Aspermia
Reading File
Finding Sources
Finding Sources
Searching PubMed
aspermia anejaculation treatment
Reading File
Reading File
Searching PubMed
anejaculation aspermia male infertility
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer on aspermia. Let me compile everything.
Aspermia
Definition
Aspermia (also called "dry ejaculate") refers to the complete absence of seminal fluid discharged from the urethra at orgasm - no semen whatsoever. It is distinct from:
- Azoospermia - semen is present but contains no sperm
- Hypospermia - reduced semen volume (< 1.5 mL)
- Retrograde ejaculation - semen goes backward into the bladder
The terms aspermia, dry ejaculate, and anejaculation are sometimes used interchangeably, but strictly speaking anejaculation means no ejaculation at all, while aspermia refers specifically to absent seminal fluid output.
- Campbell Walsh Wein Urology, p. 1868-1869
Pathophysiology
Normal ejaculation requires coordinated action of:
- Emission - seminal vesicles, prostate, and vasa deferentia contract under sympathetic (T10-L2) control, depositing fluid into the posterior urethra
- Ejaculation - rhythmic contractions of the bulbocavernosus and ischiocavernosus muscles expel semen via the urethra
Aspermia results from failure at any level of this process. The seminal vesicles contribute ~80% of ejaculate volume (fructose-rich, viscous fluid), so obstruction or dysfunction of the seminal vesicles or ejaculatory ducts produces absent or near-absent ejaculate.
Causes
1. Ejaculatory Duct Obstruction (EDO)
The most clinically significant organic cause. Can be:
- Congenital - Mullerian duct cysts, wolffian duct abnormalities
- Acquired - prostatitis, STIs (chlamydia, gonorrhea), ductal calculi
Men with bilateral complete obstruction produce no semen at all (aspermia) or very low-volume, low-pH, low-fructose, azoospermic fluid. EDO accounts for 1-5% of male infertility. Orgasm is usually preserved (pelvic floor muscle contractions still occur), and postorgasm pelvic pain is a characteristic feature.
- Campbell Walsh Wein Urology, p. 1733
2. Retrograde Ejaculation (RE)
Semen is redirected into the bladder due to failure of the bladder neck to close. The patient has orgasm but no antegrade ejaculate. Distinguished from true aspermia by finding sperm in post-orgasm urine. Causes include:
- Diabetes mellitus (autonomic neuropathy)
- Spinal cord injury or pelvic surgery (retroperitoneal lymph node dissection, prostatectomy)
- Alpha-blocker drugs (e.g., tamsulosin)
- Transurethral resection of the prostate (TURP)
3. Neurogenic (Failure of Emission)
- Spinal cord injury - ejaculation rates are only 1% with complete upper motor neuron lesions and 15% with complete lower motor neuron lesions
- Sympathectomy, aortoiliac surgery, retroperitoneal dissection
- Multiple sclerosis, diabetic autonomic neuropathy
4. Iatrogenic / Drug-Induced
- SSRIs - up to 60% of patients report ejaculatory dysfunction
- Antipsychotics - dopamine blockade impairs ejaculation
- Alpha-1 adrenergic blockers (tamsulosin) - relax bladder neck, cause retrograde ejaculation or absent emission
- Valganciclovir - may cause hypospermia or aspermia
- Post-radiation therapy (e.g., seminoma treatment)
5. Endocrine Causes
- Hypothyroidism is strongly associated with delayed/absent ejaculation
- Hypogonadism / low testosterone
- Hyperprolactinemia (inhibits GnRH, reduces testosterone, impairs ejaculation)
6. Obstructive / Anatomical
- Congenital bilateral absence of the vas deferens (CBAVD) - seen in cystic fibrosis; nearly all men with CF have absent vas deferens and produce no or minimal ejaculate
- Wolffian duct abnormalities affecting seminal vesicles and ejaculatory ducts
- Genitourinary tuberculosis - calcification and fibrotic obstruction of reproductive tract
- Post-vasectomy (context: aspermia used in post-vasectomy confirmation)
7. Psychogenic
Inhibited male orgasm - psychological inhibition prevents the ejaculatory reflex despite sufficient arousal and intact neurological pathways.
