CXR findings in pulmonary edema
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have rich material from multiple authoritative textbooks and several real CXR images. Let me compile the comprehensive answer.
CXR Findings in Pulmonary Edema
The plain chest radiograph remains the most practical and widely used tool for detecting pulmonary edema. Findings depend on the stage of edema (interstitial vs. alveolar) and the underlying etiology (cardiogenic vs. non-cardiogenic). - Murray & Nadel's Textbook of Respiratory Medicine
Sequence of Radiographic Changes (Stage-Based)
CXR findings follow a predictable progression as pulmonary capillary wedge pressure (PCWP) rises:
| PCWP (mmHg) | Stage | Key CXR Findings |
|---|---|---|
| < 12 | Normal | Normal vascular pattern |
| 12-18 | Vascular redistribution | Cephalization / upper lobe vascular diversion |
| 18-25 | Interstitial edema | Kerley lines, peribronchial cuffing, perihilar haze, septal thickening |
| > 25 | Alveolar edema | Bilateral airspace opacities, bat-wing/butterfly pattern, air bronchograms |
Detailed Findings
1. Cardiomegaly
- Cardiothoracic ratio > 0.5 on a PA film.
- The most sensitive individual CXR sign for AHF (74.7% sensitive, negative LR 0.43). - Rosen's Emergency Medicine
- In acute severe cases (e.g., acute mitral regurgitation), the heart may be normal in size despite florid alveolar edema.
2. Vascular Redistribution / Cephalization
- Normally, lower lobe vessels are larger than upper lobe vessels in the erect patient.
- In elevated PCWP, upper lobe veins dilate and become equal to or larger than lower lobe vessels ("upper lobe blood diversion").
- This is an early, subtle finding reflecting early elevation of pulmonary venous pressure.
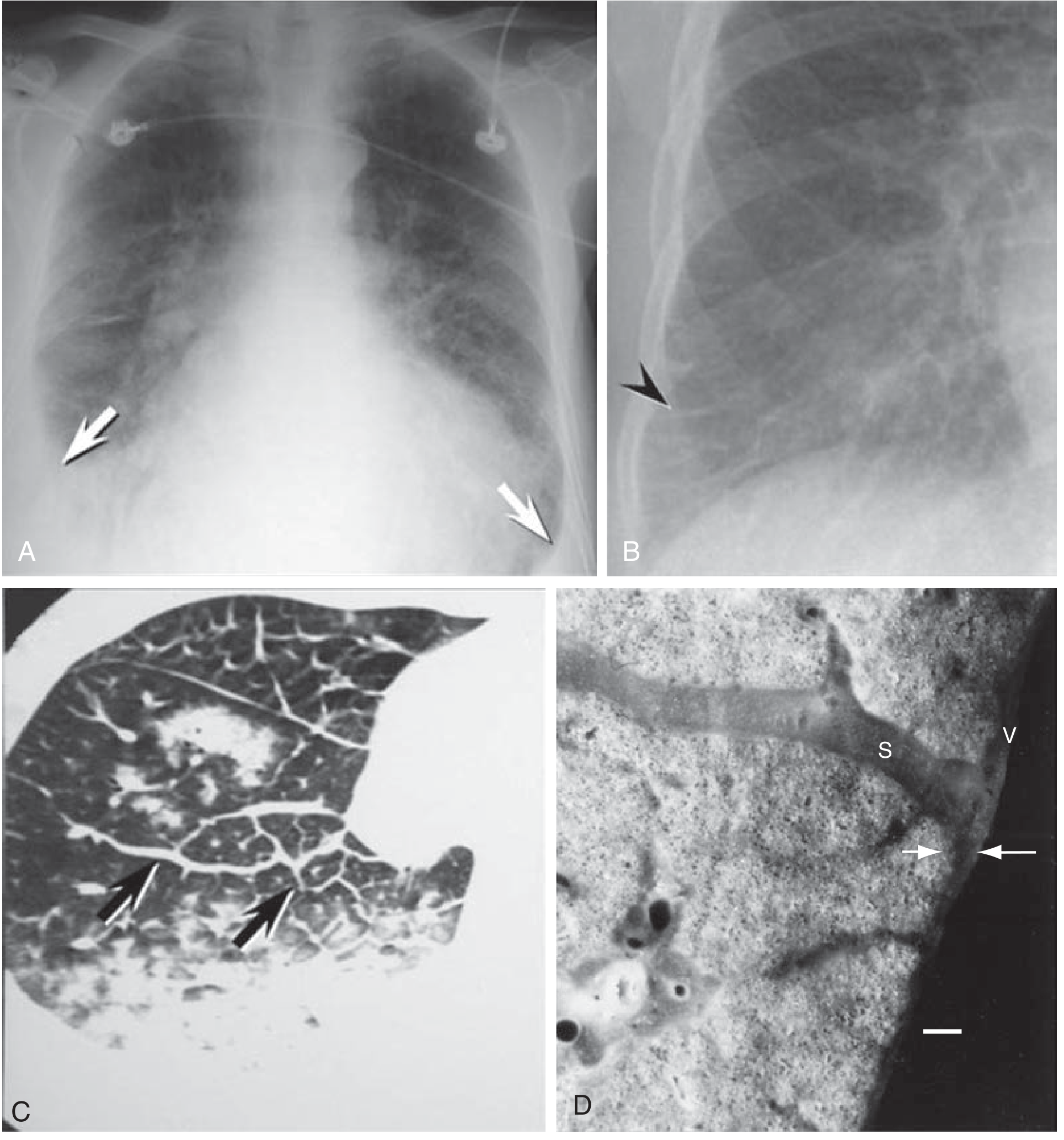
3. Kerley Lines
Three types, all representing thickened interlobular septa filled with edema fluid:
- Kerley B lines - Most common. Short (1-2 cm), horizontal, non-branching lines at the lung periphery, particularly the costophrenic angles. They are perpendicular to the pleural surface.
