Deltoid ligament
Reading File
Finding Sources
Finding Sources
Searching the Web
deltoid ligament anatomy function layers clinical significance
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a thorough response:
Deltoid Ligament (Medial Ligament of the Ankle)
Overview
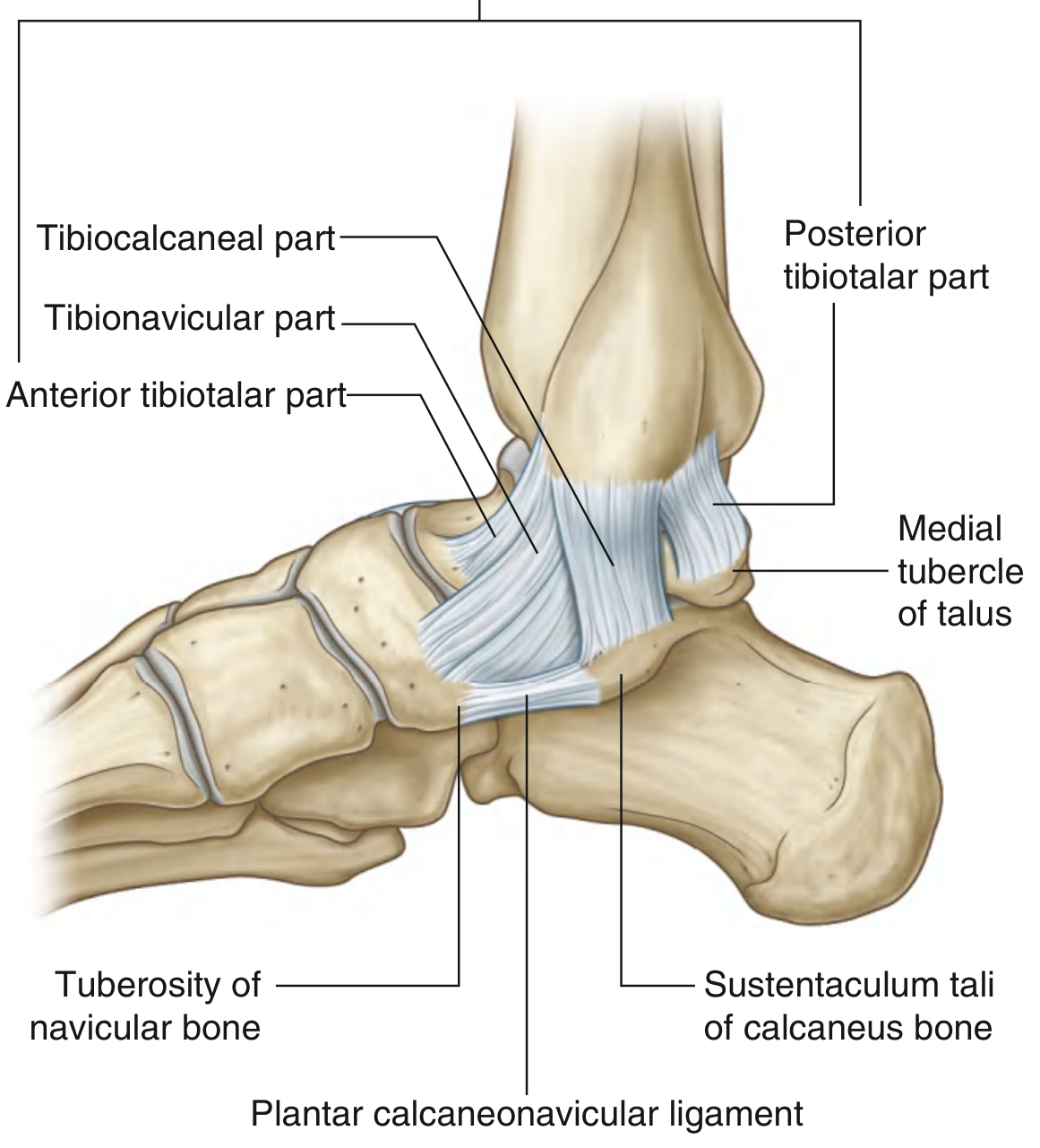
The deltoid ligament is the primary stabilizing structure on the medial side of the ankle. It is large, strong, and triangular in shape. Its apex attaches proximally to the medial malleolus, and its broad base fans out inferiorly to attach across a line extending from the navicular bone anteriorly to the medial tubercle of the talus posteriorly.