Diagnostic Algorithm
The figure below (from Campbell Walsh Wein Urology) illustrates the office management approach:
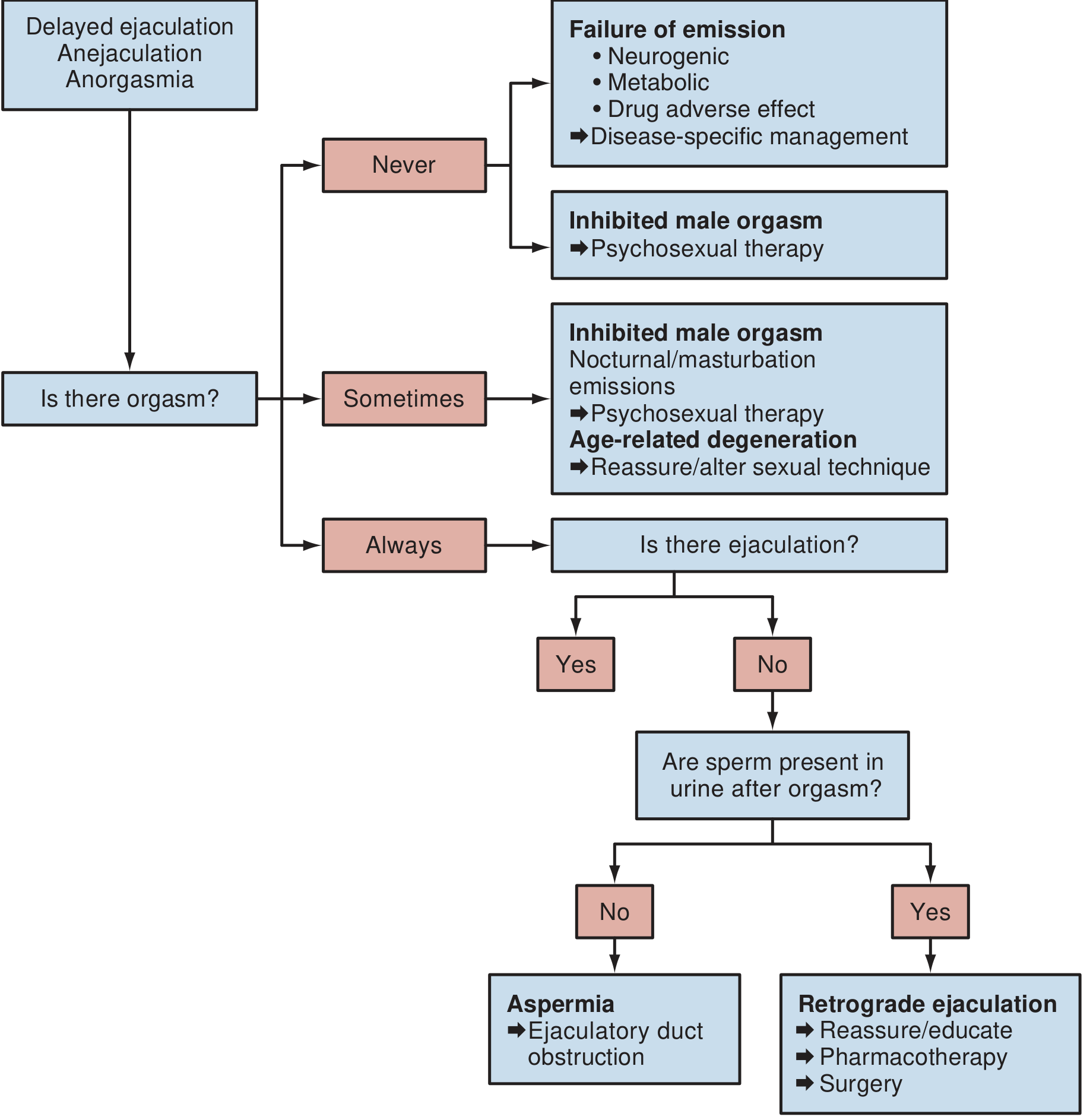
Fig. 71.4 - Algorithm for office management of delayed ejaculation/anejaculation (Campbell Walsh Wein Urology)
Evaluation
History
- Lifelong vs. acquired; global vs. situational
- Presence or absence of orgasm
- Drug history (SSRIs, antipsychotics, alpha-blockers)
- History of pelvic surgery, STIs, radiation, diabetes, spinal injury
- Fertility goals
Physical Examination
- Testicular size and consistency
- Presence of vas deferens (absent in CBAVD/CF)
- Prostate examination
Key Investigations
| Test | Purpose |
|---|---|
| Post-ejaculatory urinalysis | Sperm in urine = retrograde ejaculation |
| Semen analysis | Volume, pH, fructose, viscosity |
| TRUS (transrectal ultrasound) | Evaluate ejaculatory duct obstruction, seminal vesicle dilation |
| MRI pelvis | Better soft-tissue delineation of EDO |
| Serum testosterone, FSH, LH, prolactin | Endocrine workup |
| Serum TSH | Rule out hypothyroidism |
| Cystic fibrosis mutation testing | If CBAVD suspected |
Key diagnostic point: low-volume, low-pH, low-fructose, azoospermic fluid with preserved orgasm = ejaculatory duct obstruction. Sperm in post-masturbation urine = retrograde ejaculation.
- Campbell Walsh Wein Urology, p. 1864
Treatment
Treatment is cause-specific.
1. Ejaculatory Duct Obstruction
- Transurethral resection of ejaculatory ducts (TURED) - surgical unroofing of the ducts; can restore antegrade ejaculation
- Aspiration of seminal vesicle contents under TRUS guidance for sperm retrieval for ART
2. Retrograde Ejaculation
- Pharmacotherapy - sympathomimetics to restore bladder neck closure:
- Pseudoephedrine, ephedrine, imipramine (tricyclic antidepressant with sympathomimetic properties)
- Sperm retrieval from urine - alkalinize urine (NaHCO3), then retrieve sperm post-orgasm for intrauterine insemination (IUI) or IVF
- Surgical: bladder neck reconstruction in selected cases
3. Neurogenic Anejaculation (e.g., Spinal Cord Injury)
- Penile vibratory stimulation (PVS) - first-line; successful in up to 70% of spinal cord injured men (most effective in T10 and above lesions)
