Notes for structure of nephron / microscopic structure of kidney, juxtaglomerular apparatus, micro circulation of kidney
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full notes.
Microscopic Structure of the Kidney / Nephron - Complete Notes
1. Structure of the Nephron
Overview
- Each kidney contains approximately 1 million nephrons - the functional unit of the kidney.
- A nephron = glomerulus + renal tubule.
- The glomerulus is a capillary network arising from an afferent arteriole, surrounded by Bowman's capsule (Bowman's space).
- Blood is ultrafiltered across glomerular capillaries into Bowman's space - first step in urine formation.
- The tubule is lined by epithelial cells serving reabsorption and secretion.
(Costanzo Physiology 7th Edition)
Segments of the Nephron (in order)
| Segment | Abbreviation |
|---|---|
| Proximal convoluted tubule | PCT |
| Proximal straight tubule | PST |
| Thin descending limb of loop of Henle | tDLH |
| Thin ascending limb of loop of Henle | tALH |
| Thick ascending limb of loop of Henle | TAL |
| Distal convoluted tubule | DCT |
| Connecting tubule | CNT |
| Cortical collecting tubule | CCT |
| Outer medullary collecting duct | OMCD |
| Inner medullary collecting duct | IMCD |
(Medical Physiology, Boron & Boulpaep)
Types of Nephrons
| Feature | Superficial Cortical Nephrons | Juxtamedullary Nephrons |
|---|---|---|
| Glomeruli location | Outer cortex | Near corticomedullary border |
| Loop of Henle | Short - descends only to outer medulla | Long - descends deep into inner medulla |
| Role | General filtration | Concentrating urine (countercurrent) |
Microscopic Features of Tubule Segments
Proximal Convoluted Tubule (PCT)
- Cells have a prominent brush border (microvilli) on the apical/luminal surface.
- This greatly increases surface area for reabsorption - the PCT reabsorbs the bulk of filtered fluid (~67% Na+, glucose, amino acids, water, bicarbonate).
- Basolateral membranes form extensive interdigitations with abundant mitochondria (energy-intensive active transport).
- Cells contain lysosomes, endocytic vacuoles, well-developed ER, and prominent Golgi.
- S1 → S2 → S3 segments: progressively less complex brush border, fewer mitochondria, reduced reabsorption.
- A central cilium (mechano/flow sensor) protrudes from the apical pole.
Thin Descending and Ascending Limbs of Loop of Henle
- Simple, flat squamous epithelium - minimal cell complexity.
- Very few mitochondria; little membrane amplification.
- Thin descending limb: freely permeable to water, not to solutes.
- Thin ascending limb: impermeable to water, some solute permeability.
Thick Ascending Limb (TAL)
- Cuboidal to low columnar cells with basolateral Na+/K+-ATPase activity.
- Impermeable to water - actively transports NaCl out (site of action of loop diuretics).
Distal Convoluted Tubule (DCT)
- Cells are smaller and flatter than PCT cells.
- No brush border - empty-looking lumens.
- Fewer mitochondria → less acidophilic than PCT.
- More nuclei visible per section (due to smaller cell volume).
- Na+ reabsorption regulated by aldosterone.
Collecting Duct
- Principal cells: Stubby microvilli, prominent glycocalyx, invaginated basal membrane, deep tight junctions. Regulated by ADH (aquaporin insertion) and aldosterone.
- Intercalated cells (Type A): Dark cytoplasm, many mitochondria, apical microfolds - responsible for H+ secretion and acid-base regulation.