- Kerley A lines - Longer (4-6 cm) linear opacities extending obliquely from the hilum toward the periphery, representing lymphatic engorgement in deeper septa.
- Kerley C lines - Fine reticular pattern at the lung base, representing B-lines seen en face.
The presence of Kerley B-lines strongly suggests AHF in the context of undifferentiated dyspnea. - Rosen's Emergency Medicine
4. Peribronchial Cuffing
- Loss of sharp definition of bronchial walls seen end-on near the hila ("doughnut sign").
- Results from fluid accumulation in the peribronchial and perivascular interstitium.
- Also called perivascular haziness when vessels lose their sharp margins.
5. Perihilar Haze
- Increased opacity radiating from both hila, often bilaterally symmetric.
- Indicates interstitial edema concentrated in the bronchovascular bundles.
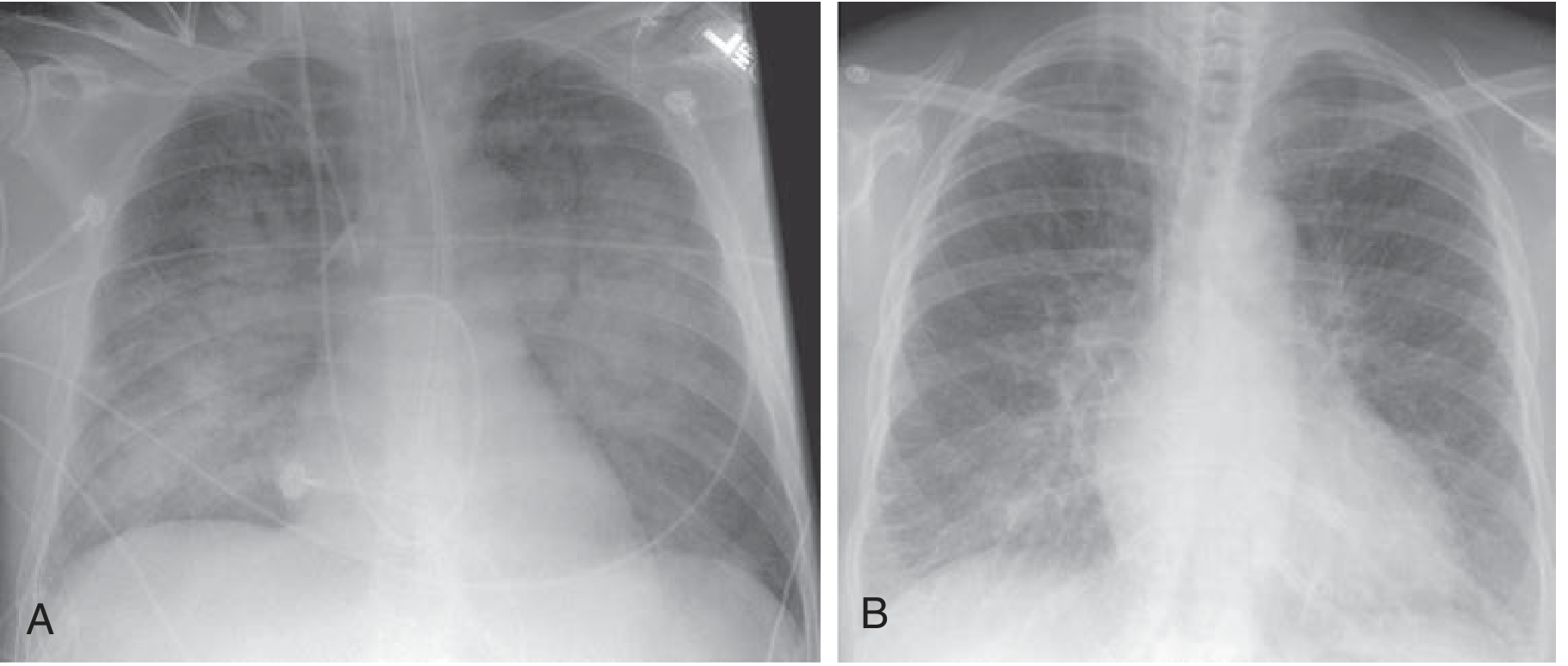
6. Bat-Wing / Butterfly Pattern