- Electroejaculation (EEJ) - electrical stimulation of sympathetic fibers via rectal probe; achieves ejaculation in ~71% of spinal cord injured men
- Both carry risk of autonomic dysreflexia - pretreat with fast-acting vasodilator (e.g., nifedipine) in high-risk lesions
- Collected sperm used for ART (IUI, IVF/ICSI)
- Campbell Walsh Wein Urology, p. 1803-1806
4. Drug-Induced
- Reduce dose or substitute the causative agent where clinically feasible
- Switch SSRI to one with lower ejaculatory side-effect profile (e.g., bupropion)
- Withdraw alpha-blocker if medically appropriate
5. Pharmacotherapy for Delayed Ejaculation / Anejaculation
No drugs are currently approved by regulatory agencies for this indication. Drugs used off-label work through:
| Mechanism | Drug | Dosing |
|---|---|---|
| Dopaminergic | Cabergoline | 0.5 mg daily |
| Antiserotonergic | Cyproheptadine | As needed |
| Adrenergic (peripheral) | Pseudoephedrine, imipramine | As needed |
| Oxytocinergic | Oxytocin | Experimental |
Results are relatively poor in psychogenic and neuropathic DE/anejaculation.
- Campbell Walsh Wein Urology, p. 1888
6. Psychological / Psychosexual Therapy
- Indicated when organic and pharmacologic causes are excluded
- Masturbatory retraining, anxiety reduction, sensate focus techniques
- Goal: incremental arousal through fantasy and self-stimulation before partner involvement
- Reducing "ejaculatory performance anxiety" is a key therapeutic target
7. Assisted Reproduction
When antegrade ejaculation cannot be restored, sperm can still be retrieved for use in ART:
- Sperm from urine (retrograde ejaculation)
- Surgical sperm retrieval - PESA (percutaneous epididymal sperm aspiration), TESA (testicular sperm aspiration), or micro-TESE
- IUI, IVF, ICSI depending on sperm quality
Special Context: Post-Vasectomy Aspermia
In preventive medicine, achieving aspermia (confirmed on semen analysis) is the endpoint of successful vasectomy. Patients are advised to use contraceptives until aspermia is confirmed, which typically requires ~20 ejaculations or 3 months post-procedure.