(Comprehensive Clinical Nephrology 7th Ed; Medical Physiology; Histology - Text and Atlas)
2. Juxtaglomerular Apparatus (JGA)
Components
The JGA has three components:
- Macula Densa
- Juxtaglomerular (JG) Granular Cells (also called juxtaglomerular cells)
- Extraglomerular Mesangial Cells (Lacis cells)
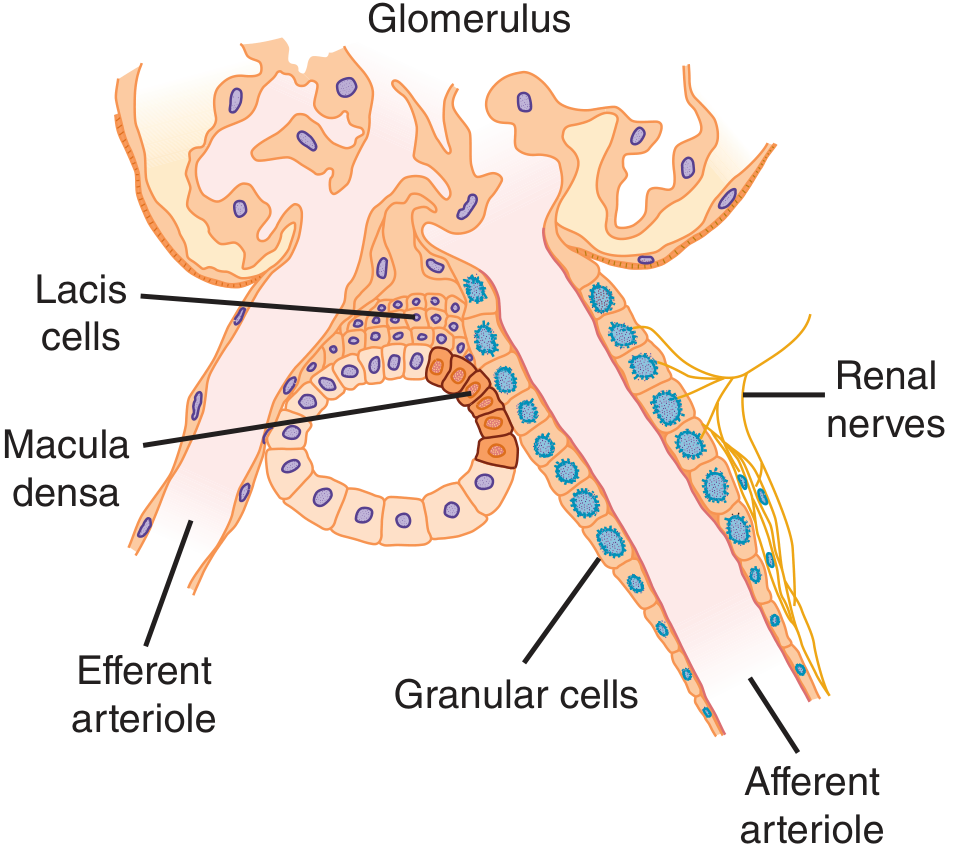
1. Macula Densa
- A plaque of specialized tubular epithelial cells in the wall of the thick ascending limb of Henle (TAL), at the site where it makes contact with the parent glomerulus at the vascular pole.
- Cells are narrowly packed, taller and narrower than other distal tubule cells, with crowded nuclei (hence the name - "dense spot").
- Cells are anchored to a basement membrane blending with the extraglomerular mesangium matrix.
- Joined by tight junctions with very low permeability; prominent lateral intercellular spaces that vary with functional state.
- High content of neuronal NOS (nNOS) and cyclooxygenase-2 (COX-2) - key for paracrine signaling.
- Function: Senses NaCl concentration/delivery in tubular fluid; triggers tubuloglomerular feedback.
2. Juxtaglomerular (Granular) Cells
- Modified smooth muscle cells in the media of the afferent arteriole (and sometimes efferent arteriole) near the glomerulus.
- Have spherical nuclei (unlike normal elongated smooth muscle nuclei), rough ER, Golgi complex.
- Contain membrane-lined secretory granules filled with renin (an aspartyl protease).
- Act as baroreceptors: reduced stretch (low BP) stimulates renin release.
3. Extraglomerular Mesangial Cells (Lacis Cells / EGM cells)
- Located at the junction between the afferent and efferent arterioles, adjacent to the macula densa.
- Heavily branched cells interconnected by gap junctions, containing prominent bundles of microfilaments.
- No blood vessels or lymphatics penetrate this region.
- Share supportive, contractile, and phagocytic properties with intraglomerular mesangial cells.