Layers and Components
The deltoid ligament is classically divided into two layers - superficial and deep - with a total of five components (per Campbell's Operative Orthopaedics) or described with slightly varying nomenclature across sources:
Deep Layer (intraarticular, extrasynovial - bridges tibiotalar joint only)
| Component | Origin | Insertion | Function |
|---|---|---|---|
| Deep anterior tibiotalar | Intercollicular groove + anterior colliculus | Medial surface of talus | Resists anterior talar translation |
| Deep posterior tibiotalar | Posterior colliculus + intercollicular groove | Medial surface of talus (posterolateral course) | Primary stabilizer - resists lateral talar translation and external rotation |
The posterior deep tibiotalar ligament is the strongest component of the entire deltoid complex and the most important stabilizer of the talus within the ankle mortise.
Superficial Layer (bridges both tibiotalar and subtalar joints)
| Component | Origin | Insertion | Function |
|---|---|---|---|
| Tibionavicular | Anterior colliculus of medial malleolus | Dorsomedial navicular + spring ligament | Resists valgus/eversion |
| Tibiocalcaneal | Medial malleolus (middle portion) | Sustentaculum tali of calcaneus | Resists valgus tilt |
| Superficial posterior tibiotalar | Distal medial malleolus | Medial tubercle of talus | Resists valgus and external rotation |
Some descriptions (Milner and Soames) also include a tibiospring component connecting to the spring (plantar calcaneonavicular) ligament as part of the superficial layer.
Key Functions
- Primary role: Stabilizes the medial ankle during the stance phase of gait
- Deep layer: Primarily resists lateral talar translation and external rotation of the talus
- Superficial layer: Primarily resists valgus/eversion forces (talar tilt)
- Both layers act as secondary restraints against anterior talar translation
- The deltoid works in concert with the spring (plantar calcaneonavicular) ligament to support the talar head and maintain the medial longitudinal arch
Clinical Relevance
Injury Patterns
- Isolated deltoid ligament ruptures are rare - they far more commonly occur alongside lateral malleolar fractures, syndesmotic injuries, or lateral ligament tears
- Of patients with lateral ankle instability, 72% have a concurrent deltoid injury, and 43% have injury to both deep and superficial components - Campbell's Operative Orthopaedics 15th Ed, p. 5242
- Incidence of deltoid lesions increases significantly when the ATFL is completely ruptured
- An avulsed deltoid ligament can become entrapped between the medial malleolus and the talus, blocking fracture reduction
Diagnosis
- Medial ankle tenderness and swelling after inversion/external rotation injury
- Stress X-rays (valgus/varus, anterior drawer): widening of the medial clear space on mortise view suggests deep deltoid incompetence
- MRI: gold standard for determining extent - distinguishes partial from complete tears and identifies which layers are involved
- The medial clear space on mortise view should be ≤4 mm and equal to the superior tibiotalar joint space when the deltoid is intact
Treatment
Isolated partial rupture:
- Conservative - immobilization in below-knee non-weight-bearing cast, then functional rehabilitation (prolonged compared to lateral sprains)
Isolated complete disruption (rare):
- Below-knee non-weight-bearing cast for 6 weeks, then progressive weight-bearing
Acute rupture with associated fracture or instability:
- Surgical repair is generally recommended in active patients, especially when MRI confirms complete disruption or mortise imaging shows talar shift
- Primary repair uses suture anchor re-attachment to the medial malleolus, imbrication of tibionavicular and tibiocalcaneal bands
- Note: lateral malleolar fixation alone may restore mortise stability even if the deltoid is not repaired in some cases
Chronic insufficiency / reconstruction:
- Ligament reconstruction techniques (analogous to Brostrom for the lateral side) are indicated when primary repair is no longer possible