- Park's Textbook of Preventive and Social Medicine
Summary
| Feature | Detail |
|---|---|
| Definition | Complete absence of seminal fluid at orgasm |
| Key distinction | Check post-orgasm urine: sperm present = retrograde ejaculation; absent = true aspermia/EDO |
| Most common cause | Ejaculatory duct obstruction, retrograde ejaculation, neurogenic |
| Investigation | Post-ejaculatory urinalysis, TRUS, semen analysis, hormones |
| Treatment | Cause-specific: TURED for EDO, sympathomimetics for RE, PVS/EEJ for neurogenic, ART for fertility |
| Fertility outcome | Pregnancy is achievable in most cases via ART even when antegrade ejaculation cannot be restored |
Azoospermia
Finding Sources
Finding Sources
Searching PubMed
azoospermia diagnosis management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Azoospermia
Definition
Azoospermia is the complete absence of spermatozoa in the ejaculate. It is found in ~1% of all men and 15-20% of infertile men, making it one of the most significant causes of male infertility.
- Berek & Novak's Gynecology, p. 2431
Classification
Azoospermia is categorized into three broad groups based on the level of the defect:
| Category | Mechanism | Key Hormonal Pattern |
|---|---|---|
| Pretesticular (Secretory) | Gonadotropin deficiency - no spermatogenesis stimulus | Low LH, FSH, testosterone (hypogonadotropic) |
| Testicular (Secretory / NOA) | Primary testicular/spermatogenic failure | High FSH, high LH, low testosterone (hypergonadotropic) |
| Posttesticular (Obstructive / OA) | Obstruction or dysfunction of the outflow tract | Normal gonadotropins and testosterone |
Posttesticular causes account for up to 40% of azoospermic men.
1. Pretesticular Azoospermia (Hypogonadotropic Hypogonadism)
Relatively rare. Results from gonadotropin deficiency leading to absent spermatogenesis.
Causes
- Congenital: Kallmann syndrome (GnRH deficiency + anosmia), isolated hypogonadotropic hypogonadism
- Acquired: Pituitary adenoma, hyperprolactinemia, hemochromatosis, systemic illness, cranial irradiation
- Iatrogenic (most common today): Exogenous testosterone / anabolic steroid use - suppresses the HPG axis and shuts down endogenous testosterone and FSH, halting spermatogenesis
Key Workup
- Low LH, FSH, testosterone
- Elevated prolactin - consider pituitary MRI
- History of puberty, growth, and anosmia
Treatment
-
Pulsatile GnRH (via pump) - for hypothalamic causes
-
hCG + FSH (exogenous gonadotropins) - for both hypothalamic and pituitary causes; best response predicted by postpubertal onset and testicular volume > 8 mL
-
Testosterone cessation for iatrogenic cases + recovery with clomiphene citrate, hCG, and/or FSH. Sperm typically recovers to a median of 6.5 million/mL about 4.5 months after stopping testosterone; full recovery more likely if testosterone was used < 1 year
-
Berek & Novak's Gynecology, p. 2436
2. Testicular Azoospermia (Non-Obstructive Azoospermia, NOA)
Primary failure of the testes to produce sperm (spermatogenic failure). The most challenging category.
Causes
Genetic:
- Klinefelter syndrome (47,XXY) - most common chromosomal cause; accounts for ~2/3 of infertility-associated chromosomal abnormalities. Men have small, firm testes and hypergonadotropic hypogonadism. Historically thought to preclude biological fatherhood, but rare sperm can be found with micro-TESE.
