What is headache? explain types and cure in details
Reading File
Finding Sources
Searching the Web
headache types classification treatment 2024
Searching PubMed
"headache" AND "classification"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have excellent comprehensive data from multiple authoritative sources. Let me compile the full detailed answer.
Headache: Definition, Types, and Treatment
What is a Headache?
A headache is pain or discomfort felt anywhere in the head, scalp, neck, or upper back that arises from pain-sensitive structures - including blood vessels, meninges, cranial nerves, and muscles. The brain tissue itself has no pain receptors; headache pain arises when surrounding structures are irritated, inflamed, stretched, or compressed.
Headache is one of the most common medical complaints worldwide, affecting approximately 90% of individuals during their lifetime (J Am Board Fam Med, 2024). It is consistently among the top reasons for emergency department visits.
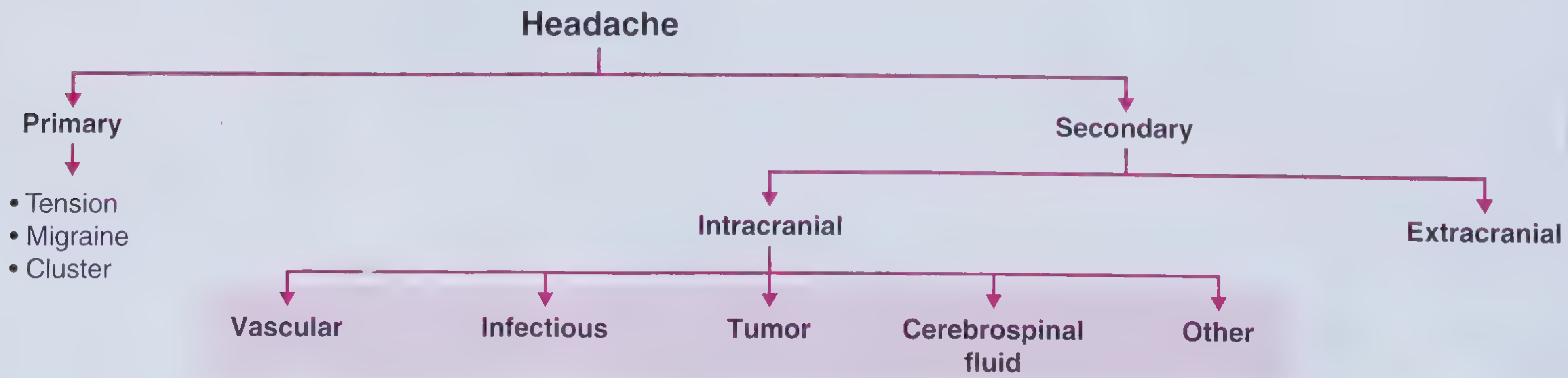
Classification: Primary vs. Secondary
Headaches are divided into two fundamental categories:
| Category | Definition | Examples |
|---|---|---|
| Primary | The headache itself is the disorder; no underlying disease causes it | Tension-type, Migraine, Cluster |
| Secondary | Headache is a symptom of another condition | Meningitis, brain tumor, SAH, hypertension |
Headaches occurring fewer than 15 days/month are episodic; those occurring more than 15 days/month are chronic.
PRIMARY HEADACHES
1. Tension-Type Headache (TTH)
The most common type of headache.
Features:
- Location: Bilateral, described as a "band" or "vice" around the entire head
- Character: Dull, persistent, pressing/tightening - NOT throbbing
- Severity: Mild to moderate
- Duration: 30 minutes to 7 days
- NOT worsened by physical activity (unlike migraine)
- May have mild light/sound sensitivity and mild anorexia, but no nausea/vomiting
Subtypes:
- Infrequent episodic - less than 1 day/month
- Frequent episodic - 1-14 days/month
- Chronic - more than 15 days/month
Triggers: Stress, reduced sleep, missed meals, muscle tension in neck/shoulders
Treatment:
- Acute: Ibuprofen 400 mg or acetaminophen 1000 mg (NSAIDs preferred); aspirin
- Prevention (chronic TTH): Amitriptyline 50-100 mg significantly reduces monthly headache days
- Non-pharmacological: Cognitive behavioral therapy, adequate rest, moist heat, massage, aerobic exercise
2. Migraine
The second most common primary headache, and the most disabling.