Functions of the JGA
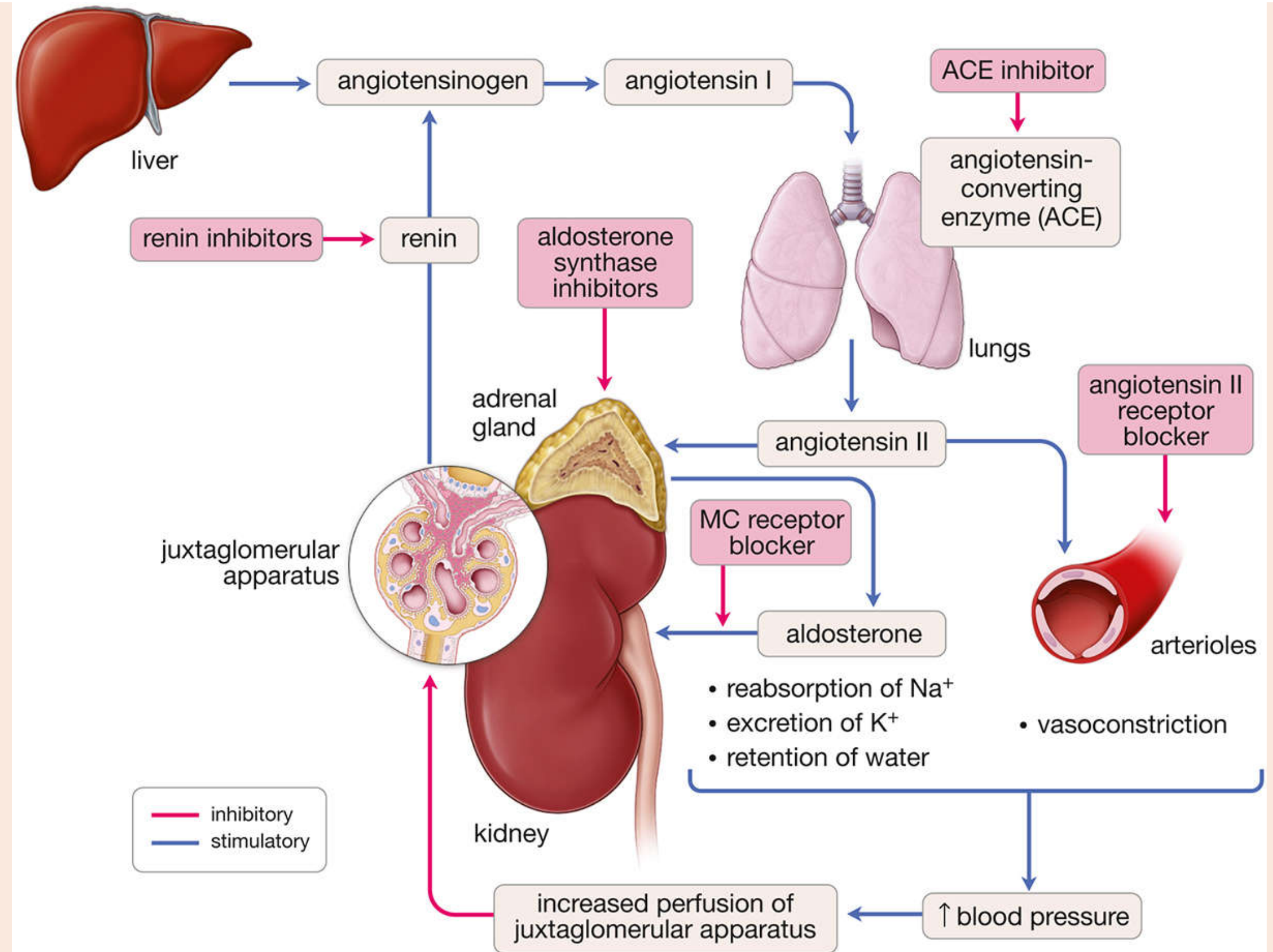
A. Renin-Angiotensin-Aldosterone System (RAAS) Activation
Renin is released from JG cells in response to:
- Decreased afferent arteriolar stretch (low BP - baroreceptor mechanism)
- Increased sympathetic activity (via renal nerves, β1 receptors)
- Increased circulating catecholamines
- Prostaglandins
Renin release is inhibited by:
- Increased NaCl reabsorption across macula densa
- Increased afferent arteriolar pressure
- Angiotensin II (negative feedback)
- Vasopressin
Renin cleaves angiotensinogen (hepatic α2-globulin) → Angiotensin I → converted by ACE (in lungs) → Angiotensin II → vasoconstriction + aldosterone release.