- Post-operative protocol involves short-leg casting in plantarflexion/inversion for 5 weeks, then boot with arch support, physical therapy at 8 weeks, return to impact activity at 16 weeks
Key Points Summary
| Feature | Detail |
|---|---|
| Shape | Triangular, broad-based fan |
| Proximal attachment | Medial malleolus (both colliculi, intercollicular groove) |
| Distal attachments | Navicular, spring ligament, sustentaculum tali, medial talus |
| Layers | Superficial (3 bands) + Deep (2 bands) |
| Strongest component | Deep posterior tibiotalar |
| Primary function | Resist lateral talar translation + eversion/valgus |
| Most common injury context | Associated with fibular fracture or syndesmotic injury |
| Imaging of choice | MRI for ligament; mortise X-ray for instability |
Sources: Gray's Anatomy for Students, p. 5229-5239 | Campbell's Operative Orthopaedics 15th Ed, p. 5087-5102, 5242-5253 | Rockwood and Green's Fractures in Adults 10th Ed, p. 1757 | Miller's Review of Orthopaedics 9th Ed, p. 374-383 | Imaging Anatomy: Bones, Joints, Vessels and Nerves, p. 579-588
Give in this format for all pg answers
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Searching the Web
deltoid ligament injury classification recent advances 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading Web Page
deltoid ligament classification grading
I now have all the content needed. Here is the full PG-format answer:
DELTOID LIGAMENT
1. Introduction
The deltoid ligament (medial ligament of the ankle) is the primary stabilizing structure on the medial side of the talocrural joint. It is a large, flat, strong, triangular-shaped ligament whose apex attaches to the medial malleolus and whose broad base fans inferiorly to span multiple tarsal bones. Unlike the lateral ligament complex (three separate bands), the deltoid is a continuous but multi-component structure. It functions as the primary ankle stabilizer during the stance phase of gait and prevents lateral talar translation, external rotation, and valgus tilt of the talus.
2. History
- Described as early as the 19th century as part of classical ankle anatomy
- Lauge-Hansen (1950) - classified ankle ligament injuries based on mechanism; described deltoid involvement in supination-external rotation (SER) and pronation-abduction (PA) patterns
- Danis-Weber classification - indirectly accounts for deltoid status through fracture level
- Milner and Soames - provided the most widely used modern sub-component naming of the deltoid (tibionavicular, tibiospring, tibiocalcaneal, superficial + deep posterior tibiotalar)
- Deland - described peroneus longus autograft reconstruction for chronic deltoid insufficiency
- Jeng, Bluman, Myerson (2011) - described minimally invasive deltoid reconstruction for Stage IV flatfoot
3. Anatomy
Shape and Attachments
- Shape: Triangular, broad-based fan
- Proximal attachment: Apex to the medial malleolus (both anterior and posterior colliculi and the intercollicular groove)
- Distal attachments: Tuberosity of the navicular, plantar calcaneonavicular (spring) ligament, sustentaculum tali of calcaneus, medial surface of talus (anterior and posterior)
Two-Layer Structure (5 components total)
DEEP LAYER - intraarticular, extrasynovial; bridges tibiotalar joint only
| Component | Origin | Insertion |
|---|---|---|
| Deep anterior tibiotalar | Intercollicular groove + anterior colliculus | Medial surface of talus |
| Deep posterior tibiotalar | Posterior colliculus + intercollicular groove | Medial surface of talus (posterolateral course) |
- The deep posterior tibiotalar ligament is the strongest component of the entire deltoid complex and the principal stabilizer of the talus in the mortise
SUPERFICIAL LAYER - bridges both tibiotalar and subtalar joints
| Component | Origin | Insertion |
|---|---|---|
| Tibionavicular | Anterior colliculus | Dorsomedial navicular + spring ligament |
| Tibiocalcaneal | Distal medial malleolus | Sustentaculum tali of calcaneus |
| Superficial posterior tibiotalar | Distal medial malleolus | Medial tubercle of talus |
Some authors include a tibiospring component (to the spring ligament) as a 4th superficial band.