- Bilateral, confluent, perihilar airspace opacification that spares the periphery, creating the classic "bat-wing" appearance.
- Represents frank alveolar flooding with PCWP typically > 25 mmHg.
- Typical of cardiogenic pulmonary edema; generally absent in high-altitude pulmonary edema (HAPE) and non-cardiogenic causes. - Rosen's Emergency Medicine
7. Air Bronchograms
- Air-filled bronchi made visible against the background of fluid-filled alveoli.
- Seen in severe alveolar edema; also present in pneumonia, atelectasis, and ARDS.
8. Pleural Effusions
- Bilateral (usually right > left or symmetric) transudate.
- Unilateral or markedly asymmetric effusions should prompt further investigation (other diagnoses or additional pathology). - Murray & Nadel's
- Obliterates the costophrenic angle when > 200-300 mL.
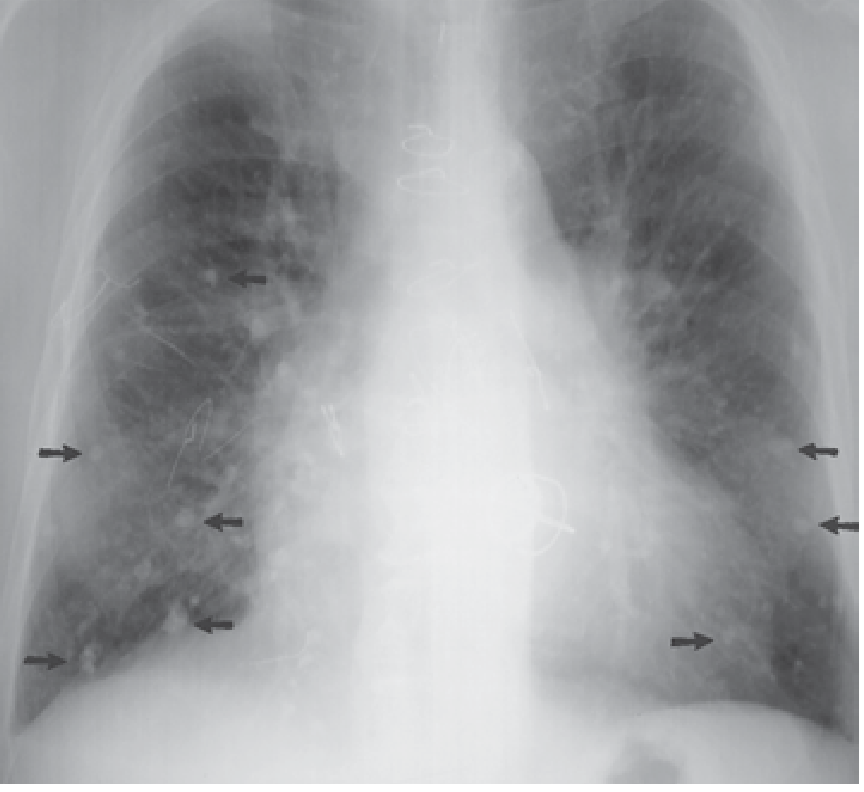
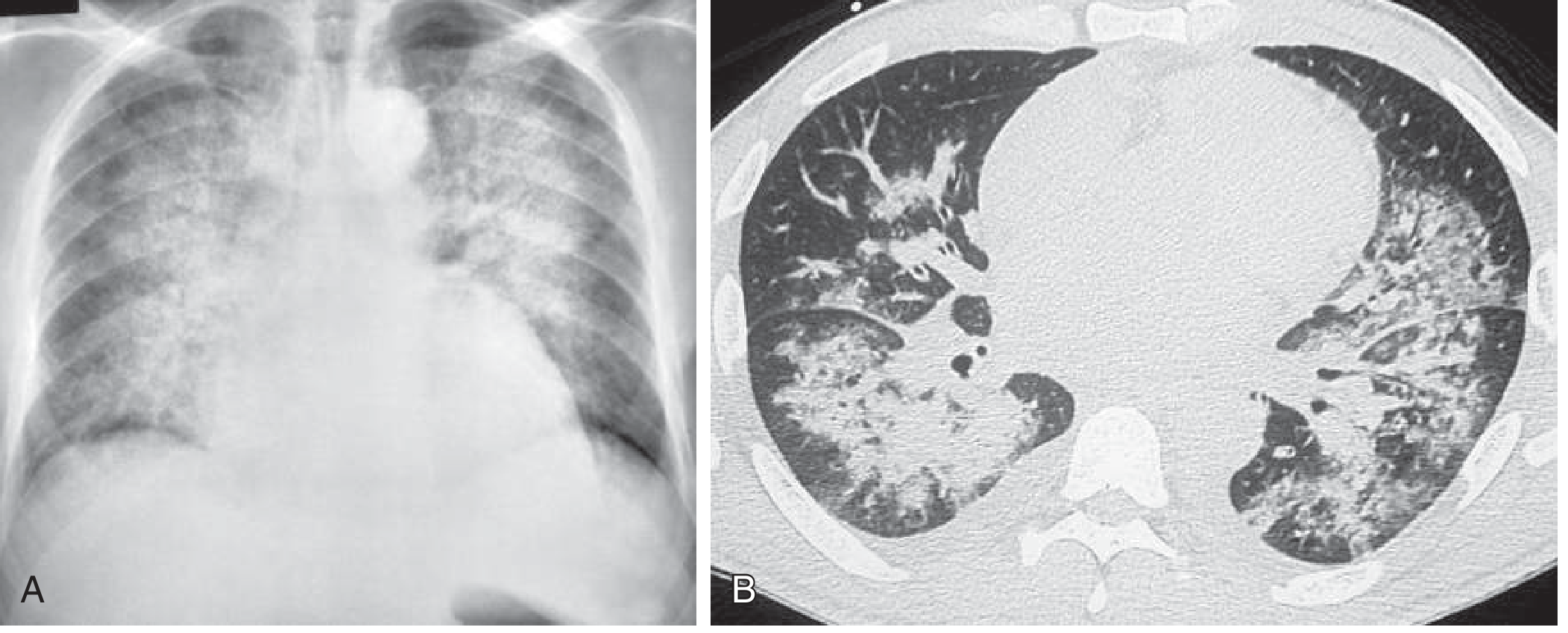
9. Alveolar Opacities / Consolidation
- Patchy, irregular, or confluent increases in lung density obscuring vascular markings.
