Senile cataract
Reading File
Finding Sources
Finding Sources
Searching PubMed
"age-related cataract" AND pathogenesis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer on senile cataract.
Senile (Age-Related) Cataract
A senile cataract is any opacification of the crystalline lens occurring as a consequence of aging. It is the leading cause of reversible blindness worldwide. In India, senile cataract occurs approximately a decade earlier than in Western populations.
Anatomy of the Lens (Relevant Background)
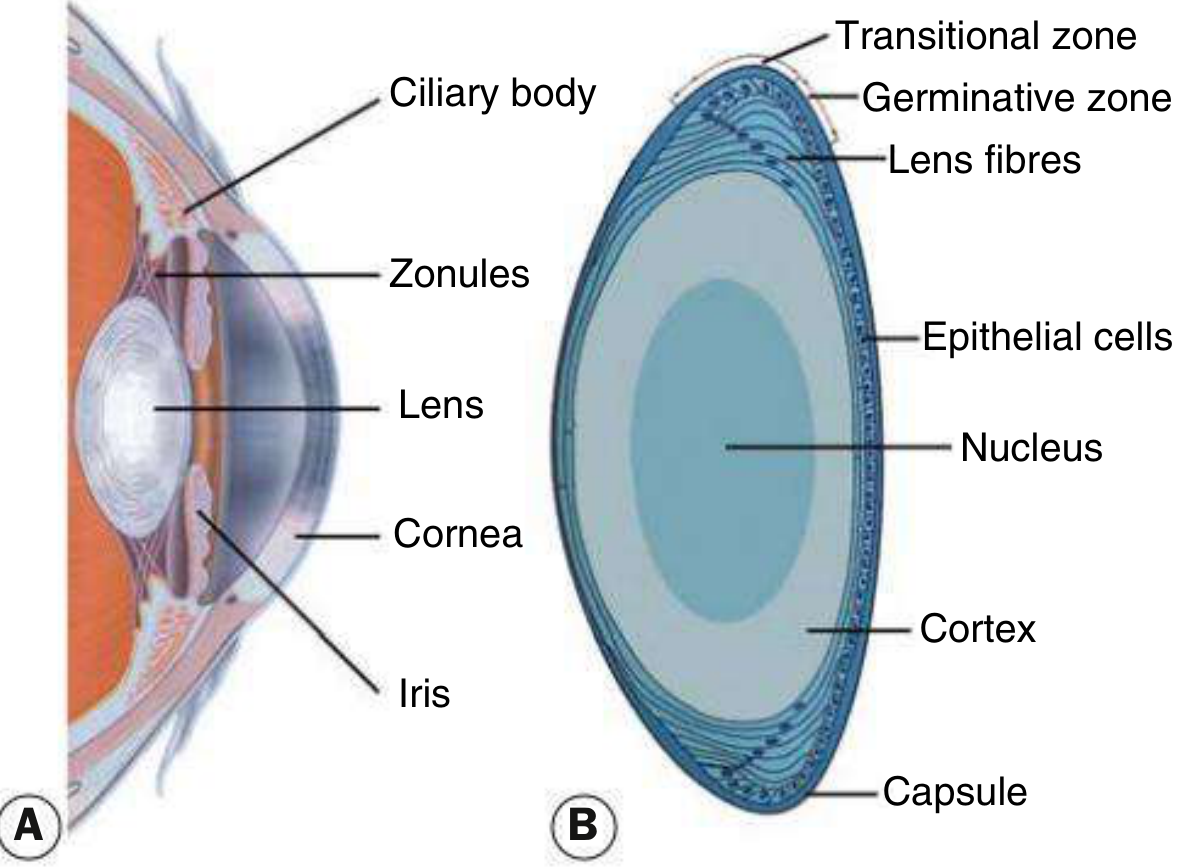
Fig. 10.1 from Kanski's Clinical Ophthalmology - (A) Anterior segment cross-section showing the lens, ciliary body, zonules, cornea and iris; (B) Lens histology showing nucleus, cortex, capsule, epithelial cells, lens fibres, germinative and transitional zones.
The lens is a biconvex, avascular, transparent structure suspended by zonular ligaments from the ciliary body. It consists of:
- Capsule - outer elastic basement membrane
- Epithelial cells - single anterior layer (the germinative zone produces new lens fibres throughout life)
- Cortex - superficial newer fibres
- Nucleus - central older, compacted fibres
Pathogenesis
Senile cataract occurs because lens proteins denature and degrade over time - Adams & Victor's Principles of Neurology, p. 254. The lens has no mechanism to remove damaged cells; accumulating protein changes progressively reduce transparency.