Functions
- Deep layer: Primarily resists lateral talar translation and external rotation of the talus
- Superficial layer: Primarily resists valgus/eversion forces (talar tilt)
- Both layers: Secondary restraints against anterior talar translation
- Works in concert with the spring ligament to support the talar head and medial longitudinal arch
4. Etiology (of Injury)
- Eversion injury - most common mechanism (forced eversion/pronation-abduction)
- External rotation - supination-external rotation (SER) pattern per Lauge-Hansen; the sequence involves anterior capsule tear then deltoid disruption
- Associated fractures - fibular fracture, bimalleolar / trimalleolar fractures
- Syndesmotic injury - frequently co-existent
- Chronic insufficiency - Stage IV adult-acquired flatfoot deformity (posterior tibial tendon dysfunction with valgus talar tilt)
- Iatrogenic - excessive eversion in ankle arthroplasty or hindfoot reconstruction
5. Mechanism of Injury
Lauge-Hansen Framework (relevant patterns):
Supination-External Rotation (SER) - most common (60-70% of ankle fractures)
- Stage 1: Anterior inferior tibiofibular ligament rupture
- Stage 2: Spiral/oblique fibular fracture at/above syndesmosis
- Stage 3: Posterior tibiofibular ligament or posterior malleolus
- Stage 4: Deltoid ligament rupture (or medial malleolus fracture = bimalleolar equivalent)
Pronation-Abduction (PA) / Pronation-External Rotation (PER)
- Stage 1: Deltoid ligament torn first (or medial malleolus avulsion)
- Subsequent stages: syndesmotic injury, high fibular fracture
Biomechanical consequence:
- A 1 mm lateral talar shift reduces the effective tibiotalar weight-bearing area by 20-40%
- A 5 mm lateral shift reduces it by 80%
- This explains why even apparently minor deltoid incompetence has profound biomechanical implications
6. Pathology
- Partial tear (more common) - disruption of individual bands, usually superficial layer
- Complete rupture (rare in isolation) - full thickness disruption of both layers; commonly with fibular fracture or syndesmotic injury
- Avulsion - ligament torn from medial malleolus (proximal) or from tarsal bone attachments (distal); avulsed stump can become entrapped between medial malleolus and talus, blocking mortise reduction
- Chronic attenuation - seen in Stage IV PTTD flatfoot; the deltoid is incompetent, allowing valgus talar tilt even with structurally intact fibrous tissue
Associated with: 72% of patients with lateral ankle instability have deltoid injury; 43% have both deep and superficial layer involvement.
7. Clinical Features
Symptoms
- Medial ankle pain and swelling after eversion/external rotation injury
- Difficulty or inability to bear weight
- Sense of instability (giving way)
Signs
- Tenderness over the medial malleolus and medial ligament complex
- Swelling and ecchymosis medially (hematoma suggests significant tear)
- Note: Medial tenderness alone does NOT reliably predict deep deltoid rupture - no statistically significant relationship has been demonstrated between medial tenderness and deep deltoid disruption in the setting of lateral malleolar fracture
- In chronic insufficiency: valgus hindfoot alignment, medial arch collapse, forefoot abduction
Special Tests
- Eversion stress test: Pain and gapping medially
- External rotation stress test: Pain with widening of medial clear space
- Always palpate the full length of the fibula to rule out a Maisonneuve fracture (proximal fibular fracture) when medial tenderness is present
8. Investigations
- Plain X-ray (weight-bearing AP, lateral, mortise views) - first line
- Gravity stress radiograph / manual eversion stress - to unmask occult instability