B. Tubuloglomerular Feedback (TGF)
The JGA links tubular NaCl delivery to GFR control:
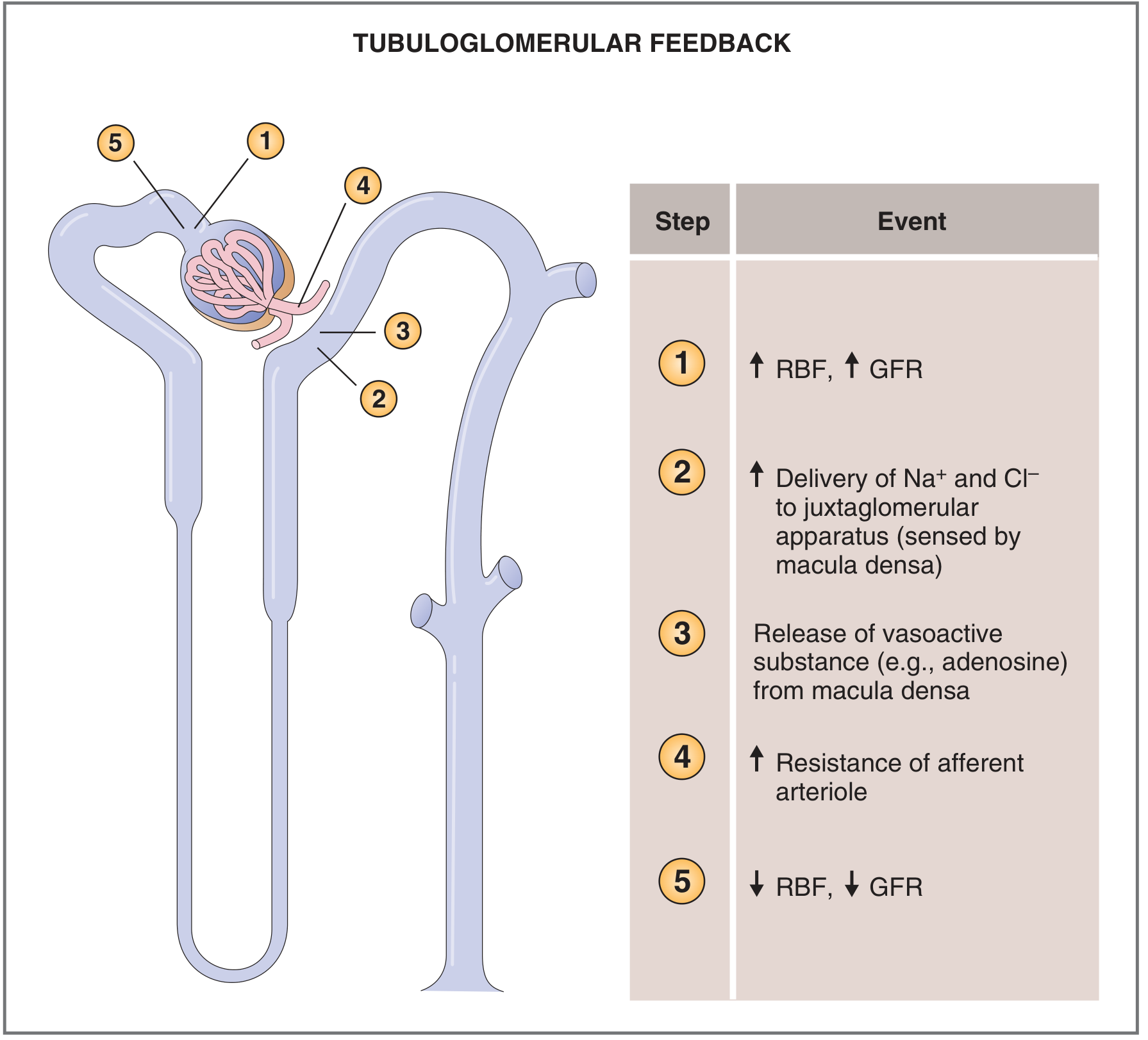
Step-by-step:
- ↑ RBF → ↑ GFR
- ↑ delivery of Na+/Cl- to macula densa (sensed)
- Macula densa releases adenosine (vasoactive paracrine substance)
- Adenosine → constricts afferent arteriole → ↑ resistance
- ↓ RBF and ↓ GFR (returns to normal)
(Ganong's Review of Medical Physiology; Costanzo Physiology 7th Ed; Junqueira's Basic Histology 17e; Comprehensive Clinical Nephrology 7th Ed)
3. Microcirculation of the Kidney
General Overview
- The kidneys receive ~22-25% of cardiac output despite being only ~0.4% of body weight.