Key molecular mechanisms include:
- Oxidative damage - ROS attack lens crystallins, leading to protein aggregation and high-molecular-weight complexes that scatter light
- Glycation - non-enzymatic glycosylation of lens proteins (relevant in diabetes, where glucose is converted to sorbitol by aldose reductase, creating osmotic stress)
- Dehydration and ionic imbalance - breakdown of Na+/K+-ATPase pump leads to water influx and cortical hydration
- Urochrome pigment deposition - yellowing/browning of the nucleus with aging
Types / Morphological Classification
1. Posterior Subcapsular Cataract (PSC)
- Lies just in front of the posterior capsule
- Granular or plaque-like on oblique slit lamp; black and vacuolated on retroillumination (vacuoles = swollen Wedl/bladder cells - migratory lens epithelial cells)
- Located at the nodal point of the eye - disproportionately affects vision even at early stages
- Key symptom: glare (from oncoming headlights), worse with miosis (near work, bright sunlight)
- Also caused by: steroids, diabetes, radiation, retinitis pigmentosa
2. Nuclear Sclerotic Cataract
- Exaggeration of normal aging - compaction and hardening of the nucleus
- Yellowish hue due to urochrome pigment deposition (best seen on oblique slit beam)
- Advanced cases turn brown (brunescent) or rarely black (nigra)
- Classic feature: myopic shift ("second sight of the aged") - patient can suddenly read without spectacles because increased refractive index of nucleus causes index myopia
- Retroillumination shows preserved red reflex but subtle nucleus-cortex demarcation
3. Cortical Cataract
- Involves anterior, posterior or equatorial cortex
- Starts as clefts and vacuoles due to cortical hydration
- Progresses to cuneiform (wedge-shaped) or spoke-like radial opacities, typically beginning in the inferonasal quadrant
- Seen on slit lamp as spokes radiating from the lens equator
- Glare is common, similar to PSC
4. Christmas Tree Cataract
- Uncommon; polychromatic needle-like (iridescent) formations in the deep cortex and nucleus
- Associated with myotonic dystrophy
Stages of Senile Cataract (Classical)
| Stage | Features |
|---|---|
| Incipient | Early peripheral cortical opacities; vision largely unaffected |
| Immature | Opacities increase; lens takes on some fluid (intumescent); vision reduced; iris shadow present (oblique illumination test positive) |
| Mature | Complete opacification; lens appears white; no red reflex; iris shadow absent; vision reduced to perception of light |
| Hypermature | Lens proteins liquefy (Morgagnian); brown nucleus sinks to dependent position; risk of phacolytic glaucoma |
Slit Lamp Appearances
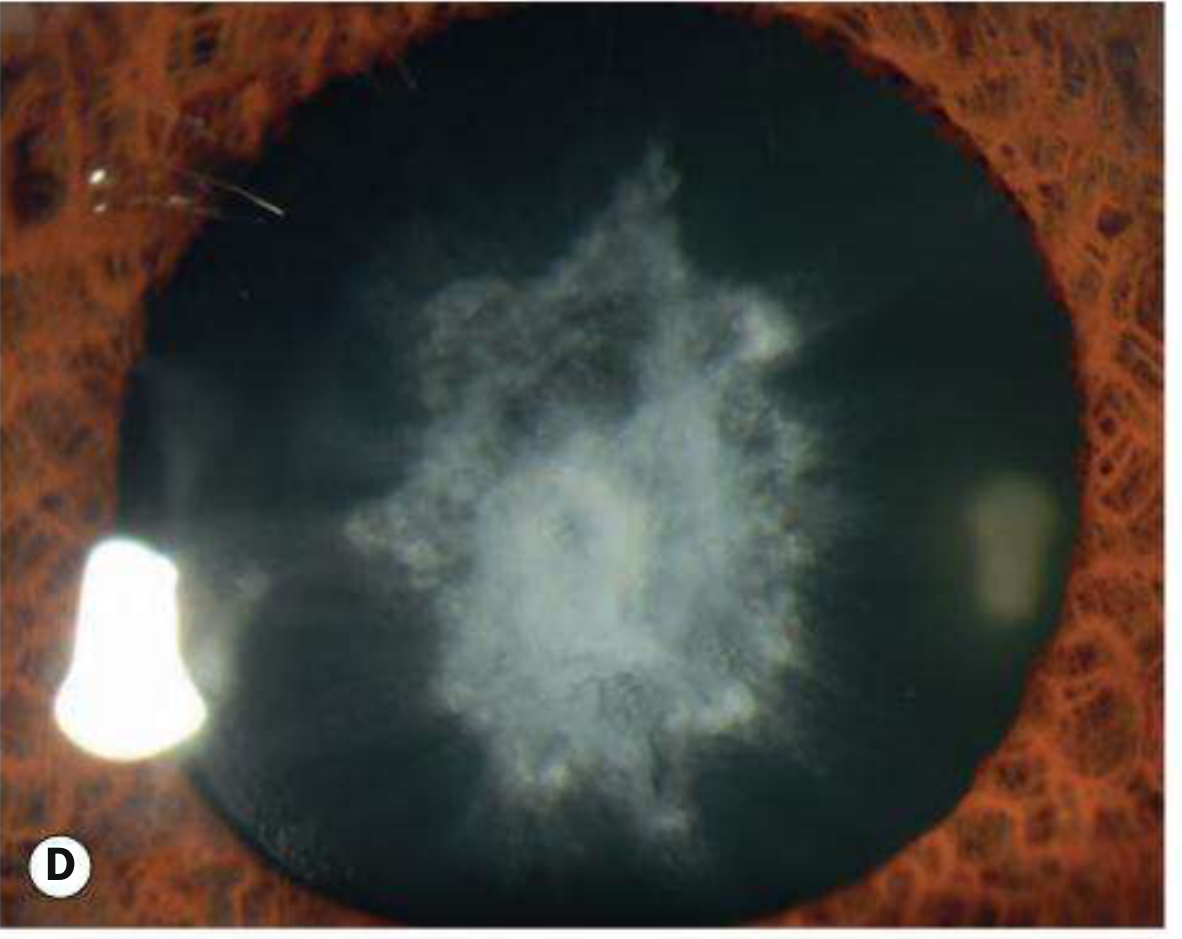
Advanced nuclear cataract as seen by retroillumination - dense central opacity against dark pupil background.