- Y chromosome microdeletions - found in 10-20% of men with idiopathic NOA or severe oligospermia (< 5 million/mL). Three regions implicated:
- AZFa - complete deletion: Sertoli cell-only syndrome; no sperm retrievable
- AZFb - complete deletion: spermatogenic arrest; no sperm retrievable
- AZFc - most common deletion; contains the DAZ (Deleted in Azoospermia) gene; sperm retrieval often possible with IVF/ICSI
Detected by PCR of peripheral blood leukocytes using sequence-tagged sites (sY84, sY86 for AZFa; sY127, sY134 for AZFb; sY254, sY255 for AZFc).
- Harrison's Principles of Internal Medicine, p. 2713
- Smith & Tanagho's General Urology, p. 4093
Acquired:
- Mumps orchitis (bilateral) - post-pubertal infection causes testicular atrophy
- Testicular torsion (bilateral or recurrent)
- Radiation therapy, chemotherapy (alkylating agents are most gonadotoxic)
- Cryptorchidism (undescended testis)
- Varicocele
Developmental:
- Testicular maldescent / dysgenesis
Biopsy Histological Patterns in NOA
-
Hypospermatogenesis - all stages present but reduced in number
-
Maturation arrest - usually at primary spermatocyte stage
-
Sertoli cell-only syndrome (SCO) - absent germ cells, tubules lined only by Sertoli cells
-
Hyalinization / tubular sclerosis - end-stage, absent cellular elements
-
Harrison's Principles of Internal Medicine, p. 2708
Note on Testicular Biopsy in NOA
Biopsy is generally not recommended when hypergonadotropic hypogonadism (high FSH/LH + low testosterone) is already established - sperm retrieval is unlikely and donor sperm may be counseled. However, even men with markedly elevated FSH and small soft testes sometimes harbor rare mature sperm discoverable on micro-TESE. Diagnostic biopsy may be indicated when hormones are normal to differentiate NOA from obstructive azoospermia.
- Campbell Walsh Wein Urology, p. 2991
3. Posttesticular Azoospermia (Obstructive Azoospermia, OA)
Spermatogenesis is normal but outflow is blocked. Characterized by normal FSH, normal testosterone, normal testicular size.
Causes
| Site of Obstruction | Cause |
|---|---|
| Vas deferens | Vasectomy (most common in developed world), CBAVD, post-hernia repair injury |
| Epididymis | Post-infective (gonorrhea, chlamydia), Young syndrome, idiopathic |
| Ejaculatory duct | Congenital (Mullerian duct cysts), acquired (prostatitis, STIs, calculi) |
| Seminal vesicles | Agenesis (associated with CBAVD/CF) |
Congenital Bilateral Absence of Vas Deferens (CBAVD):
-
Present in virtually all men with cystic fibrosis
-
At least two-thirds of isolated CBAVD cases harbor mutations of the CFTR gene
-
Spermatogenesis is normal (biopsy not routinely needed)
-
Low semen volume, low pH, absent fructose (due to seminal vesicle agenesis)
-
Female partner must be tested for CFTR carrier status before any ART
-
Associated with 10-25% incidence of renal agenesis - renal imaging required
-
Berek & Novak's Gynecology, p. 2467
Diagnostic Evaluation
Step 1: Confirm Azoospermia
- Two separate semen analyses with centrifugation to search for rare sperm (cryptozoospermia)
- Abstinence 2-3 days before collection; analysis within 1 hour
- WHO 2010 lower reference limit: sperm concentration 15 million/mL; azoospermia = zero
Step 2: Initial Investigations
| Investigation | Purpose |
|---|---|
| Serum FSH, LH, testosterone | Distinguish NOA (high FSH) from OA (normal FSH) |
| Serum prolactin | Rule out hyperprolactinemia |
| TSH | Rule out hypothyroidism |
| Peripheral karyotype | Detect Klinefelter (47,XXY) and other aneuploidies |
| Y chromosome microdeletion testing | In idiopathic NOA or severe oligospermia (PCR-based blood test) |
| CFTR mutation testing | If CBAVD suspected (absent vas deferens on examination) |
| Post-ejaculatory urinalysis | Low-volume azoospermia - rule out retrograde ejaculation |
| TRUS / scrotal ultrasound | Ejaculatory duct obstruction, seminal vesicle agenesis |
Step 3: Testicular Biopsy / Sperm Retrieval
Indicated in azoospermic men with:
- Normal testis size and consistency
- Palpable vas deferens
- Normal FSH
Under these conditions, biopsy distinguishes OA from NOA and can retrieve sperm for ICSI simultaneously.