- MRI - gold standard for ligament assessment
- Ultrasound - dynamic assessment, useful for superficial bands
- CT scan - for bony injury characterization, syndesmosis assessment
9. Radiograph
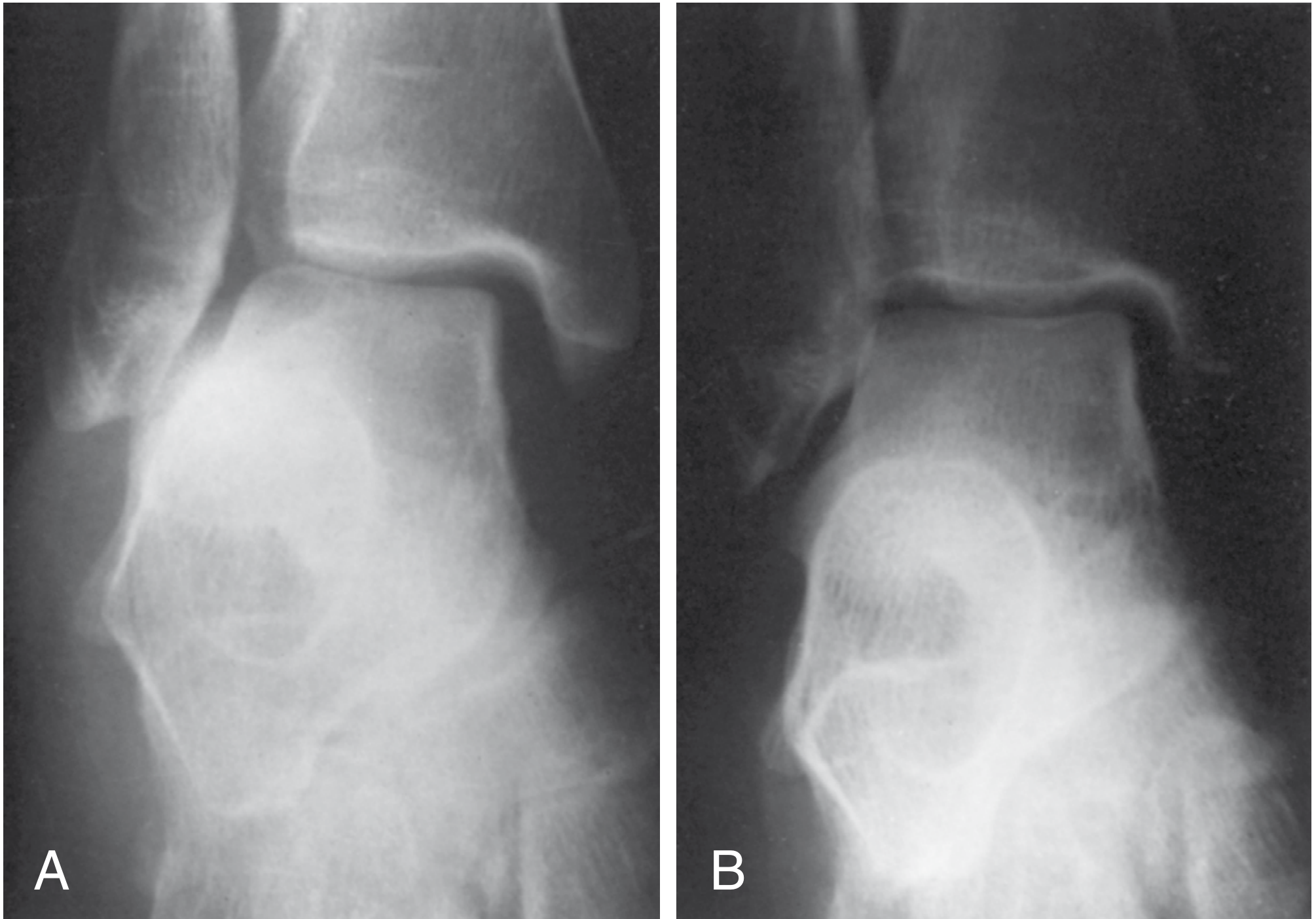
Key Measurements (Mortise View - ankle in neutral dorsiflexion):
- Medial clear space (between medial talus and medial malleolus): Normal ≤ 4 mm
- Medial clear space = Superior joint space: If medial clear space > superior space, suggests deltoid incompetence
- Tibiofibular clear space (on AP view): < 6 mm normal
- Tibiofibular overlap: > 6 mm on AP, > 1 mm on mortise view
Important: Measurement must be on mortise view with ankle in neutral position - plantarflexion allows the narrow part of the talar dome into the mortise, giving a spuriously wide medial space even in a normal ankle.
10. CT Scan
- Not routinely needed for isolated deltoid injury
- Indicated when:
- Syndesmosis injury is suspected (3D CT for tibiofibular relationship)
- Complex fracture pattern with deltoid involvement (trimalleolar, pilon)
- Pre-operative planning for reconstruction
- Assessing for osteochondral lesions of the talus (common co-injury)
- CT may show tibiofibular diastasis not apparent on plain films
11. MRI
- Most accurate investigation for assessing the deltoid ligament
- Axial sequences (with local gradient): Best for deep layers and tibionavicular component
- Coronal sequences: Best for tibiocalcaneal, posterior tibiotalar, and calcaneofibular ligaments; allows complete view and differentiation of superficial vs deep layers
- 3T MRI with 3D reconstruction: High-spatial resolution protocol can produce high-quality images of all ligament components in < 10 minutes (Campbell's, p. 5239-5240)
- MRI findings: Ligament discontinuity, increased T2 signal within the substance (partial tear), fluid surrounding torn ends (complete rupture), periligamentous edema
- MRI is more specific than sensitive for ankle ligament injuries (particularly the CFL)
- Bone bruises occur in significant proportion of ankle sprains; multiple bone bruises suggest multiple ligament injury
12. Classification
A. Sprain Grading (Universal - applied to all ankle ligaments including deltoid)
| Grade | Pathology | Clinical |
|---|---|---|
| Grade I | Ligament stretch, microscopic tears, intact | Mild pain, minimal swelling, full weight-bearing |
| Grade II | Partial macroscopic tear | Moderate pain, swelling, difficulty walking |
| Grade III | Complete rupture | Severe pain, swelling, instability, unable to bear weight |
B. Anatomic Location Classification (Radiopaedia / anatomic):
| Type | Description |
|---|---|
| Type 1 | Proximal tear or avulsion from medial malleolus |
| Type 2 | Mid-substance (interstitial) tear |
| Type 3 | Distal tear or avulsion from tarsal attachment |
C. Lauge-Hansen Classification (mechanism-based, relevant to deltoid stage)
- Describes deltoid injury within the staged sequence of ankle fracture-ligament injuries (SER Stage 4, PA Stage 1, PER Stage 1)
D. In context of Flatfoot (PTTD) - Johnson & Strom / Myerson Staging:
- Stage IV: Deltoid ligament insufficiency with valgus talar tilt added to Stage III deformity - requires deltoid reconstruction as part of treatment
13. Treatment
A. Non-Operative
Indications:
- Grade I and II isolated sprains
- Isolated complete rupture (Grade III) in low-demand patients
- Deltoid tear with lateral malleolar fracture where mortise remains congruent after fibular fixation
Protocol:
- Acute phase (0-2 weeks): RICE (Rest, Ice, Compression, Elevation); non-weight-bearing below-knee cast or boot
- Sub-acute (2-6 weeks): Progressive weight-bearing in boot with arch support; physiotherapy