Features:
- Location: Usually unilateral (one side), but can be bilateral
- Character: Pulsating, throbbing
- Severity: Moderate to severe
- Duration: 2-72 hours per episode
- Worsened by physical activity
- Associated symptoms: Nausea, vomiting, photophobia (light sensitivity), phonophobia (sound sensitivity), osmophobia (smell sensitivity)
- Frequency: 1-5 attacks per month in severe cases
Migraine Phases:
- Prodrome (hours to days before): fatigue, difficulty concentrating, mood changes
- Aura (in ~30% of patients): visual disturbances (zigzag lines, blind spots), sensory symptoms, or speech difficulty - usually lasts 20-60 minutes
- Headache phase: the main throbbing pain
- Postdrome: fatigue, confusion after pain resolves
Pathophysiology: The aura is caused by cortical spreading depression - a wave of neuronal suppression - associated with brief reduction in blood flow followed by hyperemia. Pain occurs when trigeminal afferents of the dura are stimulated. Calcitonin gene-related peptide (CGRP) plays a key role in migraine pain signaling.
Comorbidities: Epilepsy, depression, anxiety, stroke, fibromyalgia, irritable bowel syndrome.
Treatment - Acute (Mild attacks):
- Acetaminophen 650-1000 mg
- NSAIDs: Aspirin 250-1000 mg, Ibuprofen 400-600 mg, Naproxen 500-825 mg, Diclofenac 50 mg
Treatment - Acute (Moderate/Severe attacks):
- Triptans (first-line migraine-specific): Sumatriptan, Rizatriptan, Zolmitriptan, Eletriptan, Frovatriptan, Naratriptan, Almotriptan - these are serotonin (5-HT1B/1D) agonists that cause vasoconstriction and block pain signals. Contraindicated in cardiovascular disease.
- Gepants (CGRP antagonists): Ubrogepant, Rimegepant - for patients who cannot tolerate triptans; oral administration, lower cardiovascular risk
- Ergotamine/Dihydroergotamine (DHE): Older agents, still used for severe/refractory migraines
- Parenteral options (emergency): Dopamine antagonists (metoclopramide, prochlorperazine), ketorolac IV
- Note: Opioids are NOT recommended for primary headaches
Treatment - Prevention (if 2+ attacks/month):
- Beta-blockers (first-line): Propranolol, Metoprolol
- Anticonvulsants: Topiramate, Divalproex sodium (valproate)
- Antidepressants: Amitriptyline, Venlafaxine
- Calcium channel blockers: Verapamil
- CGRP monoclonal antibodies (newer): Erenumab, Galcanezumab, Fremanezumab, Eptinezumab (injectable, once monthly/quarterly)
- Oral CGRP antagonists (prevention): Rimegepant, Atogepant
- OnabotulinumtoxinA (Botox): For chronic migraine (not episodic)
- Aerobic exercise and physiotherapy can also reduce attack frequency
3. Cluster Headache
The most severe primary headache - often called "suicide headache" due to its intensity.
Features:
- Location: Strictly unilateral - behind or around ONE eye; never switches sides during an attack
- Character: Excruciating, sharp, stabbing, steady (not throbbing)
- Severity: Extreme - among the most painful conditions known
- Duration: 15-90 minutes per episode
- Occurs in "clusters" - multiple attacks per day (1-8/day) for weeks to months, followed by remission periods
- Onset: Often during sleep
- Sex: Males more often than females (3:1)
- Autonomic features (hallmark): Ipsilateral lacrimation, nasal congestion/rhinorrhea, ptosis (drooping eyelid), miosis, facial flushing, sweating around the eye
- Patient is typically restless and agitated (unlike migraine patients who prefer to lie still)
Treatment - Acute (abortive):
- 100% oxygen inhalation (7-12 L/min for 15 minutes) - highly effective, fast onset
- Sumatriptan (subcutaneous injection 6 mg) - fastest-acting triptan for cluster
- Zolmitriptan nasal spray
Treatment - Prevention:
- Verapamil (calcium channel blocker) - first-line preventive
- Lithium - for chronic cluster
- Topiramate, Divalproex
- Short-course corticosteroids - to break a cluster cycle
- Occipital nerve blocks (injections)
4. Other Notable Primary Headaches
| Type | Key Feature |
|---|---|
| Hemicrania continua | Continuous, strictly one-sided, responds only to indomethacin |
| Chronic daily headache | Headache on >15 days/month for >3 months |
| Medication overuse headache (MOH) | From overusing pain medications (especially opioids, triptans >10-15 days/month); treated by gradual withdrawal |
| Exertional headache | Triggered by physical exertion |
| Ice pick headache | Brief, stabbing jabs of pain |
| Thunderclap headache | Maximum-intensity headache within 1 minute - ALWAYS requires emergency evaluation to rule out subarachnoid hemorrhage (SAH) |
SECONDARY HEADACHES
These are caused by an identifiable underlying condition. The headache resolves when the underlying cause is treated.
