexus
- Spinal nerves C2-C7 exit above the named pedicle; C8 and below exit below the named pedicle
Internal Tracts (Cross-Sectional Anatomy)
| Tract | Location | Function |
|---|---|---|
| Dorsal Columns (Fasciculus gracilis/cuneatus) | Posterior | Ipsilateral fine touch, proprioception, vibration |
| Spinothalamic Tract (STT) | Anterolateral | Contralateral pain and temperature |
| Corticospinal Tract (CST) | Lateral (posterior) | Ipsilateral voluntary motor control |
| Anterior CST | Anterior | Ipsilateral proximal motor |
Somatotopic arrangement: Cervical tracts are located centrally; thoracic, lumbar, and sacral tracts are progressively more peripheral. This explains the clinical findings of central cord syndrome and syrinx.
2. TYPES OF SPINAL CORD INJURY
A. Based on Completeness
Complete SCI (ASIA A)
- No motor or sensory function preserved in sacral segments S4-S5
- Complete transection or physiological disruption below the lesion level
Incomplete SCI (ASIA B, C, D)
- Some sensory or motor function is preserved below the neurological level, including in S4-S5
B. Spinal Cord Syndromes (Incomplete Patterns)
| Syndrome | Cord Region Affected | Key Clinical Features |
|---|---|---|
| Central Cord Syndrome | Central gray + central white matter | Upper extremity weakness > lower; bladder dysfunction; cervical hyperextension injury in elderly |
| Anterior Cord Syndrome | Anterior 2/3 (STT + CST) | Loss of motor + pain/temperature below level; dorsal column (proprioception, vibration) PRESERVED |
| Brown-Sequard Syndrome | Hemisection | Ipsilateral motor loss + proprioception loss; contralateral pain + temperature loss |
| Posterior Cord Syndrome | Dorsal columns | Loss of proprioception, vibration, fine touch; motor PRESERVED |
| Conus Medullaris Syndrome | L1-L2 (conus) | Mixed UMN + LMN features; bladder/bowel/sexual dysfunction prominent |
| Cauda Equina Syndrome | Below L2 (nerve roots) | Pure LMN: flaccid paralysis, areflexia, saddle anesthesia, bladder/bowel incontinence |
C. By Level
| Level | Designation | Primary Deficit |
|---|---|---|
| C1-C4 | High Cervical | Quadriplegia, diaphragm paralysis (C4+), ventilator dependent |
| C5-C8 | Low Cervical | Quadriplegia; C5: shoulder abduction; C6: wrist extension; C7: elbow extension |
| T1-T12 | Thoracic | Paraplegia; T1-T6: respiratory impairment; Below T6: trunk control intact |
| L1-L2 | Conus | Mixed UMN/LMN |
| L3-S2 | Cauda equina | Flaccid paraplegia/paresis |
3. PATHOPHYSIOLOGY
Primary Injury
The initial mechanical insult results from:
- Contusion (most common) - vertebral fracture-dislocation
- Laceration / transection - penetrating trauma
- Distraction - flexion-extension
- Compression - burst fractures, disc herniation
Mechanisms produce: direct axonal disruption, neuronal death, hemorrhage into gray matter
Secondary Injury Cascade
This extends damage over hours to days:
| Phase | Mechanism | Timing |
|---|---|---|
| Vascular | Ischemia, microhemorrhage, vasospasm | Minutes-hours |
| Ionic | Na+ influx, Ca2+ overload, K+ efflux | Hours |
| Excitotoxicity | Glutamate release, NMDA receptor activation | Hours |
| Inflammatory | Neutrophils, macrophages, microglia activation | Hours-days |
| Free radicals | Lipid peroxidation, oxidative stress | Days |
| Apoptosis | Programmed cell death in neurons and oligodendrocytes | Days-weeks |
| Cystic cavitation | Glial scar + syrinx formation | Weeks-months |
Increased autophagy activity is detected in neurons, astrocytes, and oligodendrocytes at the lesion zone.