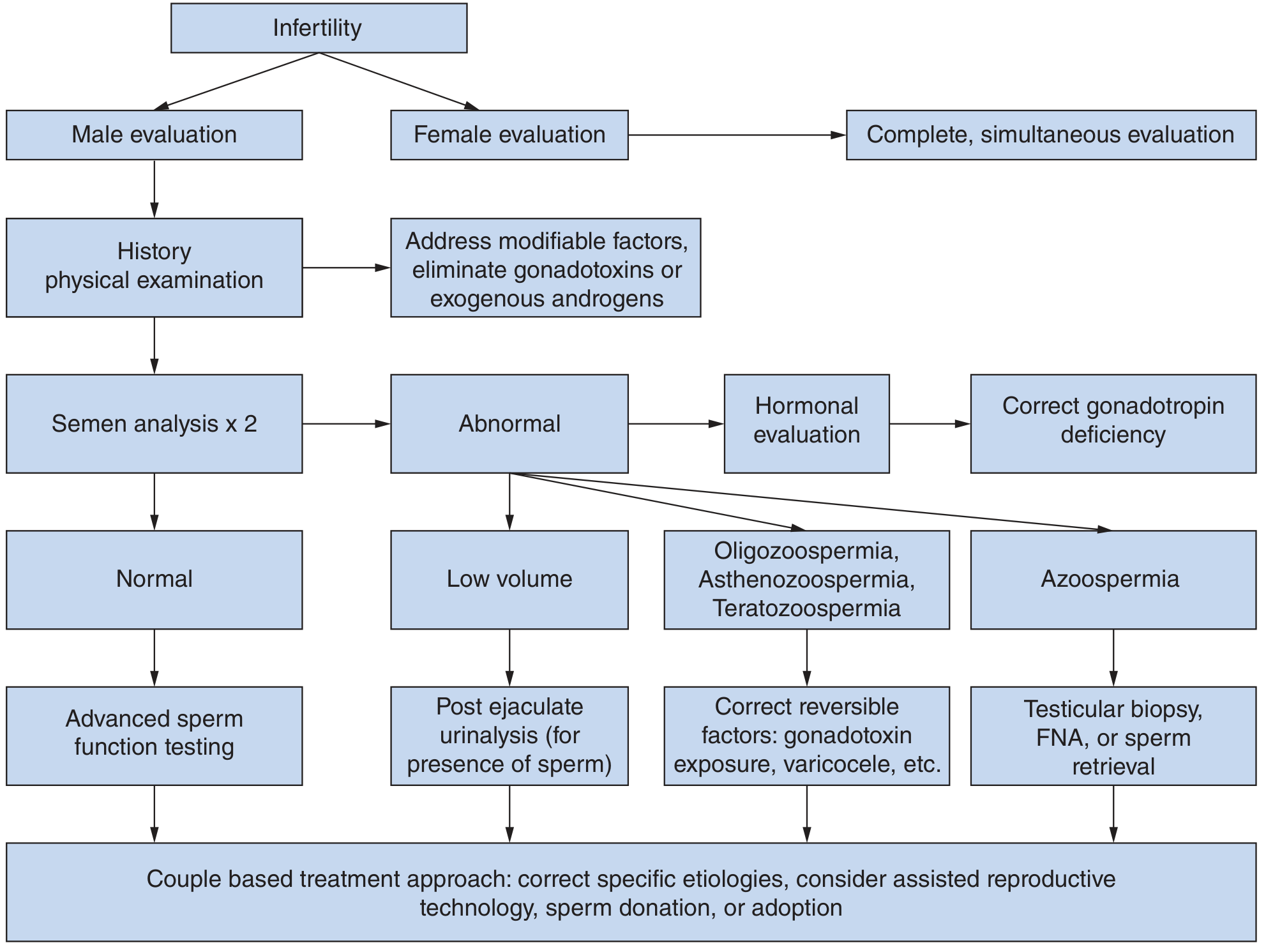
The diagnostic algorithm from Smith & Tanagho:
Treatment
A. Pretesticular (Hormonal / Reversible)
- Gonadotropin therapy (hCG ± FSH/recombinant FSH) for hypogonadotropic hypogonadism
- Pulsatile GnRH for hypothalamic defects
- Cessation of exogenous androgens + recovery agents (clomiphene, hCG, FSH) for iatrogenic suppression
- Treat hyperprolactinemia (dopamine agonists: cabergoline, bromocriptine)
- Treat hypothyroidism (levothyroxine)
B. Obstructive Azoospermia (Surgical Reconstruction)
Vasectomy Reversal:
-
Vasovasostomy - end-to-end anastomosis of the vas; patency rates approach 100%, pregnancy rates ~80%
-
Vasoepididymostomy - when epididymal obstruction is present (proximal to anastomosis)
-
Success decreases with increasing time since vasectomy, especially > 15 years
-
~60% develop antisperm antibodies post-reversal but this does not significantly affect fecundability
-
If azoospermia persists 6 months post-reversal - repeat procedure (75% patency, 43% pregnancy) or proceed to TESE + ICSI
-
Berek & Novak's Gynecology, p. 2472
Transurethral Resection of Ejaculatory Ducts (TURED): for ejaculatory duct obstruction
C. Non-Obstructive Azoospermia (Sperm Retrieval + ART)
When spermatogenesis cannot be restored medically, sperm can still sometimes be retrieved directly from the testis:
| Technique | Description | Anesthesia |
|---|---|---|
| Micro-TESE (microdissection TESE) | Operating microscope to identify dilated tubules with active spermatogenesis; highest yield in NOA | General / spinal |
| TESE (conventional) | Multiple open biopsies of testis | General / spinal |
| MESA (microsurgical epididymal sperm aspiration) | Best for OA; highest quality motile sperm | General / regional |
| PESA (percutaneous epididymal sperm aspiration) | Needle aspiration of epididymis; OA only | Local |
| TESA / FNA (fine-needle aspiration) | Percutaneous testicular needle aspiration | Local |
