Show me tough ECG and prominent finding
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have a comprehensive collection of real ECG images and detailed textbook content. Let me compile the full answer.
Tough ECGs: High-Yield Patterns with Prominent Findings
Source: ROSEN's Emergency Medicine, Washington Manual of Medical Therapeutics
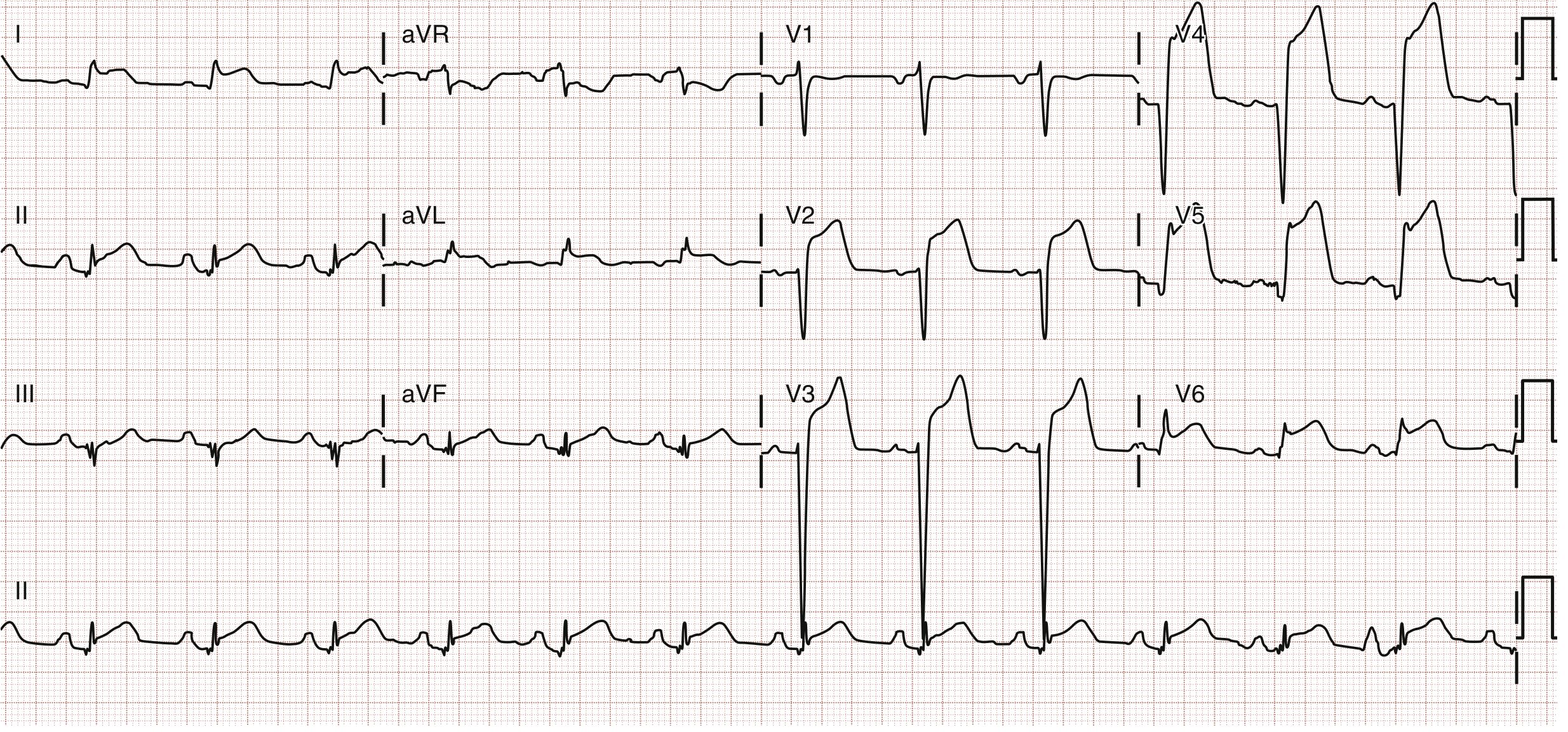
1. Anterior STEMI (LAD Occlusion)
Finding: ST elevation in V1-V4, obliquely straight or convex morphology.