- In an adult (~70 kg): Renal Blood Flow (RBF) ≈ 1100-1250 mL/min (~1800 L/day).
- This massive flow is not for metabolic needs alone - it supports the high filtration rate required for precise body fluid regulation.
(Guyton & Hall Textbook of Medical Physiology; Costanzo Physiology 7th Ed)
Vascular Pathway (Microcirculation)
Renal artery
↓
Interlobar arteries (between pyramids)
↓
Arcuate arteries (arch at corticomedullary junction)
↓
Interlobular (cortical radiate) arteries
↓
Afferent arterioles → Glomerular capillaries → Efferent arterioles
↓ ↓
(cortical nephrons) (juxtamedullary nephrons)
Peritubular capillaries Vasa Recta
↓ ↓
Interlobular veins → Arcuate veins → Interlobar veins → Renal vein
Key unique feature: Two capillary beds in series (glomerular + peritubular/vasa recta) separated by efferent arteriole - this is unique to the kidney.
Pressure Profile and Vascular Resistance
| Vessel | Pressure (mmHg) | % of Total Resistance |
|---|---|---|
| Renal artery | 100 | ~0 |
| Interlobar/arcuate/interlobular arteries | 100 → 85 | ~16% |
| Afferent arteriole | 85 → 60 | ~26% |
| Glomerular capillaries | 60 → 59 | ~1% |
| Efferent arteriole | 59 → 18 | ~43% |
| Peritubular capillaries | 18 → 8 | ~10% |
| Veins | 8 → 4 | ~4% |
- The efferent arteriole is the dominant resistance vessel in the renal circulation.
- Both afferent and efferent arterioles are the primary sites of regulation.
(Guyton & Hall; Costanzo)
Vasa Recta (Medullary Microcirculation)
- Arise from efferent arterioles of juxtamedullary nephrons.
- Run parallel to the long loops of Henle, descending into the medulla then looping back.
- Medulla receives only 1-2% of total RBF (vs. most flow going to cortex).
- Low medullary flow preserves the osmotic gradient needed for urine concentration.
- Vasa recta act as countercurrent exchangers - solutes and water exchange passively to maintain medullary hypertonicity.
Regulation of Renal Blood Flow
Vasoconstrictors vs. Vasodilators
| Vasoconstrictors | Vasodilators |
|---|---|
| Sympathetic nerves (catecholamines, α1) | PGE2, PGI2 |
| Angiotensin II | Nitric oxide |
| Endothelin | Bradykinin |
| Dopamine | |
| Atrial natriuretic peptide (ANP) |
Sympathetic Nervous System
- Both afferent and efferent arterioles are innervated by sympathetic (α1) fibers.
- More α1 receptors on afferent arterioles → increased SNS activity → ↓ RBF and ↓ GFR (e.g., in hemorrhage, baroreceptor reflex sacrifices renal flow to restore systemic BP).
Angiotensin II
- Constricts both afferent and efferent arterioles.
- Efferent arterioles are more sensitive to Ang II.
- Low Ang II → preferential efferent constriction → ↑ GFR (glomerular pressure maintained).
- High Ang II → constricts both → ↓ RBF and ↓ GFR.
Autoregulation (80-200 mmHg range)
RBF remains constant over mean arterial pressure of 80-200 mmHg via two mechanisms:
1. Myogenic Mechanism:
- ↑ arterial pressure → stretches afferent arteriole wall → opens stretch-activated Ca2+ channels → smooth muscle contracts → ↑ resistance → RBF maintained.
2. Tubuloglomerular Feedback (JGA-mediated, see above):
- ↑ pressure → ↑ GFR → ↑ NaCl to macula densa → adenosine → afferent arteriolar constriction → ↓ RBF and GFR back to normal.
- Autoregulation is intrinsic (independent of renal innervation - transplanted kidneys autoregulate normally).
Oxygen Consumption
- Kidney O2 consumption is ~2x that of brain per gram weight.
- Renal O2 use is mainly for active Na+ reabsorption by tubules.