Spinal Shock
- Immediately after SCI: marked reduction in all spinal reflex activity below the lesion
- Results in areflexic acontractile bladder (urinary retention lasting 6-12 weeks in complete SCI)
- Ends when the bulbocavernosus reflex returns
- Below-level reflexes then transition to spasticity (detrusor overactivity, DSD)
4. PG-LEVEL PHYSIOTHERAPY ASSESSMENT
A. Subjective Assessment
History:
- Mechanism of injury (trauma type, direction of force)
- Time since injury, surgical intervention, precautions
- Premorbid functional level and comorbidities
- Presenting complaints: pain, spasticity, pressure areas, bowel/bladder status
- Autonomic symptoms: sweating, flushing, headache (autonomic dysreflexia screening)
- Social history, home environment, prior aids/appliances
B. Objective Assessment - Positive Findings
1. Neurological Level Assessment (ISNCSCI / ASIA)
The International Standards for Neurological Classification of SCI (ISNCSCI) is the gold-standard tool:
Motor Testing - Key Muscle Groups (graded 0-5 MRC scale):
| Level | Key Muscle | Movement |
|---|---|---|
| C5 | Elbow flexors (biceps) | Elbow flexion |
| C6 | Wrist extensors (ECRL) | Wrist extension |
| C7 | Elbow extensors (triceps) | Elbow extension |
| C8 | Finger flexors (FDP, middle finger) | Grip |
| T1 | Finger abductors (DI) | Small finger abduction |
| L2 | Hip flexors (iliopsoas) | Hip flexion |
| L3 | Knee extensors (quadriceps) | Knee extension |
| L4 | Ankle dorsiflexors (tibialis anterior) | Ankle dorsiflexion |
| L5 | Long toe extensors (EHL) | Great toe extension |
| S1 | Ankle plantarflexors (gastrocnemius) | Ankle plantarflexion |
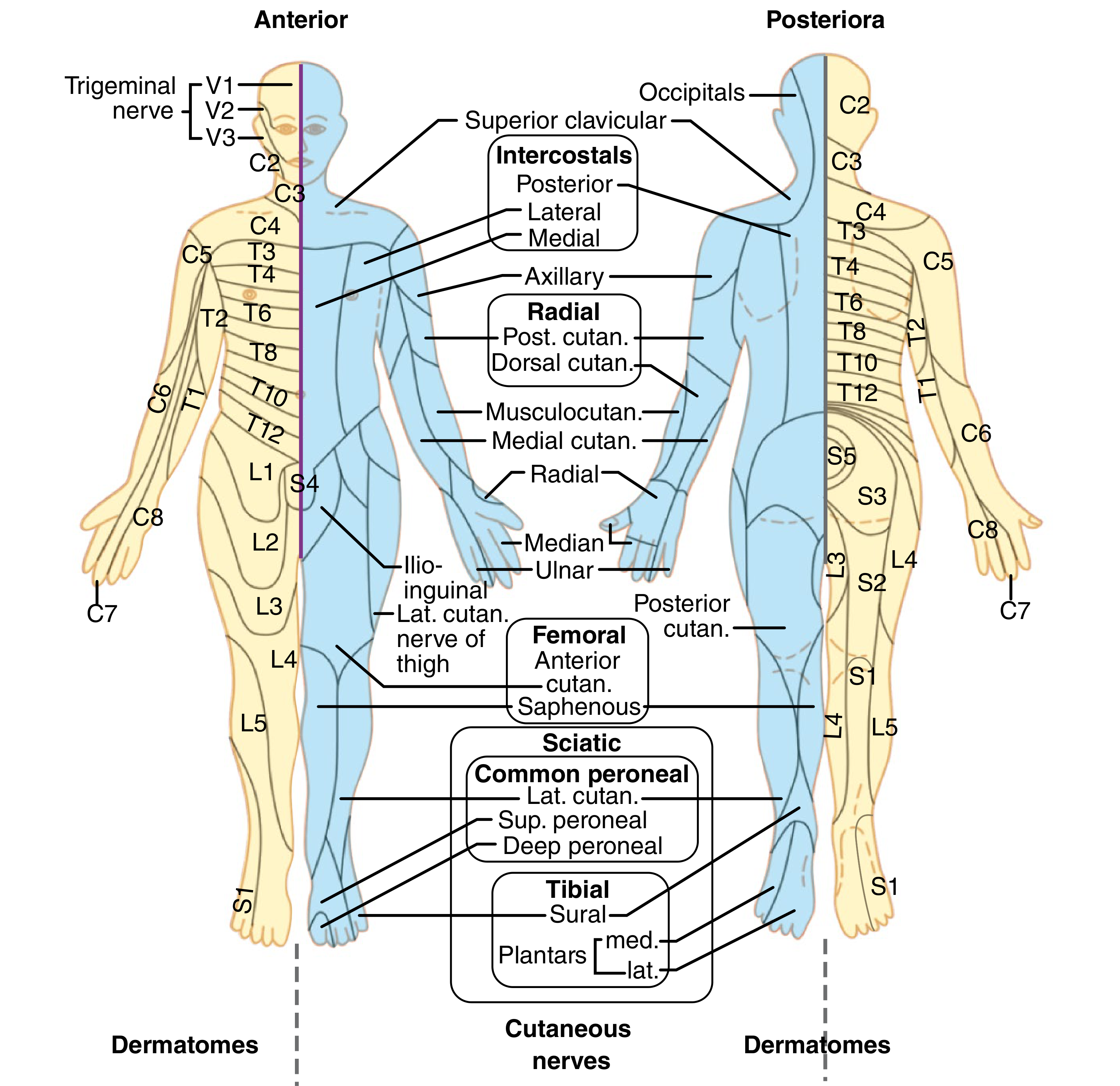
Sensory Testing - Key Dermatomes (light touch + pinprick):
- Tested bilaterally at 28 key points per the ASIA standard form
- Graded: 0 = absent, 1 = altered/impaired, 2 = normal
ASIA Impairment Scale (AIS) Grade:
| Grade | Definition |
|---|---|
| A - Complete | No motor or sensory in S4-S5 |
| B - Sensory Incomplete | Sensory but no motor function below neurological level including S4-S5 |
| C - Motor Incomplete | Motor function below neurological level, majority of key muscles grade < 3 |
| D - Motor Incomplete | Motor function below neurological level, majority of key muscles grade ≥ 3 |
| E - Normal | Motor and sensory normal |
Positive finding: ASIA motor score, sensory score (light touch/pinprick), neurological level of injury (NLI), zone of partial preservation (ZPP)
2. Tone & Spasticity Assessment
Positive signs of spasticity (UAMS SCI Guidelines 2024):
- Clonus (sustained rhythmic contractions)
- Rigidity
- Increased cutaneous and muscle stretch reflexes (hyperreflexia)
- Spasms (flexor/extensor)
- Preserved muscle mass / increased muscle activity
Negative signs (also assessed):