Key diagnostic criteria (4th Universal MI Definition):
- Men >40 yrs: STE ≥2 mm in V2-V3, >1 mm elsewhere
- Men <40 yrs: STE >2.5 mm in V2-V3
- Women: STE >1.5 mm in V2-V3, >1 mm elsewhere
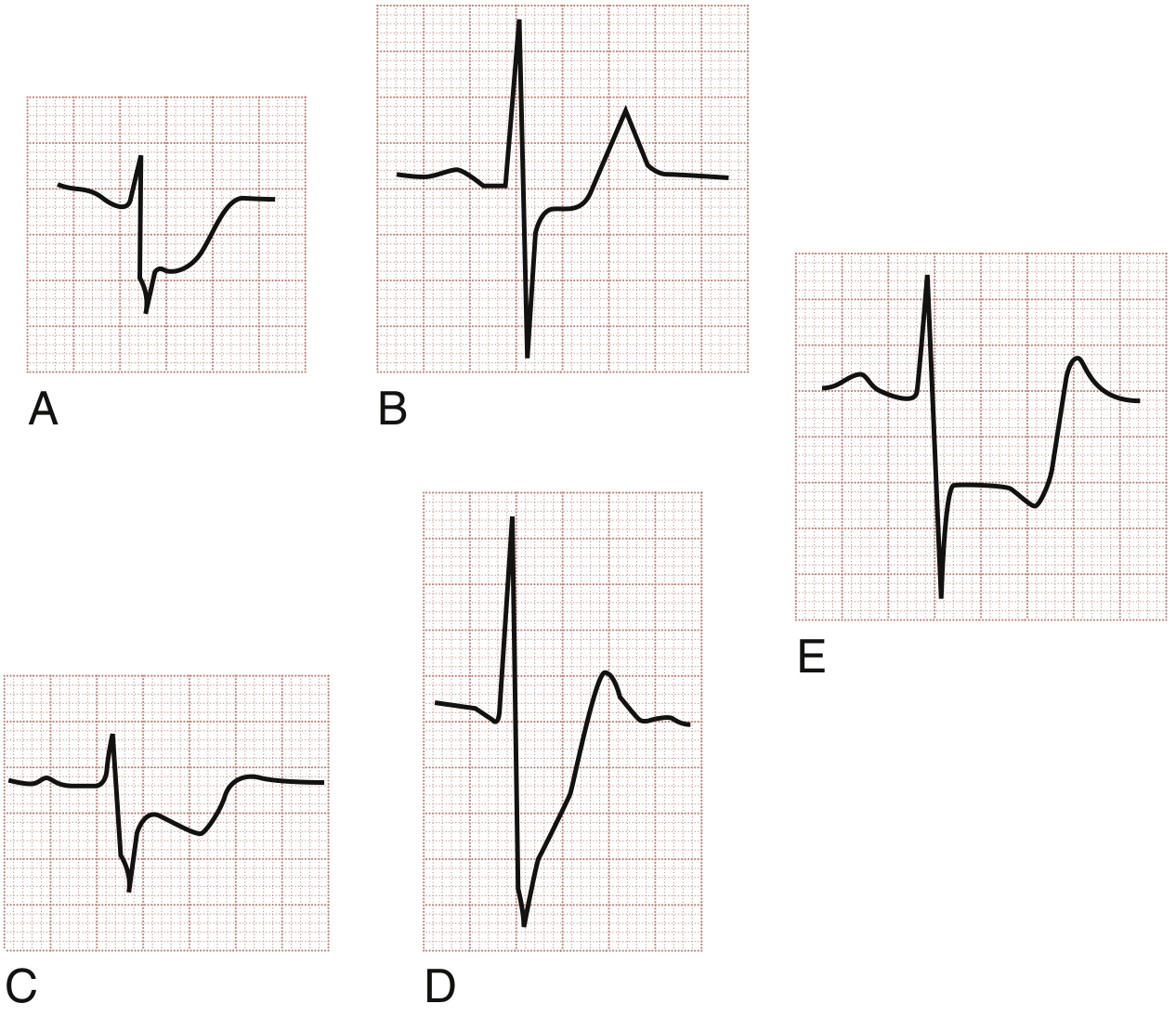
Pitfall: The very first ECG finding is the hyperacute T wave - tall, broad-based, asymmetric, appearing within minutes of occlusion. It precedes STE and is easy to miss.
2. Anterolateral STEMI (Proximal LAD / Left Main)
Finding: STE in V1-V6 + I + aVL, representing massive territory at risk.