On slit lamp examination (Pfenninger's Procedures, p. 3608):
- The slit beam passes through: anterior capsule → anterior cortex → nucleus → posterior cortex → posterior capsule
- Cortical cataracts: spoke-like opacities from lens equator
- Nuclear cataracts: yellow/amber central hue
- PSC: clustered punctate vacuoles, best seen on retroillumination
Retroillumination technique: Slit beam directed parallel to the visual axis nasally or temporally; lens opacities appear dark against the red reflex from the retina.
Symptoms
- Gradual, painless decrease in vision
- Glare (especially PSC and cortical types)
- Monocular diplopia or polyopia
- Altered colour perception (yellowing in nuclear cataracts)
- "Second sight" - temporary improvement in near vision (nuclear myopia)
- Difficulty with night driving
Systemic/Risk Factor Associations
| Condition | Cataract Type |
|---|---|
| Diabetes mellitus | Snowflake (osmotic) or premature nuclear |
| Corticosteroid use | Posterior subcapsular |
| Galactosaemia | Osmotic (oil-droplet/nuclear) |
| Hypoparathyroidism | Subcapsular |
| Myotonic dystrophy | Christmas tree / PSC |
| Wilson disease | Sunflower cataract |
| Ionizing radiation | Posterior subcapsular |
| Atopic dermatitis | Anterior subcapsular shield cataract |
| Marfan syndrome | Lens subluxation (upward), not cataract per se |
Investigations / Workup
- Visual acuity - Snellen chart
- Slit lamp biomicroscopy - type and density of opacity
- Retroillumination - best for PSC
- Glare testing - functional impact assessment
- Dilated fundus examination - to rule out co-existing retinal pathology that would limit visual recovery post-surgery
- Biometry (pre-operatively):
- Keratometry - corneal curvature in dioptres
- A-scan ultrasonography or optical coherence biometry (partial coherence interferometry) - axial length measurement
- IOL power calculated using formulae (SRK/T, Holladay, Barrett Universal II, etc.)
Management
Conservative
- Updated spectacle correction for early cataracts (myopic shift in nuclear cataract)
- Anti-glare glasses
- No proven medical therapy to halt progression
Surgical Indications
- Visual: opacity sufficient to impair daily activities (primary indication)
- Medical: phacolytic glaucoma, phacomorphic glaucoma, cataract preventing fundus monitoring/treatment
- Clear lens exchange for refractive error management
Surgical Techniques
Phacoemulsification (Gold Standard)
- Ultrasonic fragmentation and aspiration of the lens nucleus through a small (~2.4-2.8 mm) self-sealing corneal incision
- Followed by foldable IOL implantation into the capsular bag
- No sutures required; rapid recovery
- Risk of intraoperative floppy iris syndrome with systemic alpha-blockers (e.g. tamsulosin)
Manual Small Incision Cataract Surgery (MSICS)
- Variant of extracapsular extraction (ECCE) used in resource-limited settings
- Nucleus expressed intact through a larger but self-sealing scleral tunnel incision
- No phaco machine needed; good visual outcomes; widely used in India
Extracapsular Cataract Extraction (ECCE)
- Larger limbal incision; requires sutures; more astigmatism
- Less common now; still used for very dense (brunescent) nuclei
Intracapsular Cataract Extraction (ICCE)
- Entire lens including capsule removed; largely obsolete
- No capsular support for posterior chamber IOL
Intraocular Lens (IOL) Types
- Monofocal IOL - standard; corrects for one distance (usually distance)
- Toric IOL - corrects pre-existing corneal astigmatism
- Multifocal/bifocal IOL - provides range of focal distances; higher dysphotopsia rate
- Accommodative IOL - attempts to mimic accommodation (limited clinical effect)
- Light-adjustable IOL - refractive power adjusted post-implantation using UV light
Sharp/square-edged optics are preferred as they significantly reduce posterior capsular opacification (PCO).