- Weakness, easy fatigability, loss of selective control
Tools used:
- Modified Ashworth Scale (MAS) - grades 0, 1, 1+, 2, 3, 4
- Pendulum Test (Wartenberg pendulum test for lower limbs)
- Spinal Cord Assessment Tool for Spastic Reflexes (SCATS): clonus (0-3), flexor spasms (0-3), extensor spasms (0-3)
- Penn Spasm Frequency Scale
3. Muscle Strength
- MRC grading (0-5) for all accessible muscle groups
- Compare bilateral symmetry
- Document zone of partial preservation (ZPP)
- Note any voluntary anal contraction (sacral sparing)
4. Range of Motion (ROM)
- Passive ROM: all joints, note contractures
- Active ROM: against gravity and resistance
- Joint integrity: subluxation, heterotopic ossification (HO)
- Document capsular tightness, especially shoulder (rotator cuff) in tetraplegics
5. Sensory Assessment
- Superficial sensation: light touch, pain/pinprick, temperature
- Deep sensation: proprioception, kinesthesia, vibration, deep pressure
- Sacral sensation (S4-S5): perineal sensation, voluntary anal contraction
- Map sensory level for dermatomal pattern
6. Reflexes (Positive Findings)
| Reflex | Level | Positive Finding in SCI |
|---|---|---|
| Biceps (C5-C6) | Cervical | Hyperreflexia (above lesion) |
| Triceps (C7) | Cervical | Hyperreflexia |
| Knee jerk (L3-L4) | Lumbar | Hyperreflexia (UMN) or Areflexia (LMN/shock) |
| Ankle jerk (S1-S2) | Sacral | Hyperreflexia or Clonus |
| Babinski's sign | Pyramidal | Positive (extensor plantar response) - pathological |
| Oppenheim's | Pyramidal | Positive in UMN lesion |
| Clonus | UMN | Sustained - positive |
| Bulbocavernosus reflex | S3-S4 | Absent in spinal shock; return = end of shock |
| Anal reflex | S4-S5 | Absent = complete; present = incomplete |
| Cremasteric reflex | L1-L2 | Absent in UMN lesion |
Positive UMN signs (above/at level): spasticity, hyperreflexia, Babinski, clonus, Hoffman's sign (upper limb)
Positive LMN signs (at level/cauda equina): flaccidity, areflexia, atrophy, fasciculations
7. Postural & Balance Assessment
- Sitting balance: static and dynamic (Function in Sitting Test - FIST)
- Standing balance: Berg Balance Scale (BBS), Functional Reach Test (FRT)
- Mini-BESTest (Mini-Balance Evaluation Systems Test)
- Timed Up and Go (TUG) in ambulatory incomplete SCI
- T-Shirt Test for upper limb function
- Note: A 2025 meta-analysis (PMID 39111646) confirmed balance interventions significantly improve upright balance in motor-incomplete SCI (BBS improvement MD = 4.22, 95% CI 1.78-6.66)
8. Functional Assessment
Spinal Cord Independence Measure (SCIM III):
- Self-care: 0-20 points
- Respiration and sphincter management: 0-40 points
- Mobility (room + toilet): 0-40 points
- Total: 0-100 (higher = more independent)
Functional Independence Measure (FIM):