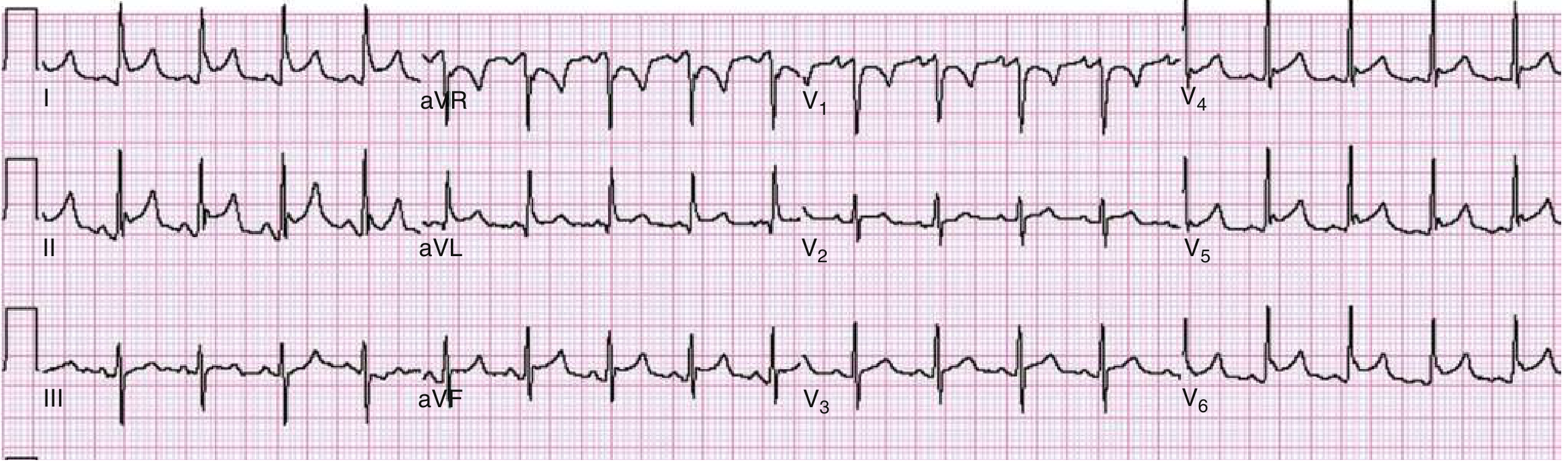
3. aVR STE - Left Main / Proximal LAD Occlusion
Finding: ST elevation in aVR >1 mV with widespread ST depression across other leads.
STE in aVR >0.5 mV is ~78% sensitive, 83% specific for left main disease. Greater aVR elevation than V1 elevation favors left main; greater V1 elevation favors proximal LAD.
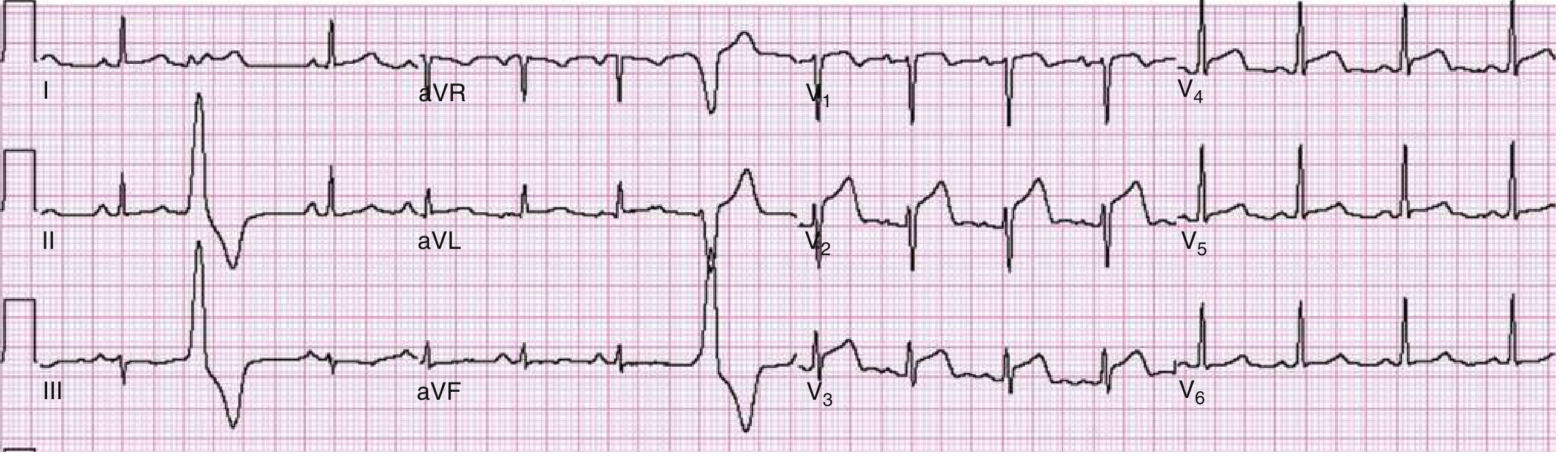
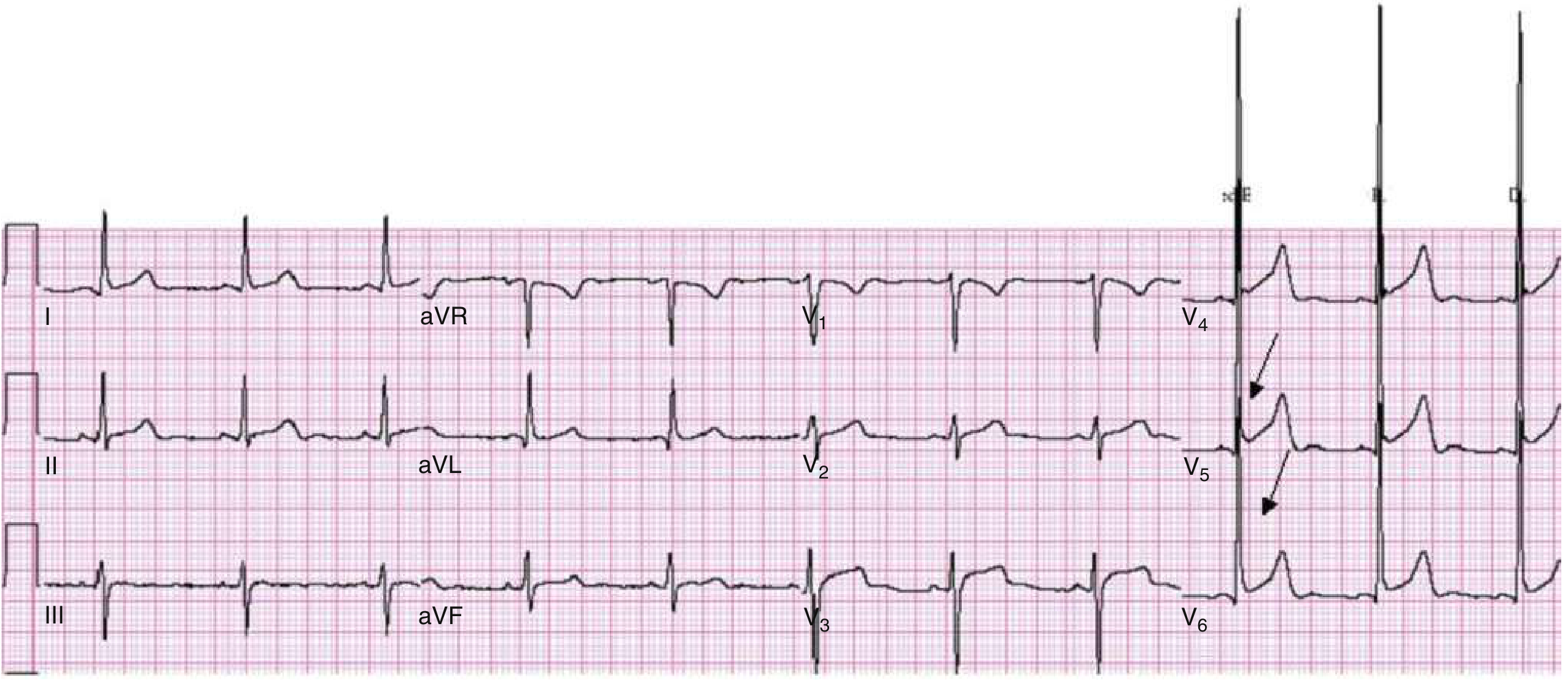
4. Wellens Syndrome (Pre-Infarction LAD Pattern)
Finding: Deep symmetric T wave inversions (Type I) or biphasic T waves (Type II) in anterior precordial leads V2-V3, with isoelectric or minimally elevated (<1 mm) ST segments and no Q waves.
Why it's tough: The patient may be pain-free when the ECG is obtained, making it easy to dismiss. This pattern indicates a critical proximal LAD stenosis - the natural history is progression to anterior STEMI. Do NOT stress test these patients.