Complications of Cataract Surgery
| Severity | Complication |
|---|---|
| Common, mild | IOP spike, iridocyclitis, PCO (~20-30% within 2-5 years), periocular ecchymosis |
| Moderate-severe | Posterior capsular rupture + vitreous loss (~1%), dropped nucleus (0.2%), cystoid macular oedema, corneal decompensation, retinal detachment (<1%), IOL dislocation |
| Rare, serious | Endophthalmitis (0.1%), suprachoroidal haemorrhage (0.04%) |
Posterior Capsular Opacification (PCO) - "after-cataract" - residual/regenerating lens epithelial cells proliferate across the posterior capsule. Treated effectively with Nd:YAG laser posterior capsulotomy.
Epidemiology / Public Health
- Senile cataract is the most common cause of blindness in India and worldwide
- In India, cataract occurs ~10 years earlier than in Europe/America - Park's Textbook of Preventive & Social Medicine
- The "National Programme for Control of Blindness" targets cataract surgical rate (CSR) as a key metric
- Cataract surgical coverage remains suboptimal in Indigenous populations and resource-poor settings (BMJ Open Ophthalmol, 2025)
Sources: Kanski's Clinical Ophthalmology (10th ed., Ch. 10); Adams & Victor's Principles of Neurology (12th ed.); Pfenninger & Fowler's Procedures for Primary Care; Park's Textbook of Preventive & Social Medicine; Goldman-Cecil Medicine
Senile cataract Give in short for surgery subject bhms exam
Here's a concise exam-ready answer for BHMS Surgery:
Senile Cataract
Definition
Opacity of the crystalline lens occurring due to aging (usually after 50 years).
Etiology / Risk Factors
- Old age (most common)
- UV light exposure
- Diabetes mellitus
- Malnutrition
- Smoking, dehydration
Types (Morphological)
| Type | Feature |
|---|---|
| Nuclear | Central yellowing/browning; causes myopia ("second sight") |
| Cortical | Spoke-like/wedge opacities from periphery |
| Posterior Subcapsular (PSC) | Most visually disabling; causes glare; worst in bright light |
Stages
| Stage | Key Feature |
|---|---|
| Incipient | Early opacity; vision normal |
| Immature | Partial opacity; iris shadow present |
| Mature | Complete white opacity; iris shadow absent; no red reflex |
| Hypermature | Liquefied cortex; nucleus sinks (Morgagnian cataract); risk of phacolytic glaucoma |
Iris shadow test: In immature cataract - iris casts a shadow on the lens (oblique illumination). In mature cataract - no shadow (lens fully opaque).
Symptoms
- Gradual, painless diminution of vision
- Glare / photophobia
- Monocular diplopia
- "Second sight" (nuclear type - myopic shift)
- Altered colour perception
Diagnosis
- Slit lamp biomicroscopy
- Retroillumination (best for PSC)
- Fundus examination (dilated)
- Biometry (pre-op: keratometry + axial length for IOL power)
Treatment
Surgical (only definitive treatment)
Indications: Visual impairment affecting daily life; phacolytic/phacomorphic glaucoma
Methods:
-
Phacoemulsification - Gold standard
- Ultrasound breaks up nucleus; aspirated through 2.4-3 mm incision
- Foldable IOL implanted in capsular bag
- No sutures; rapid recovery
-
MSICS (Manual Small Incision Cataract Surgery)
- Popular in India; no phaco machine needed
- Good outcomes; cost-effective
-
ECCE (Extracapsular Cataract Extraction)
- Larger incision; sutures needed
- Used for very hard (brunescent) nuclei
-
ICCE (Intracapsular) - Obsolete
Complications of Surgery
- PCO (Posterior Capsular Opacification / "after-cataract") - treated by Nd:YAG laser
- Endophthalmitis (rare, serious)
- Cystoid macular oedema
- Posterior capsule rupture
- Retinal detachment
Important Exam Points
- Mature cataract = no iris shadow, no red reflex, white pupil (leukocoria)
- Hypermature = risk of phacolytic glaucoma (lens proteins leak out → macrophage blockage of trabecular meshwork)
- "Second sight" = nuclear myopia (patient reads without glasses temporarily)
- PSC = worst glare; worst in bright light / near work
- Morgagnian cataract = liquefied cortex with sunken brown nucleus
This is a shared conversation. Sign in to Orris to start your own chat.