- 18-item scale; motor and cognitive subscales
- 7-point scale (1 = total assist; 7 = complete independence)
Wheelchair Skills Test (WST) - for wheelchair users
9. Respiratory Assessment
- Vital Capacity (VC) and FEV1 - significantly reduced in high cervical/thoracic injuries
- Diaphragm function (C3-C5 via phrenic nerve)
- Accessory muscle recruitment (sternocleidomastoid, scalenes)
- Cough effectiveness (peak cough flow)
- Positive findings: reduced VC, paradoxical breathing pattern, absent cough, SPO2 <95%
- ABG analysis in ventilator-dependent patients (C4 and above)
10. Autonomic Assessment
- Blood pressure: orthostatic hypotension (common at acute stage)
- Autonomic Dysreflexia (AD): lesions at or above T6
- Triggers: bladder distension, pressure sores, constipation
- Positive signs: paroxysmal hypertension (>150 mmHg systolic), bradycardia, flushing/sweating above lesion, pallor/piloerection below lesion, headache
- Emergency: sit upright, remove trigger, sublingual nifedipine if SBP >150 mmHg
- Thermoregulation: poikilothermia below lesion level
- Heart rate variability
11. Skin & Pressure Injury Risk
- Braden Scale / WATERLOW Score for pressure injury risk
- Inspect all bony prominences: sacrum, ischials, greater trochanter, malleoli, heels
- Note skin breakdown, maceration, redness, Stage I-IV pressure injuries
- Assess sensory impairment over pressure areas
12. Pain Assessment
- Neuropathic pain (at-level / below-level): burning, shooting, dysesthetic
- Nociceptive pain: musculoskeletal (shoulder overuse in wheelchair users)
- Numeric Rating Scale (NRS) / Visual Analogue Scale (VAS)
- International SCI Pain Basic Data Set classification
13. Gait & Locomotion (Incomplete SCI)
- 10-Metre Walk Test (10MWT): walking speed
- 6-Minute Walk Test (6MWT): endurance
- Timed Up and Go (TUG)
- Walking Index for SCI (WISCI II): 0-20 scale incorporating use of assistive device, bracing, and physical assistance
- Lower Extremity Motor Score (LEMS): Patients with LEMS ≥ 10 at 1 month become community ambulators; LEMS ≥ 30 allows near-normal walking speed (Bradley and Daroff, cited in Dobkin et al. 2006)
14. Upper Limb Function (Tetraplegia)
- Grasp and release: key pinch, palmar grasp, lateral pinch
- Jebsen-Taylor Hand Function Test
- Graded Redefined Assessment of Strength, Sensibility and Prehension (GRASSP)
- Box and Block Test
- Manual wheelchair propulsion capacity
C. Outcome Measures Summary (PG Level)
| Domain | Tool |
|---|---|
| Neurological classification | ISNCSCI / ASIA |
| Spasticity | MAS, SCATS, Penn Spasm Scale |
| Functional independence | SCIM III, FIM |
| Ambulatory function | WISCI II, 10MWT, 6MWT, TUG |
| Balance | BBS, FIST, Mini-BESTest |
| Pain | NRS, VAS, SCI Pain Basic Data Set |
| Quality of life | SF-36, WHOQOL-BREF |