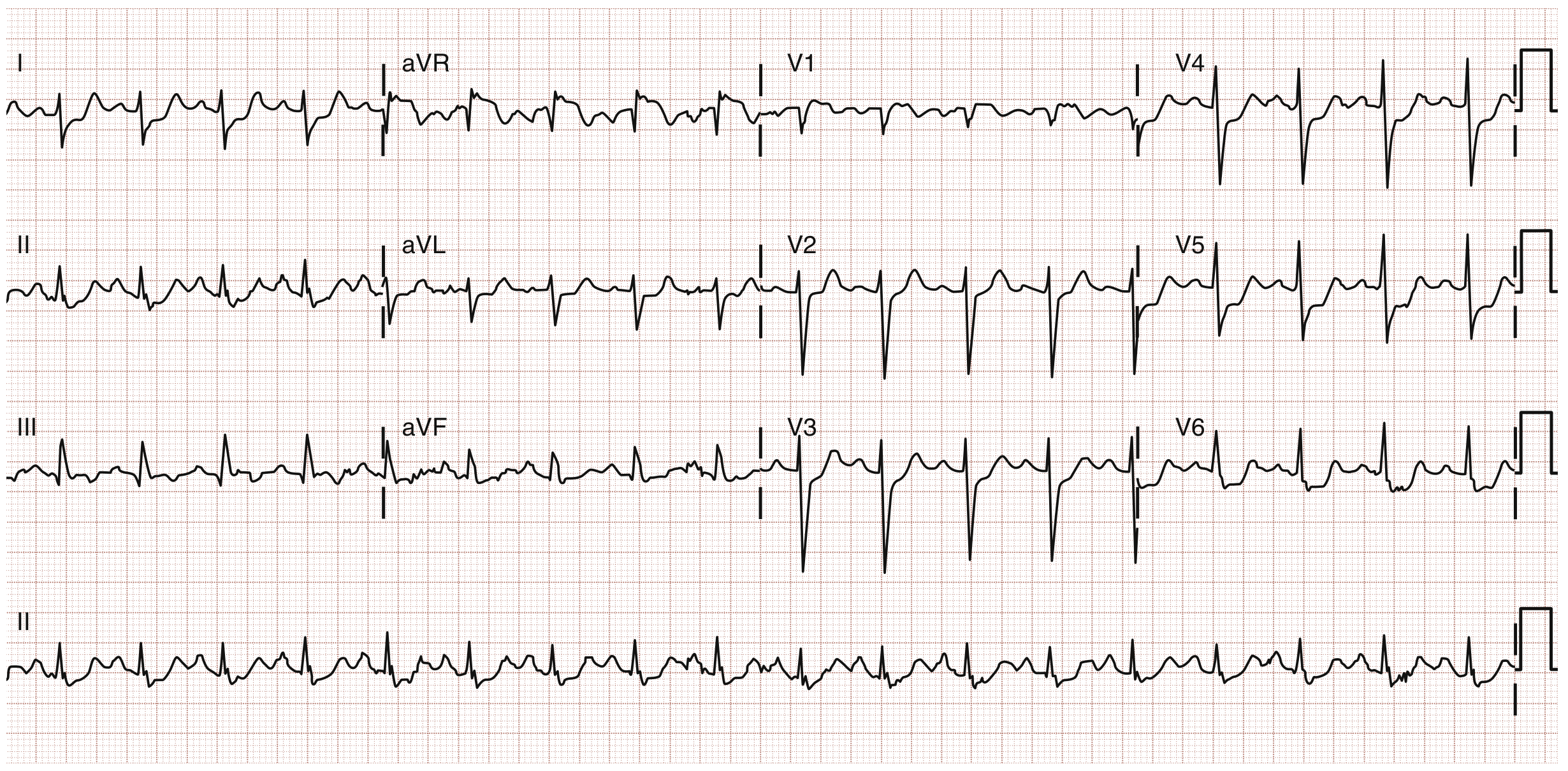
5. De Winter ECG Pattern (STEMI Equivalent)
Finding: J-point depression + upsloping ST depression in precordial leads + tall, prominent (hyperacute) T waves + ST elevation in aVR.