- Represents flooded alveoli; may be asymmetric or change rapidly.
Reticular Pattern (Interstitial Phase)
Before alveolar flooding, a fine reticular (net-like) pattern develops, most prominent at the lung bases. This is caused by fluid accumulation within interlobular septa. Acute-onset reticular pattern in the correct clinical setting is highly suggestive of interstitial edema (e.g., left-sided heart failure, fluid overload). - Goldman-Cecil Medicine
Diagnostic Performance of CXR Findings (for AHF)
| Finding | Sensitivity | Specificity | +LR | -LR |
|---|---|---|---|---|
| Cardiomegaly | 74.7% | ~70% | ~2.5 | 0.43 |
| Pulmonary edema | 56.9% | ~90% | ~5.5 | 0.48 |
| Cephalization | ~60% | ~75% | ~2.5 | ~0.55 |
| Kerley B lines | ~40% | ~96% | ~10 | ~0.6 |
Key point: A normal CXR does not rule out AHF unless pretest probability is very low. CXR has high positive predictive value but poor sensitivity. - Rosen's Emergency Medicine
Cardiogenic vs. Non-Cardiogenic Pulmonary Edema on CXR
| Feature | Cardiogenic | Non-Cardiogenic (ARDS/HAPE) |
|---|---|---|
| Cardiomegaly | Present | Usually absent |
| Bat-wing distribution | Classic | Absent / peripheral |
| Kerley B lines | Present | Absent (HAPE) |
| Pleural effusions | Common (bilateral) | Rare |
| Air space distribution | Perihilar predominance | Peripheral / diffuse |
| Vascular redistribution | Present | Absent |
| Response to diuresis | Rapid clearing | Slow |
In HAPE specifically, CXR shows patchy alveolar infiltrates, often right mid-lung predominance in early stages, with bilateral involvement in advanced cases - without the bat-wing pattern, Kerley B lines, or cardiomegaly typical of cardiogenic edema. - Rosen's Emergency Medicine (HAPE section)
Summary Mnemonic: "ABC DKPV"
- A - Airspace opacities (alveolar phase)
- B - Bat-wing distribution (perihilar)
- C - Cardiomegaly
- D - Dilation of upper lobe vessels (cephalization)
- K - Kerley lines (A, B, C)
- P - Pleural effusions (bilateral) + Peribronchial cuffing
- V - Vascular haziness (perihilar haze)
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Rosen's Emergency Medicine | Goldman-Cecil Medicine | Fuster & Hurst's The Heart, 15th Edition | Roberts & Hedges' Clinical Procedures in Emergency Medicine
Pcwp?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive material. Here is a full answer on PCWP:
Pulmonary Capillary Wedge Pressure (PCWP)
Also called Pulmonary Artery Occlusion Pressure (PAOP) or Pulmonary Artery Wedge Pressure (PAWP).
What Is It?
PCWP is the pressure recorded when a balloon-tipped, flow-directed Swan-Ganz (pulmonary artery) catheter is advanced until it occludes a small branch of the pulmonary artery. With forward flow blocked, the catheter tip "looks back" through a static column of blood across the pulmonary capillaries, pulmonary veins, and into the left atrium. This makes PCWP an indirect, backpressure estimate of:
PCWP ≈ Left Atrial Pressure (LAP) ≈ Left Ventricular End-Diastolic Pressure (LVEDP)
...assuming no obstruction between the tip and the LV (e.g., no mitral stenosis). - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Normal Values
| Parameter | Normal Value |
|---|---|
| PCWP | 6-12 mmHg (upper limit ≤15 mmHg) |
| Mean PA pressure (mPAP) | < 21 mmHg |
| CVP / Right atrial pressure | 0-8 mmHg |
| Cardiac output | 4-6 L/min |
| PVR | < 3 Wood units |
A PCWP > 15 mmHg is considered elevated and suggests post-capillary (left-sided) disease. - Fishman's Pulmonary Diseases and Disorders
How Is It Measured?