Retrieved sperm are used with ICSI (intracytoplasmic sperm injection) - even a single viable sperm can achieve fertilization.
- Testicular atrophy is a rare complication of TESE/TESA
Varicocele repair: In NOA with varicocele, repair may restore sperm to the ejaculate and permit natural pregnancy or IUI/IVF-ICSI.
D. Donor Sperm / Adoption
Considered when:
- Hypergonadotropic hypogonadism with complete testicular failure (SCO, AZFa/AZFb deletions)
- Sperm retrieval fails
- Genetic conditions the couple does not wish to transmit
Genetic Counseling Points
- Chromosomal abnormalities in azoospermic men: ~10-15%
- Y chromosome microdeletions (especially AZFc) are transmitted to male offspring who will also be infertile - genetic counseling before ICSI is mandatory
- CBAVD: female partner must be tested for CFTR carrier status; if carrier, 1 in 2 male children may have CF
- Klinefelter: mosaic (46XY/47XXY) men more likely to have sperm than non-mosaic; ICSI offspring should be tested prenatally or by PGT
Key Distinguishing Features: OA vs NOA
| Feature | Obstructive (OA) | Non-Obstructive (NOA) |
|---|---|---|
| FSH | Normal | Elevated (usually) |
| Testis size | Normal | Small / atrophic |
| Testis consistency | Normal/firm | Soft |
| Semen volume | Normal or low | Normal |
| Vas deferens | May be absent (CBAVD) | Present |
| Biopsy | Normal spermatogenesis | Spermatogenic failure pattern |
| Sperm retrieval rate | ~100% | ~50% with micro-TESE |
| Treatment | Reconstruction / MESA | Micro-TESE + ICSI |
Recent literature note: Reviews published in 2024-2025 (PMID 37737473, 39243180, 39268812) emphasize expanding genetic and epigenetic characterization of NOA and refining the OA vs NOA distinction. No major departures from standard textbook management have been identified, but genetic biomarker panels for predicting micro-TESE success are an active research area.
This is a shared conversation. Sign in to Orris to start your own chat.