- Rehabilitation: Proprioceptive training, peroneal strengthening, range of motion; time course longer than lateral sprains
- Serial radiographic monitoring to confirm no loss of mortise congruence
B. Operative
i. Acute Repair - Indications:
- Complete rupture in active/high-demand patient (Grade III)
- Deltoid tear with lateral malleolar fracture + talar shift in mortise (MRI confirmed or stress-positive)
- Deltoid avulsion interposed in joint (blocking reduction)
- Bimalleolar equivalent fractures with confirmed instability
ii. Acute Repair - Technique:
- Curvilinear medial incision over medial malleolus extending to navicular
- Identify disrupted deltoid ligament (usually avulsed from medial malleolus)
- Debride torn edges; create shallow trough on medial malleolus with rongeur to enhance healing
- Place suture anchor in distal medial malleolus
- Repair deltoid in imbricated fashion - approximating tibionavicular and tibiocalcaneal bands to native attachment
- Protect with below-knee cast in 5-10° plantarflexion and inversion
- ORIF of lateral malleolus is performed concurrently
- Note: Many surgeons do NOT routinely repair the deltoid; fibular fixation alone often restores mortise congruence; medial exploration is reserved for cases with persistent wide medial clear space or blocked reduction
iii. Chronic Reconstruction - Indications:
- Chronic deltoid instability with pain/functional limitation
- Stage IV adult-acquired flatfoot (PTTD with deltoid insufficiency)
- Failed conservative management of chronic medial instability
iv. Reconstruction Techniques:
a. Tape suture augmentation (most common, preferred)
- Primary repair with imbrication + suture tape (InternalBrace-type) from medial malleolus to sustentaculum tali
- Guide pin into sustentaculum tali angled 15° plantar to avoid subtalar joint violation
- Suture tape anchored in sustentaculum + medial malleolus; deltoid repaired over the tape
b. Peroneus longus autograft (Deland technique)
- Peroneus longus preferred over peroneus brevis - longer and inserts medially
- Difficult to harvest on plantar surface; requires cadaver practice
c. Minimally invasive allograft (Jeng, Bluman, Myerson 2011 - for Stage IV flatfoot)
- Tibial tunnel: Guidewire parallel to joint surface at physeal scar level; 6.5 mm tunnel, 25 mm deep
- Tendon graft (semitendinosus/hamstring allograft) fixed in tibial tunnel with biotenodesis screw
- Subcutaneous tunnel from tibia to medial malleolus tip
- Talar tunnel: From medial center of tibiotalar rotation to lateral talar neck junction - 5 mm tunnel
- Graft passed medial to lateral through talar tunnel; fixed with interference screw in maximal inversion
- Calcaneal (sustentaculum) arm fixed with biotenodesis screw
- Often combined with medial displacement calcaneal osteotomy and spring ligament repair
d. Hamstring allograft reconstruction - alternative to autograft
Postoperative Protocol:
- Sutures removed at 2 weeks
- Short leg cast in 5° plantarflexion + inversion x 5 weeks
- Boot with orthotic arch support at 5 weeks; weight-bearing as tolerated
- Physiotherapy at 8 weeks; transition to stiff-soled shoe with orthotic
- Impact activity (running) from 16 weeks with carbon insert protection
14. Recent Advances
-
High-resolution 3T MRI with AI-based reconstruction - acceleration protocols producing high-quality ligament and tendon images in < 10 minutes; may lead to more routine MRI use and improved accuracy of deltoid assessment (Campbell's 15th Ed, 2026)
-
Suture tape augmentation (InternalBrace) - biomechanically superior to primary repair alone; allows immediate protected weight-bearing; now the preferred adjunct for both acute repair and chronic reconstruction