A Swan-Ganz catheter is inserted via a central vein (internal jugular, subclavian, or femoral) and floated forward by inflating a small balloon at its tip, which is carried by blood flow through the right heart chambers into the pulmonary artery.
The characteristic pressure waveforms guide catheter placement:
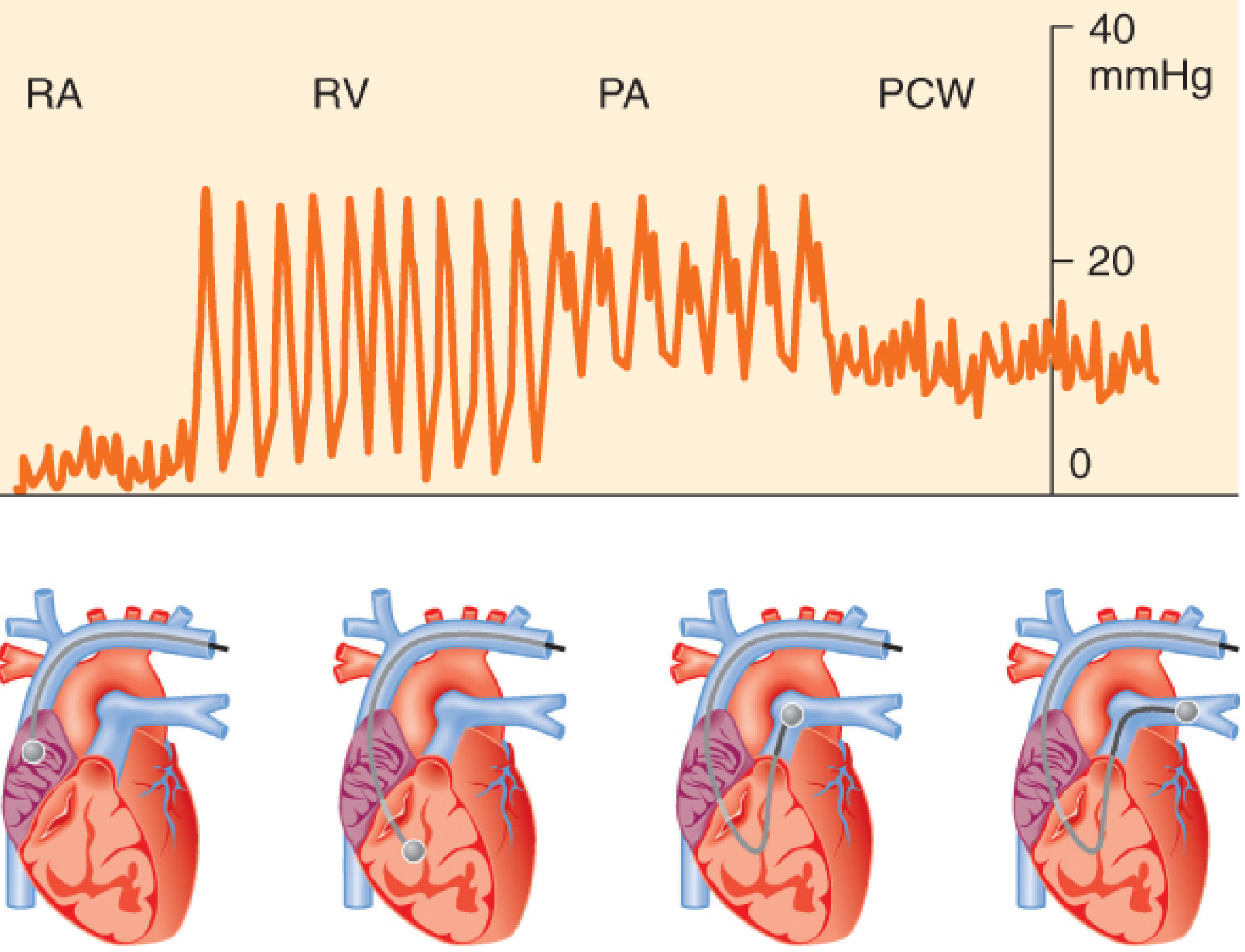
Once the balloon is wedged (~50 cm mark), the wedge tracing shows a, c, and v waves corresponding to atrial contraction, mitral valve closure, and ventricular systole/atrial filling respectively. The mean of this tracing = PCWP.