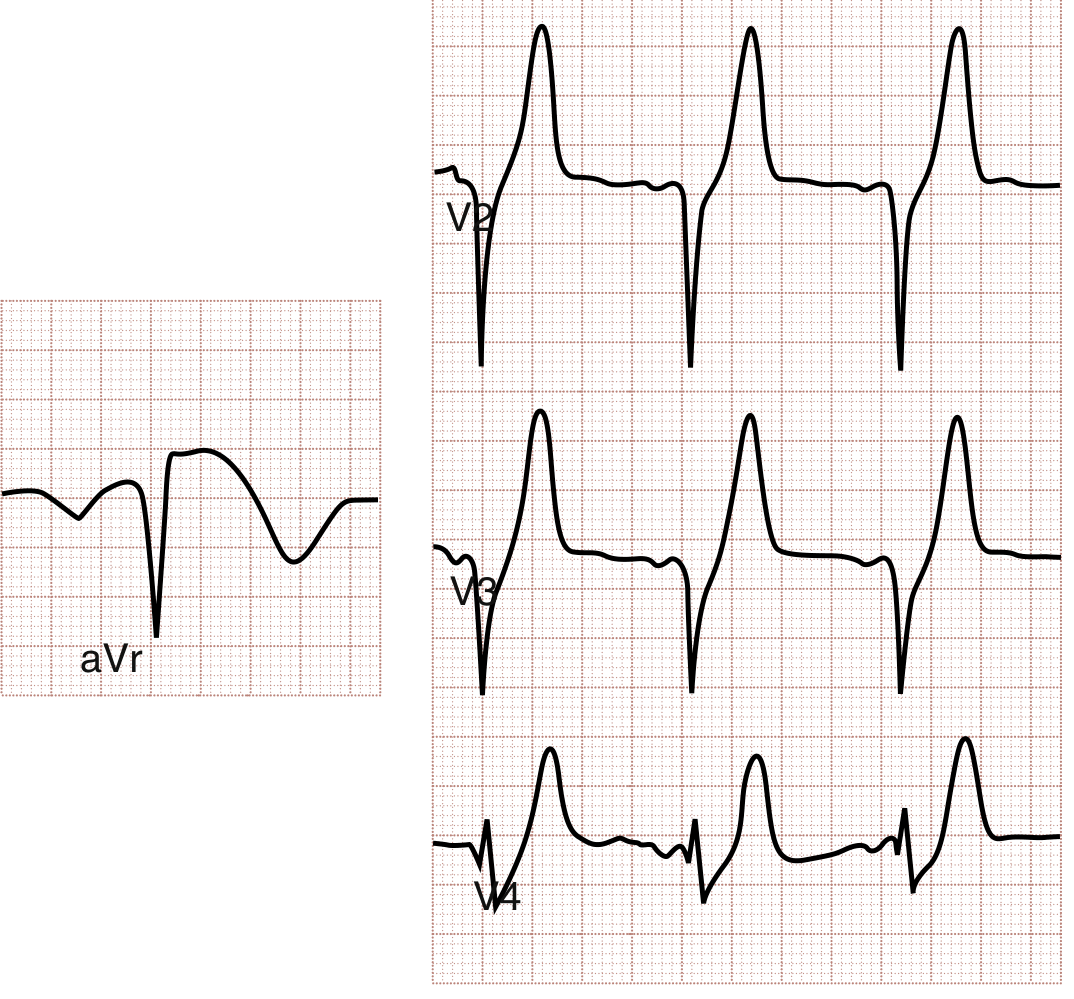
Why it's tough: This pattern doesn't show classic STE, so it often goes unrecognized. It is a STEMI equivalent - treat with emergent PCI. Associated with proximal LAD occlusion, same territory as anterior STEMI.
6. Pericarditis vs. STEMI
Finding: Diffuse concave-upward ("saddle-shaped") STE + PR depression in most leads + PR elevation in aVR + sinus tachycardia.
Distinguishing features from STEMI:
| Feature | Pericarditis | STEMI |
|---|---|---|
| STE distribution | Diffuse (multiple territories) | Regional (contiguous leads) |
| ST morphology | Concave upward | Flat/convex/oblique |
| PR depression | Present (most leads) | Absent |
| Reciprocal STD | Absent (except aVR) | Present |
| Q waves | No | Develop over time |
7. Benign Early Repolarization (BER) vs. STEMI
Finding: Concave-upward STE best seen in V4-V6, relatively large T waves in same leads, subtle J-point notching.
The trap: BER can mimic anterior STEMI. Key differentiators: the STE is stable on serial ECGs, concave morphology, and absence of reciprocal changes.
8. Brugada Syndrome
Finding: Downward coved (Type 1) or saddleback (Type 2) ST elevation in V1-V3, sometimes simulating RBBB morphology. May be transient or unmasked only by sodium channel blockers (ajmaline, flecainide), fever, or vagotonic states.
Clinical context: Young male + unexplained syncope + Brugada pattern = admit for ICD evaluation. Inherited Na+ channelopathy causing ventricular fibrillation and sudden cardiac death without structural heart disease.
Differential for STE in V1-V3: Brugada, RBBB, anterior STEMI, RV strain, Hyperkalemia, Na+ channel drug toxicity.