- O2 consumption ∝ sodium reabsorption ∝ GFR.
- If GFR ceases → sodium reabsorption stops → O2 consumption drops to ~1/4 normal (residual basal cell needs).
(Guyton & Hall Textbook of Medical Physiology)
Sources
- Costanzo Physiology, 7th Edition - Structure of the Nephron, Renal Blood Flow, Autoregulation
- Guyton and Hall Textbook of Medical Physiology - Renal Blood Flow, Vasa Recta, Determinants of RBF
- Comprehensive Clinical Nephrology, 7th Edition - Juxtaglomerular Apparatus
- Ganong's Review of Medical Physiology, 26th Edition - JGA, Renin Secretion
- Junqueira's Basic Histology, 17th Edition - DCT, JGA histology
- Histology: A Text and Atlas (Pawlina) - JGA cells, RAAS
- Medical Physiology (Boron & Boulpaep) - Tubule ultrastructure, nephron segments, TGF
Notes for structure of nephron / microscopic structure of kidney, juxtaglomerular apparatus, micro circulation of kidney. Need asap 😭🙏🏻. Please give me fast, don't need pictures, just give me the content
Here are your complete notes - straight from the textbooks, no fluff:
Kidney - Microscopic Structure, Nephron, JGA & Microcirculation
PART 1: STRUCTURE OF THE NEPHRON
Basic Facts
- Each kidney has ~1 million nephrons
- Nephron = Glomerulus + Renal Tubule
- Glomerulus = capillary network arising from afferent arteriole, surrounded by Bowman's capsule
- Blood is ultrafiltered into Bowman's space → first step of urine formation
- Tubule is lined by epithelial cells → reabsorption + secretion
Two Types of Nephrons
| Feature | Cortical (Superficial) | Juxtamedullary |
|---|---|---|
| Glomeruli location | Outer cortex | Near corticomedullary border |
| Loop of Henle | Short - only outer medulla | Long - deep into inner medulla |
| Role | General filtration | Urine concentration |
Segments of the Nephron (in order)
- Proximal Convoluted Tubule (PCT)
- Proximal Straight Tubule (PST)
- Thin Descending Limb of Loop of Henle (tDLH)
- Thin Ascending Limb of Loop of Henle (tALH)
- Thick Ascending Limb of Loop of Henle (TAL)
- Distal Convoluted Tubule (DCT)
- Connecting Tubule (CNT)
- Cortical Collecting Tubule (CCT)
- Outer Medullary Collecting Duct (OMCD)
- Inner Medullary Collecting Duct (IMCD)
Microscopic Features - Segment by Segment
Proximal Convoluted Tubule (PCT)
- Prominent brush border (microvilli) on apical/luminal surface → huge surface area for reabsorption
- Reabsorbs ~67% of filtered Na+, glucose, amino acids, bicarbonate, water
- Basolateral membranes have extensive interdigitations packed with mitochondria (ATP for active transport)
- Contains lysosomes, endocytic vacuoles, well-developed ER, Golgi
- Sub-segments: S1 → S2 → S3: progressively less complex brush border, fewer mitochondria, reduced reabsorption rate
- All tubule cells have a single central cilium on the apical surface (senses tubular fluid flow)
Thin Descending Limb (tDLH)
- Simple flat squamous epithelium
- Very few mitochondria, minimal membrane amplification
- Freely permeable to water, impermeable to solutes
Thin Ascending Limb (tALH)
- Also simple flat epithelium
- Impermeable to water, some solute permeability
Thick Ascending Limb (TAL)
- Cuboidal to low columnar cells
- Active NaCl transport (Na+/K+/2Cl- cotransporter = NKCC2)
- Completely impermeable to water → dilutes tubular fluid
- Site of action of loop diuretics (furosemide)
Distal Convoluted Tubule (DCT)
- Cells are smaller and flatter than PCT
- No brush border → lumens appear empty/wide
- Fewer mitochondria → less acidophilic than PCT
- More nuclei visible per cross-section (cells smaller)
- Na+ reabsorption regulated by aldosterone
Collecting Duct - Two Cell Types
Principal Cells:
- Stubby microvilli, prominent glycocalyx
- Deep tight junctions, basal membrane invaginations
- Regulated by ADH (insert aquaporin-2 → water reabsorption)
- Also regulated by aldosterone (Na+ reabsorption, K+ excretion)
Intercalated Cells (Type A):
- Dark cytoplasm, many mitochondria
- Apical microfolds
- Responsible for H+ secretion and bicarbonate reabsorption → acid-base regulation
PART 2: JUXTAGLOMERULAR APPARATUS (JGA)
Location
At the vascular pole of the glomerulus, where the distal tubule loops back and contacts its parent glomerulus.