PCWP and Pulmonary Edema (Clinical Thresholds)
| PCWP | Clinical State |
|---|---|
| < 12 mmHg | Normal |
| 12-18 mmHg | Vascular redistribution on CXR; early interstitial edema risk |
| 18-25 mmHg | Frank interstitial edema (Kerley lines, peribronchial cuffing) |
| > 25 mmHg | Alveolar edema (bat-wing opacities, air bronchograms) |
| > 30 mmHg | Severe alveolar flooding |
This is the basis of the stage-based CXR classification discussed earlier.
A PCWP > 18 mmHg is the traditional threshold used to define cardiogenic (hydrostatic) pulmonary edema, as opposed to non-cardiogenic causes (ARDS, HAPE) where PCWP is typically normal (≤ 15 mmHg). - Fishman's Pulmonary Diseases and Disorders; Harrison's Principles
The Pressure Cascade: CVP → PCWP → LVEDP
Right atrium (CVP) → Right ventricle → Pulmonary artery
→ [PCWP measured here] ← Pulmonary veins ← Left atrium ← LVEDP
The chain: CVP → RAP → RVEDP → PCWP → PVP → LAP → LVEDP - Barash Clinical Anesthesia
Each step is a valid surrogate only when there is no obstruction or abnormal resistance between the measurement site and the target chamber.
PCWP vs. LVEDP - When They Diverge
PCWP overestimates LVEDP (PCWP > LVEDP):
- Positive pressure ventilation / PEEP (compresses pulmonary vessels, raises PCWP)
- Catheter tip in West Zone I or II (non-zone III placement - most important technical error)
- COPD / increased pulmonary vascular resistance
- Mitral stenosis or left atrial myxoma
- Increased intrathoracic pressure
PCWP underestimates LVEDP (PCWP < LVEDP):
-
Non-compliant LV (LV hypertrophy, ischemia) - diastolic dysfunction
-
Aortic regurgitation (premature mitral valve closure)
-
LVEDP > 25 mmHg (the mitral valve closes before full LV filling)
-
Miller's Anesthesia, 10th Edition
West Lung Zones - Why This Matters for Accuracy
PCWP is only valid when the catheter tip is in West Zone III (where PA pressure > pulmonary venous pressure > alveolar pressure), ensuring continuous blood flow and an uninterrupted fluid column to the left atrium.
- In zones I and II, alveolar pressure may exceed venous pressure, collapsing the vessels and interrupting the fluid column - making PCWP reflect alveolar pressure, not LAP.
- Tip position in non-zone III is suspected when: PCWP > PA end-diastolic pressure, or the PCWP tracing is non-phasic. - Barash Clinical Anesthesia; Murray & Nadel's
Key Uses
- Diagnosing cardiogenic vs. non-cardiogenic pulmonary edema - PCWP > 18 = cardiogenic; PCWP ≤ 15 with hypoxia = ARDS/non-cardiogenic
- Assessing LV preload and guiding fluid management in critical care
- Differentiating causes of shock (cardiogenic vs. distributive vs. obstructive)
- Right heart catheterization for pulmonary hypertension - PCWP > 15 defines post-capillary PH (WHO Group 2)
- Guiding hemodynamic optimization in perioperative patients
Note: Despite its physiologic elegance, routine PAC use has not been shown to improve outcomes in most ICU populations. Its use is now reserved for specific situations where the hemodynamic question cannot be answered by less invasive means. - Miller's Anesthesia; Barash Clinical Anesthesia
Sources: Miller's Anesthesia, 10e | Barash Clinical Anesthesia, 9e | Fishman's Pulmonary Diseases and Disorders | Harrison's Principles of Internal Medicine, 22e | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.