Red Flags ("SNOOP4" features that demand urgent workup):
- Systemic symptoms (fever, weight loss) or immunosuppression (HIV, cancer)
- Neurological deficits (focal weakness, vision loss, confusion)
- Onset sudden/thunderclap ("worst headache of my life")
- Older age at onset (new headache after age 50)
- Progressive worsening
- Posture-related (worse lying down, or only when upright)
- Papilledema (raised intracranial pressure)
- Pregnancy
Common Secondary Headache Causes:
| Cause | Key Features |
|---|---|
| Subarachnoid hemorrhage (SAH) | Thunderclap headache; "worst headache of life"; emergency - CT head then LP |
| Meningitis/Encephalitis | Fever, neck stiffness, photophobia, altered consciousness |
| Idiopathic intracranial hypertension | Obese women; pulsatile tinnitus, papilledema; treated with acetazolamide, weight loss |
| Intracranial hypotension | Worse when upright, better lying down; caused by CSF leak |
| Brain tumor | Progressive headache, worse in morning, with vomiting, focal deficits |
| Hypertension headache | BP usually >180/120; occipital, morning headache |
| Temporal (giant cell) arteritis | Age >50; tender scalp/temporal artery; risk of blindness; treat with steroids |
| Sinus headache | Facial pressure/tenderness, nasal congestion, worse bending forward |
| Post-traumatic headache | Follows head injury; can persist for months |
Comparison Table: The Three Main Primary Headaches
| Feature | Migraine | Cluster | Tension-Type |
|---|---|---|---|
| Location | Usually unilateral | Behind/around one eye | Bilateral "band" |
| Character | Pulsating, throbbing | Excruciating, sharp, steady | Dull, pressing, tightening |
| Severity | Moderate-severe | Severe-excruciating | Mild-moderate |
| Duration | 2-72 hours | 15-90 minutes | 30 min - 7 days |
| Nausea/Vomiting | Yes | Rarely | No |
| Photophobia/Phonophobia | Yes | Mild | Mild/none |
| Autonomic features | No | Yes (eye tearing, nasal congestion) | No |
| Activity worsens it | Yes | No (patient paces) | No |
| Sex predominance | Female > Male | Male > Female | Female > Male |
| Family history | Yes | No | Sometimes |
| Acute treatment | Triptans, NSAIDs | Oxygen, Sumatriptan SC | NSAIDs, Acetaminophen |
| Prevention | Beta-blockers, CGRP mAbs | Verapamil | Amitriptyline |
General Lifestyle Measures for All Headaches
- Maintain regular sleep schedules
- Stay well-hydrated
- Eat regular meals (avoid skipping)
- Manage stress (mindfulness, CBT, biofeedback)
- Avoid known triggers (alcohol, caffeine excess, bright lights, strong smells)
- Regular aerobic exercise (150 min/week moderate intensity)
- Keep a headache diary to identify patterns and triggers
- Avoid medication overuse (limits >10-15 days/month depending on drug class)
Recent Evidence (2024-2026)
- A 2024 BMJ network meta-analysis found specific triptans and newer gepants had different efficacy and tolerability profiles for acute migraine management, helping refine drug selection.
- A 2026 Lancet Neurology review (PMID: 41722594) highlights significant advances in migraine prevention, particularly with CGRP-targeted therapies.
- The VA 2024 Clinical Practice Guideline recommends ibuprofen 400 mg or acetaminophen 1000 mg for acute tension headache, and amitriptyline for chronic TTH prevention.
Sources: Goldman-Cecil Medicine, 26th Ed. | Lippincott Illustrated Reviews: Pharmacology | Bradley and Daroff's Neurology in Clinical Practice | Rosen's Emergency Medicine | Frameworks for Internal Medicine | ICHD-3 Classification | VA/ACP Headache CPG 2024
This is a shared conversation. Sign in to Orris to start your own chat.