| Respiratory | Spirometry, Peak Cough Flow |
| Upper limb (tetraplegics) | GRASSP, Jebsen-Taylor |
| Fatigue | FSS-SCI, MFI (2026 Systematic Review, PMID 41047092) |
D. Functional Prognosis (Evidence-Based)
- ASIA A at onset: ~4% recover any walking ability; almost never recover normal bowel/bladder
- ASIA B at onset: ~40% regain walking by 26 weeks
- ASIA C at onset: ~70% recover unlimited walking (Geisler et al., 2001 trial of 760 patients)
- ASIA C - no motor gains by 16 weeks markedly reduces likelihood of useful motor recovery
- With C5 intact: self-feeding possible with assistive devices; power wheelchair with hand control
- With C6 intact: wrist extension allows tenodesis grip; manual wheelchair propulsion, sliding board transfers possible
- With C7 intact: more efficient ADLs, suppository use for bowel program feasible
- Patients with education beyond high school are far more likely to return to work (Bradley and Daroff's Neurology in Clinical Practice)
E. Key Precautions During Assessment
- Maintain spinal precautions until cleared
- Screen for autonomic dysreflexia before any assessment in T6 and above injuries
- Check skin before and after positioning
- Monitor blood pressure for orthostatic hypotension during position changes
- Ensure bowel/bladder has been attended to before assessment (to prevent AD)
- Screen for deep vein thrombosis (DVT) - Homan's sign, limb swelling
5. QUICK REFERENCE: LESION LEVEL vs. EXPECTED FUNCTION
| Level Intact | Expected Function |
|---|---|
| C4 | Diaphragm breathing; power wheelchair (chin/sip-puff control); dependent for all ADLs |
| C5 | Shoulder shrug, elbow flexion; BFO-assisted feeding; power wheelchair |
| C6 | Wrist extension, tenodesis grip; self-catheterization, UE dressing, manual wheelchair |
| C7 | Elbow extension; independent transfers, most ADLs from wheelchair |
| C8-T1 | Finger control; full wheelchair independence |
| T1-T9 | Paraplegia; independent with wheelchair; therapeutic ambulation only |
| T10-L1 | Household ambulator with KAFO and walker |
| L2-S1 | Community ambulator with AFO/crutches |
Sources:
- Campbell's Operative Orthopaedics 15e (2026) - Anatomy of Spinal Cord and Nerves
- Bradley and Daroff's Neurology in Clinical Practice - SCI Rehabilitation, Neurological Level, Prognosis
- Bailey and Love's Short Practice of Surgery 28e - Spinal shock, Autonomic Dysreflexia
- StatPearls - Spinal Cord Injuries (NIH, 2024) - Classification, Pathophysiology, ASIA
- UAMS IDHI SCI Guidelines 2024 - Spasticity Assessment, MAS, SCATS
- Benn et al., 2025 (PMID 39111646) - Meta-analysis: Balance interventions in motor-incomplete SCI
- Lahuerta-Martin et al., 2026 (PMID 41047092) - Fatigue outcome measures in SCI
This is a shared conversation. Sign in to Orris to start your own chat.