-
Arthroscopic-assisted deltoid repair - diagnostic arthroscopy before open repair to assess osteochondral lesions (common co-injury) and confirm ligament pathology; combined arthroscopy + open repair recommended
-
Recognition of deltoid injury prevalence - recent evidence shows deltoid injuries are far more common than previously thought; 72% of lateral ankle instability cases have concurrent deltoid involvement; systematic MRI assessment is being advocated
-
Minimally invasive reconstruction techniques - evolving graft-based reconstructions (allograft semitendinosus, peroneus longus) now allow anatomic restoration of both deep and superficial components; superior to non-anatomic tenodesis procedures
-
Deltoid repair vs. syndesmotic fixation debate - comparative studies (2015 onwards) show similar functional outcomes with deltoid repair + PITFL repair versus trans-syndesmotic fixation in bimalleolar equivalent fractures; this is shifting practice toward deltoid repair in selected cases
-
Role in flatfoot surgery - increased recognition that Stage IV PTTD requires deltoid reconstruction rather than ignoring medial instability; failure to address deltoid in flatfoot correction leads to recurrent valgus tilt
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 (pp. 5087-5102, 5239-5253, 5542-5660, 6541-6605) | Rockwood and Green's Fractures in Adults 10th Ed 2025 (p. 1757) | Gray's Anatomy for Students (pp. 5229-5239) | Miller's Review of Orthopaedics 9th Ed (pp. 374-383) | Imaging Anatomy Vol. 3: Bones, Joints, Vessels and Nerves (pp. 579-596)
Create a summary document with anatomy diagrams and classification tables
Reading File
Running Command
Writing File
Create a summary document with anatomy diagrams and classification tables
Reading File
Running Command
Writing File
Running Command
Writing File
Running Command
Running Command
Running Command
Your document is ready (3.3 MB, all XML validated):
Deltoid Ligament PG Summary
Word Document · DOCX
What's inside the document:
| Section | Content |
|---|---|
| Cover page | Title, subtitle, anatomy diagram (Fig. 1), source list |
| 1. Introduction | Overview paragraph |
| 2. Anatomy | 5-component table (colour-coded deep/superficial), functional layer table, large anatomy diagram (Fig. 2) |
| 3. Etiology | Mechanism bullet list |
| 4. Mechanism | Lauge-Hansen SER classification table, biomechanical key facts |
| 5. Pathology | Tear types, entrapment, prevalence note box |
| 6. Clinical Features | Symptoms + signs, important clinical pitfall note |
| 7. Investigations | Radiological measurements table, stress X-ray example (Fig. 3) |
| 8–9. CT / MRI | Indications, MRI sequence guide, MRI image (Fig. 4) |
| 10. Classification | Sprain grading table (colour-coded I/II/III), anatomic location table, Lauge-Hansen, Myerson Stage IV |
| 11. Treatment | Scenario-based treatment table, non-op protocol, acute repair steps, chronic reconstruction techniques + postop protocol |
| 12. Recent Advances | 6-point table |
The document uses your PG format structure, with dark blue section headers, colour-coded tables, embedded textbook images, running header/footer, and page numbers throughout.
Generate in pdf format
Running Command
Running Command
Running Command
Running Command
Done. Your PDF is ready (796 KB):
Deltoid Ligament PG Summary
PDF Document · PDF
This is a direct conversion of the full Word document - all anatomy diagrams, colour-coded classification tables, section headers, running header/footer, and page numbers are preserved in the PDF.
This is a shared conversation. Sign in to Orris to start your own chat.