Three Components
1. Macula Densa
- Plaque of specialized epithelial cells in the wall of the TAL (thick ascending limb) at the vascular pole
- Cells are taller, narrower, closely packed with crowded (dense) nuclei → hence the name
- Anchored to a basement membrane that blends with extraglomerular mesangium
- Cells joined by tight junctions with very low permeability
- Lateral intercellular spaces vary with functional state
- High content of neuronal NOS (nNOS) and COX-2 (key paracrine mediators)
- Function: Senses NaCl concentration/delivery in tubular fluid → triggers tubuloglomerular feedback + controls renin release
2. Juxtaglomerular (JG) Granular Cells
- Modified smooth muscle cells in the tunica media of the afferent arteriole (occasionally efferent too)
- Spherical nuclei (unlike normal elongated smooth muscle nuclei)
- Contain rough ER, Golgi, and membrane-bound secretory granules packed with renin
- Act as intrarenal baroreceptors: ↓ stretch (↓ BP) → ↑ renin release
- Also called epithelioid cells or granular cells
3. Extraglomerular Mesangial Cells (Lacis Cells / EGM Cells)
- Located at the junction between afferent and efferent arterioles, adjacent to macula densa
- Heavily branched; interconnected by gap junctions
- Contain prominent microfilament bundles (contractile)
- No blood vessels or lymphatics in this region
- Share supportive, contractile, and phagocytic functions with intraglomerular mesangial cells
- Also called lacis cells (French: lacework)
Functions of the JGA
A. Renin Release and RAAS Activation
Stimuli for renin release:
- ↓ stretch of afferent arteriole (↓ BP) - intrarenal baroreceptor
- ↑ Sympathetic activity (via β1 receptors on JG cells)
- ↑ Circulating catecholamines
- Prostaglandins (PGE2, PGI2)
- ↓ NaCl delivery to macula densa
Inhibition of renin release:
- ↑ Afferent arteriolar pressure (↑ stretch)
- ↑ NaCl reabsorption across macula densa
- Angiotensin II (negative feedback)
- Vasopressin (ADH)
RAAS Cascade:
Renin → cleaves angiotensinogen (liver) → Angiotensin I → ACE in lungs → Angiotensin II → vasoconstriction + aldosterone from adrenal cortex → Na+ reabsorption + K+ excretion + ↑ BP
B. Tubuloglomerular Feedback (TGF)
Mechanism of autoregulation linking tubular NaCl delivery to GFR:
- ↑ Arterial pressure → ↑ RBF → ↑ GFR
- ↑ NaCl/water delivery to macula densa
- Macula densa releases adenosine (paracrine vasoactive substance)
- Adenosine → constricts afferent arteriole → ↑ resistance
- ↓ RBF and ↓ GFR → returns to normal
PART 3: MICROCIRCULATION OF THE KIDNEY
General Facts
- Kidneys receive ~22-25% of cardiac output despite being only 0.4% of body weight
- Normal RBF ≈ 1100-1250 mL/min (~1800 L/day in a 70 kg adult)
- Purpose: not just nutrition - supports high GFR for precise fluid/electrolyte regulation
- Unique feature: Two capillary beds in series (glomerular + peritubular) separated by the efferent arteriole
Vascular Pathway
Renal artery
↓
Interlobar arteries (run between pyramids)
↓
Arcuate arteries (arch at corticomedullary junction)
↓
Interlobular arteries (cortical radiate arteries)
↓
Afferent arterioles
↓
Glomerular capillaries (1st capillary bed)
↓
Efferent arterioles
↓ (splits based on nephron type)
Cortical nephrons: Juxtamedullary nephrons:
Peritubular capillaries Vasa Recta
↓ ↓
→ Interlobular veins → Arcuate veins → Interlobar veins → Renal vein
Pressure Profile and Resistance Distribution
| Vessel | Pressure Start → End (mmHg) | % Total Resistance |
|---|---|---|
| Renal artery | 100 | ~0% |
| Interlobar/arcuate/interlobular arteries | 100 → 85 | ~16% |
| Afferent arteriole | 85 → 60 | ~26% |