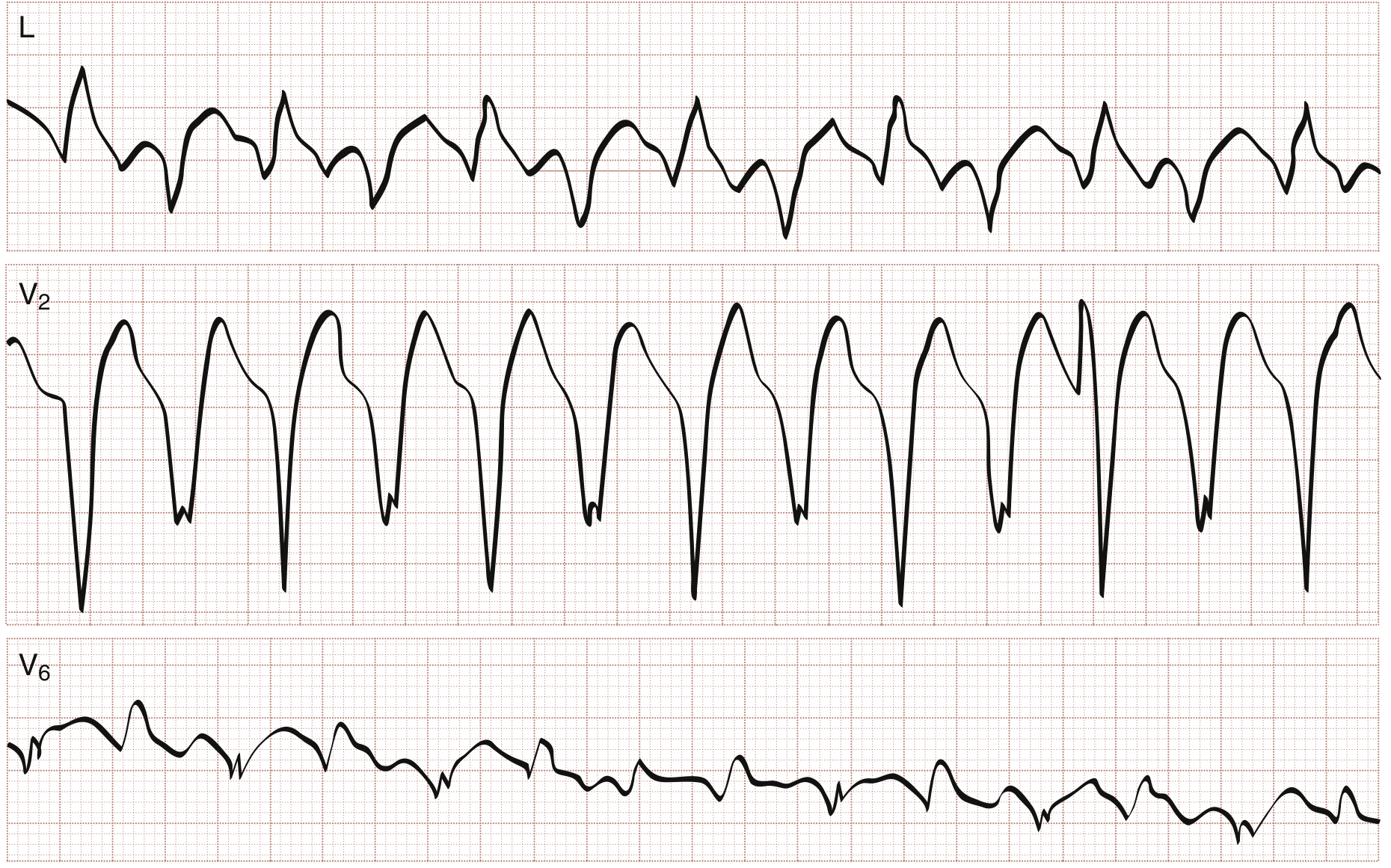
9. Ventricular Tachycardia vs. SVT with Aberrancy
Finding: Wide-complex tachycardia. Brugada VT criteria (4-step algorithm):
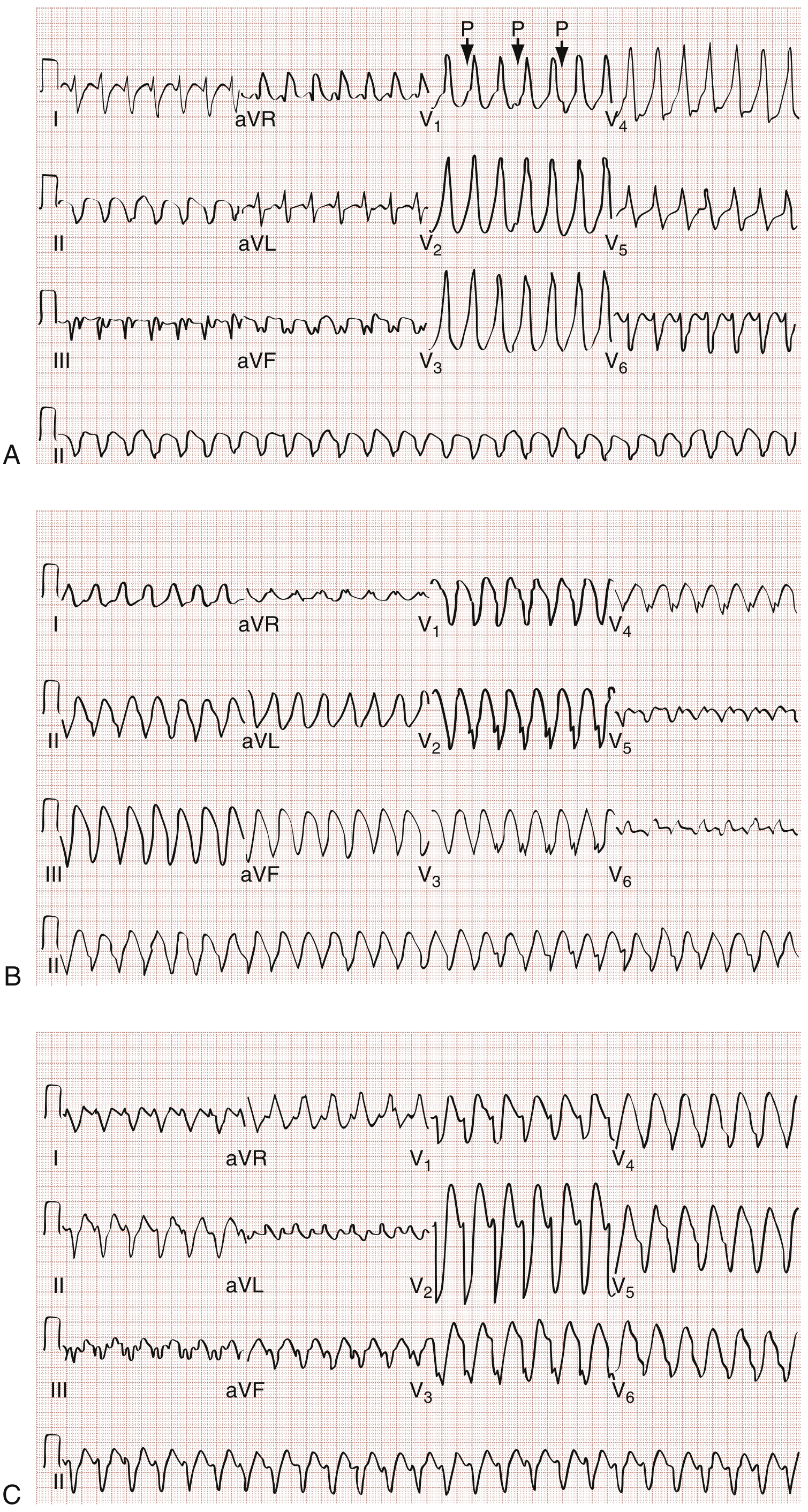
Step 1: No RS complex in any chest lead? → VT
Step 2: RS interval >100 ms in any chest lead? → VT
Step 3: AV dissociation present? → VT
Step 4: Morphologic criteria in V1 and V6 consistent with VT?
Bidirectional VT (alternating QRS axis beat-to-beat) = classic for digoxin toxicity or catecholaminergic polymorphic VT (CPVT):
10. Torsades de Pointes
Finding: Polymorphic VT with characteristic twisting of QRS complexes around the isoelectric baseline ("turning of the points"), preceded by prolonged QT.

Treatment: IV magnesium sulfate 1-2 g rapidly (even without confirmed hypomagnesemia). Overdrive pacing at 100-120 bpm for acquired (pause-dependent) forms. Beta-blockers for congenital (adrenergic-dependent) forms.
Causes (Acquired): QT-prolonging drugs (class IA/IC antiarrhythmics, macrolides, haloperidol, TCAs, azoles), hypokalemia, hypomagnesemia, severe bradycardia.
Quick Reference: Anatomic STEMI Localization
| ST Elevation Leads | Territory | Culprit Artery |
|---|---|---|
| V1-V2 | Septum | Proximal LAD / septal branch |
| V2-V4 | Anterior wall | LAD |
| V5-V6 | Lateral wall | LCX |
| II, III, aVF | Inferior wall | RCA (90%) or LCX |
| I, aVL | High lateral | Diagonal or proximal LCX |
| V1-V6 + LBBB | Anterior + septal | Proximal LAD or left main |
| aVR + diffuse STD | Left main / proximal LAD | Left main / LAD |
Sources: ROSEN's Emergency Medicine 9e (Ch. 64-65), Washington Manual of Medical Therapeutics
Am loving the info
This is a shared conversation. Sign in to Orris to start your own chat.