| Glomerular capillaries | 60 → 59 | ~1% |
| Efferent arteriole | 59 → 18 | ~43% |
| Peritubular capillaries | 18 → 8 | ~10% |
| Veins | 8 → 4 | ~4% |
- Efferent arteriole = dominant resistance vessel in renal circulation
- Glomerular capillary pressure (~60 mmHg) is much higher than other capillary beds → drives filtration
Peritubular Capillaries
- Arise from efferent arterioles of cortical nephrons
- Low pressure (after efferent arteriole) → favors reabsorption of fluid from tubules back into blood
- Surround the proximal and distal tubules in the cortex
Vasa Recta (Medullary Circulation)
- Arise from efferent arterioles of juxtamedullary nephrons
- Run parallel to long loops of Henle, descend into medulla then loop back → hairpin structure
- Medulla receives only 1-2% of total RBF (most goes to cortex)
- Low flow deliberately preserves medullary osmotic gradient for urine concentration
- Act as countercurrent exchangers: solutes and water exchange passively across vasa recta walls → hypertonicity maintained
Regulation of Renal Blood Flow
Vasoconstrictors vs. Vasodilators
| Vasoconstrictors | Vasodilators |
|---|---|
| Sympathetic nerves (α1 - catecholamines) | PGE2, PGI2 (prostaglandins) |
| Angiotensin II | Nitric oxide (NO) |
| Endothelin | Bradykinin |
| Dopamine | |
| Atrial Natriuretic Peptide (ANP) |
Sympathetic Nervous System
- Innervates both afferent and efferent arterioles via α1 receptors
- More α1 receptors on afferent arterioles
- ↑ SNS activity (e.g., hemorrhage) → afferent constriction → ↓ RBF and ↓ GFR
- Body sacrifices renal blood flow to restore systemic BP via baroreceptor reflex
Angiotensin II
- Constricts both afferent and efferent arterioles
- Efferent arteriole is more sensitive to Ang II
- Low Ang II: preferentially constricts efferent → ↑ GFR (glomerular pressure maintained)
- High Ang II: constricts both → ↓ RBF + ↓ GFR
Autoregulation of RBF
- RBF remains constant over mean arterial pressure range of 80-200 mmHg
- Below 80 mmHg → RBF falls
- Mechanism is intrinsic (transplanted/denervated kidneys autoregulate normally)
Two mechanisms:
1. Myogenic Mechanism
- ↑ Arterial pressure → stretches afferent arteriole wall
- Opens stretch-activated Ca²+ channels → Ca²+ enters smooth muscle
- Smooth muscle contracts → ↑ resistance → RBF stays constant
- Quick response (seconds)
2. Tubuloglomerular Feedback (TGF)
- ↑ Pressure → ↑ GFR → ↑ NaCl to macula densa → adenosine release → afferent constriction → ↓ RBF and GFR normalized
- (Same as described in JGA section above)
Renal Oxygen Consumption
- Kidneys consume O2 at 2x the rate of brain per gram weight but receive 7x the blood flow of the brain
- O2 delivery far exceeds metabolic needs → low arteriovenous O2 extraction
- Most O2 is used for active Na+ reabsorption (tubular Na+/K+-ATPase)
- O2 consumption ∝ Na+ reabsorption ∝ GFR
- If GFR stops → Na+ reabsorption stops → O2 consumption drops to ~1/4 of normal (residual basal cell metabolism only)
Quick Comparison Summary
| Feature | Cortex | Medulla |
|---|---|---|
| Blood supply | Peritubular capillaries | Vasa recta |
| % of RBF | ~98-99% | ~1-2% |
| Origin | Efferent of cortical nephrons | Efferent of juxtamedullary nephrons |
| Role | Reabsorption support | Countercurrent exchange, urine concentration |
| O2 tension | Higher | Lower (prone to ischemia) |
Sources: Costanzo Physiology 7e | Guyton & Hall Medical Physiology | Comprehensive Clinical Nephrology 7e | Ganong's Review of Medical Physiology 26e | Junqueira's Basic Histology 17e | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.